Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2024
The Clinical Attachment Revisited: A Clinical Opinion Introducing the (A-LEVEL), (A-GAIN), and (A-LOSS)
Aous Dannan*
Professor of Periodontology, Department of Periodontology, Faculty of Dentistry, The International University for Science and Technology, Damascus, Syria
*Corresponding Author: Aous Dannan, Professor of Periodontology, Department of Periodontology, Faculty of Dentistry, The International University for Science and Technology, Damascus, Syria; Tel: 00963 933300 485; Email: [email protected]
Received Date: February 20, 2024
Publication Date: March 15, 2024
Citation: Dannan A. (2024). The Clinical Attachment Revisited: A Clinical Opinion Introducing the (A-LEVEL), (A-GAIN), and (A-LOSS). Mathews J Dentistry. 8(1):44.
Copyright: Dannan A. © (2024)
ABSTRACT
The diagnosis of periodontal diseases usually requires resorting to several clinical indicators such as the probing depth, the gingival recession, and the amount of loss of attachment. However, the terminology used in describing the latter, and the measurements made to record it have led to confusion. This paper attempts to introduce new diagnostic terms to prevent some of the confusion that existed in the field of recording the so-called (clinical attachment loss) or (clinical attachment level). The “attachment level” (A-Level), the “attachment loss” (A-Loss), and the “attachment gain” (A-Gain) are new terminologies suggested as alternatives to some existing ones. Furthermore, essential calculations are demonstrated as new formulas to make periodontal diagnosis easier for clinicians, specialists, and non-professionals (e.g., dental students). Committing to these new suggested terminologies and formulas that are demonstrated in this paper would ensure unity in terms of periodontal diagnosis and research terminologies.
Keywords: periodontal diagnosis, attachment level, attachment loss, attachment gain
INTRODUCTION
Periodontitis is a chronic, multifactorial, inflammatory disease in which plaque bacteria and the body's defense mechanisms play an important role in its development and severity [1].
In the context of diagnosing periodontal diseases, several indicators (i.e., indices) are used to give an illustrative picture of the disease's effectiveness and the extent of its impact on periodontal tissues. Among these indicators, the measurement of the periodontal pocket, or the so-called probing depth (PD), and the amount of clinical attachment loss (CAL) are two important indicators in the field of periodontal diagnosis.
The periodontal pocket develops as a natural result of the progression of the periodontal disease deeply in an apical direction, which includes the activation of specific inflammatory mechanisms arising from the infiltration of dental plaque bacteria and their products from the surface of the tooth into the gingival connective tissue through the epithelial lining of the natural gingival crevice, and this results in the destruction of collagen fibers in the connective tissue. With the rise of inflammatory infiltration in the gingival tissue and the filling of the lining epithelium with defensive cells, the separation of epithelial tissue from the surface of the tooth begins and the apical parts of it multiply, and thus a complete shifting of the attachment toward an apical direction takes place which, in turn, leads to the formation of a periodontal pocket as a primary result.
BODY
Confirmation of the presence of a periodontal pocket, usually utilizing a periodontal probe, is an important indication of the presence of a periodontal disease [2]. The depth of the periodontal pocket is measured from the free gingival margin to the deepest point inside the pocket [3], which corresponds with the place of attachment of periodontal tissues on the surface of the tooth, and it expresses, in one way or another, the severity of the periodontal disease, exclusively when it exceeds 3mm (e.g. in cases of periodontitis) (Figure 1).
The reliance on measuring PD to determine the degree of tissue destruction around the tooth is a matter of clinical misconception due to two important reasons; firstly, the pocket that is diagnosed may be a "false" pocket (i.e., pseudo pocket) caused by gingival enlargement, and secondly, the measurement of the pocket depth depends on a non-fixed point to start from, which is the gingival margin. For instance, we can encounter a case of an entire recession of the periodontal attachment without exceeding 3 mm as a probing depth around a tooth or a set of teeth, and here, it is not correct to state that a remarkable loss of periodontal tissues does not exist.
Another important and effective diagnostic tool in periodontal diagnosis is the measurement of the so-called “amount of clinical loss of attachment” or “the clinical attachment loss” abbreviated in most references as CAL. However, sometimes a malpresentation occurs when using the same abbreviation when talking about the “clinical attachment level” or the “level of clinical attachment”.
According to scientific references, CAL is measured from a fixed point on the tooth surface to the deepest point in the periodontal pocket [4]. Hence, the cemento-enamel junction (CEJ) line was chosen as a reference level for this measurement, considering that it is a fixed anatomical point on the tooth surface and its location does not change (Figure 2).
Clinical attachment loss is measured as a diagnostic indicator of the severity of periodontal tissue damage and its regression due to periodontal disease. The use of this measurement was also approved to express the amount of the gain of periodontal attachment of teeth after completion of different periodontal treatments (e.g., regenerative periodontal procedures).
Sometimes confusion arises when talking about the “clinical attachment level” as the same term expressing the amount of “clinical attachment loss”, both abbreviated as CAL.
The 2018 Classification of Periodontal and Peri-implant Diseases and Conditions describes periodontitis by severity, extent, and rate of progression [5]. Here, interdental clinical attachment loss determines the assignment of staging any periodontal case.
As for the term “clinical attachment level”, we suggest that it can be replaced by the term “Attachment Level” (A-LEVEL) only to denote the point where the anatomical part of the periodontium is attached to the tooth (Figure. 3), thus, in a normal periodontium, it is a non-measurable term referring to the area where the junctional epithelium is located on the tooth surface (i.e. the CEJ). However, in cases of periodontal destruction and the following apical shifting of periodontal attachment, the location of (A-LEVEL) changes and would be detected in a more apical point regarding the CEJ.
In our opinion, the term “clinical attachment loss” should be used only when talking about the regression of periodontal tissues, specifically the regression of the whole periodontal attachment system (i.e., the connective attachment and epithelial attachment), from the anatomical tooth neck (i.e., the CEJ), where the measurement of probing clinically begins to exceed 3 mm. Such cases are usually seen in the course of periodontitis, in a healed periodontium, or a reduced-but-healthy periodontium. Accordingly, we suggest the term “Attachment Loss” (A-LOSS) to refer to those cases. Moreover, there is no need for the word “clinical” since there is neither “non-clinical” nor even “theoretical” attachment loss.
We believe that a distinction must also be made between what we propose to call “pathological A-LOSS” and “non-pathological A-LOSS”. The first term expresses an apical shifting of A-LEVEL due to periodontal disease (with or without accompanying gingival recession), and the second term expresses an apical shifting in A-LEVEL due to reasons that cannot be attributed to periodontal disease, such as retraction of periodontal tissues due to traumatic tooth brushing, cervical caries, and fractures, etc... Accordingly, we recommend that, when performing a complete periodontal diagnosis using a diagnostic chart, the “cause of gingival recession” should also be highlighted.
Another suggested term would be the “Attachment Gain” (A-GAIN), which refers to the amount of the gain of periodontal attachment of teeth after completion of different periodontal treatments resulting in a recovery of the periodontium (e.g., regenerative periodontal procedures).
Essential calculations and formulae
To calculate how much did we gain, as recovered periodontium, after an effective periodontal treatment; the following formula applies:
A-GAIN = [A-LEVEL] (before treatment) – [A-LEVEL] (after treatment)
In such cases, the marginal part of a fabricated acrylic stent that is rested on the related teeth could be a favorable reference point to calculate the measurements mentioned above [5,6].
To calculate the amount of A-LOSS, the following formula applies:
A-LOSS = PD + GR
where PD is the probing depth, and GR is the amount of gingival recession. Both are measured utilizing a calibrated periodontal probe (Figure 4).
Here, most of the ambiguities begin in the absence of an accompanying gingival recession, and therefore, the A-LOSS would be thought to result as:
A-LOSS = PD
and the amount of A-LOSS becomes equal to the measurement of probing depth (i.e., the depth of the periodontal pocket). However, this measurement misrepresents what is needed.
According to references, the origins of dealing with those cases in which the gingival recession is absent or “hidden”, or when, in other words, the A-LOSS is caused only by the presence of a periodontal pocket without being associated with gingival recession, depend on measuring how much did the A-LEVEL recede concerning the cemento-enamel junction. However, such measurement is practically not possible because the examiner is not able to see the anatomical parts that are covered by the gingiva.
In 1988, Griffiths et al. [7] modified the method of CAL measurement presented previously by Ramjord (1955) to minimize the errors that could occur [8]. In their paper, they suggested measuring the space from the gingival margin to the base of the crevice, rounding the record to the minimum millimeter, and thereafter, observing, to the nearest millimeter, the amount of the probe withdrawn from the pocket until the CEJ is detected. This gives a direct measurement rather than one derived from computation. It is possible to make similar measurements on the way into the crevice rather than on the way out as described, and this will be a matter of individual preference (Figure 3). However, in our opinion, though it seems to be advantageous over other methods, using this method to measure CAL may encounter a critical problem since detecting CEJ with the probe needs further experience and could be difficult when non-professionals (e.g., dental students) are in charge. A similar problem was also reported by Badersten et al. in 1984 [9]. Moreover, the most suitable periodontal probe to achieve that method would be the one that has a small ball on its tip (e.g., WHO probe or CP-12s probe) so that an acceptable sensation is guaranteed.
We believe that, when A-LOSS is to be measured in a case where no gingival recession but only a pathological pocket is present, the original sulcus depth (OSD) has to be known, and therefore, the following suggested formula applies:
A-LOSS = PD – OSD
However, although the amount of OSD relies upon the range of [1-3mm] for a healthy sulcus, we do not know exactly what it could be before a periodontal pocket has formed, which may still be debated.
Therefore, to calculate the attachment loss, the general formula for all cases would be as follows:
A-LOSS = [PD – OSD] + GR
This formula is suggested as a universal one to be applied in all cases and all situations regardless of the relation between gingival margin and CEJ.
SUMMARY
In 2022, Van der Velden, in his letter to the editor, suggested that in the Instructions for Authors section of the J Clin Perio, a sentence may be added stating that when CAL is included in clinical studies, they should provide a clear description of how CAL measurements were obtained, taking into account the location of the gingival margin relative to the cemento-enamel junction or a fixed reference point [10].
Terms such as attachment loss, attachment level, and loss of attachment have long been used synonymously. Therefore, new terminologies are introduced in this paper including the (A-LEVEL), which refers to the anatomical point where the junctional epithelium is located, the (A-LOSS), which refers to the amount of receded periodontal attachment with or without gingival recession, and the (A-GAIN), which refers to the amount of gained periodontal attachment after effective periodontal treatment.
During full periodontal diagnosis, a clinician could face one of the following scenarios when asked to calculate A-LOSS;
- Scenario #1: a probing depth that is concomitant with healthy periodontium (i.e., one to three millimeters). Here, (A-LOSS) does not exist. It is a healthy case.
- Scenario #2: a probing depth that is concomitant with a real pathological pocket (i.e. more than or equal to 4mm) with obvious gingival recession. Here, A-LOSS = PD + GR
- Scenario #3: a probing depth that is concomitant with a real pathological pocket (i.e. more than or equal to 4mm) without obvious gingival recession. Here, A-LOSS = PD – OSD
As explained earlier, both scenarios #2 and #3 can be engaged together in the suggested universal formula: A-LOSS = [PD – OSD] + GR
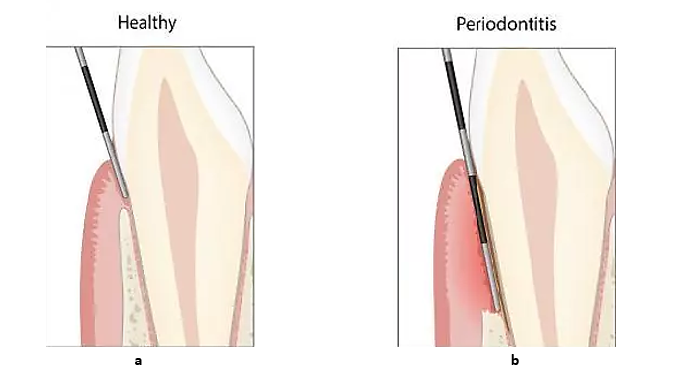
Figure 1: Probing depth screens the periodontal tissues’ status. (a): Healthy tissues due to a probing depth of less than 3mm. (b): Diseased tissues (i.e., periodontitis) due to a probing depth of more than 3mm.
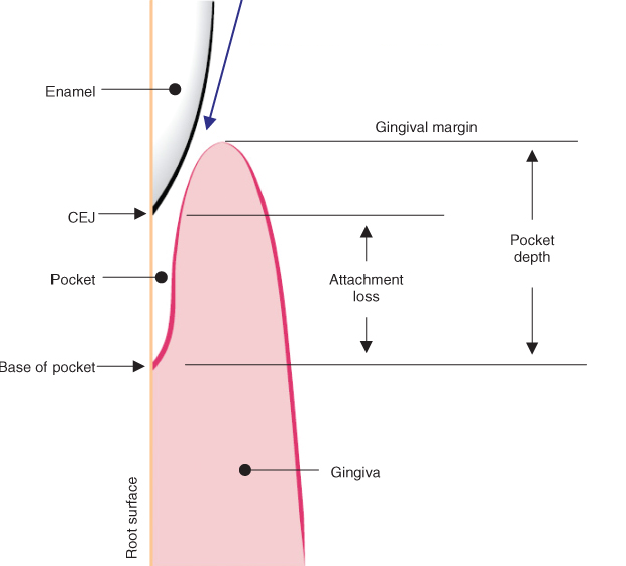
Figure 2: Distinction of the clinical attachment loss concerning PD.
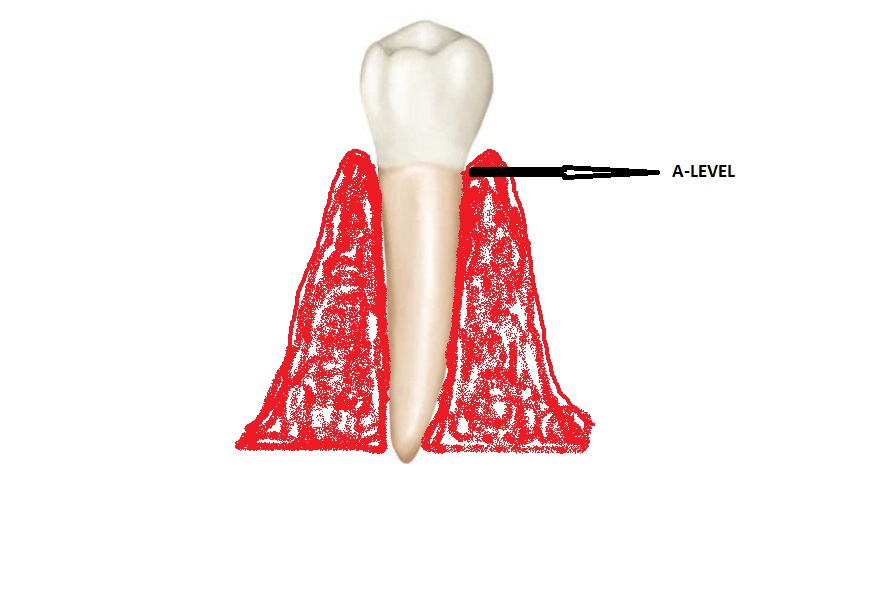
Figure 3: A-Level is the point where the anatomical part of periodontium connects to the tooth.
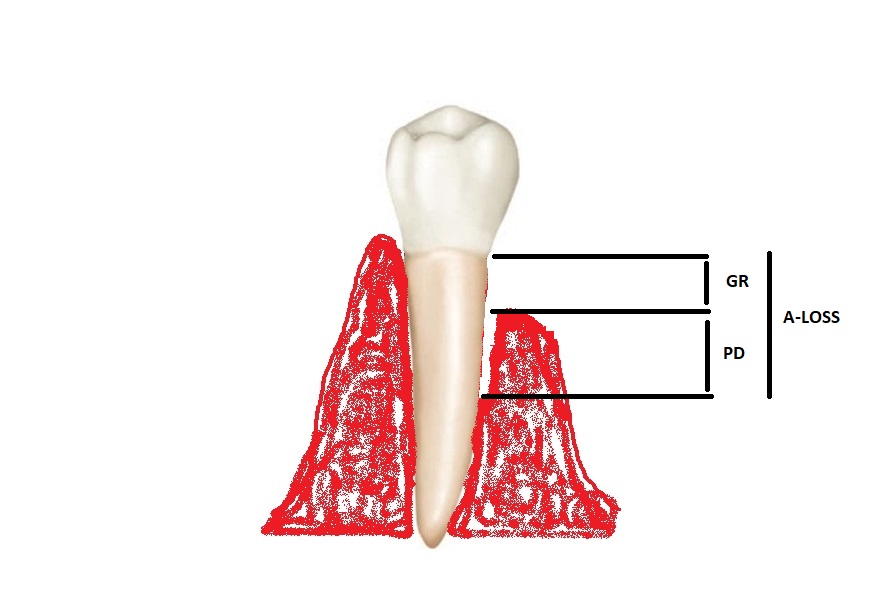
Figure 4: A-LOSS is calculated by adding an obvious gingival recession to the pocket depth [11].
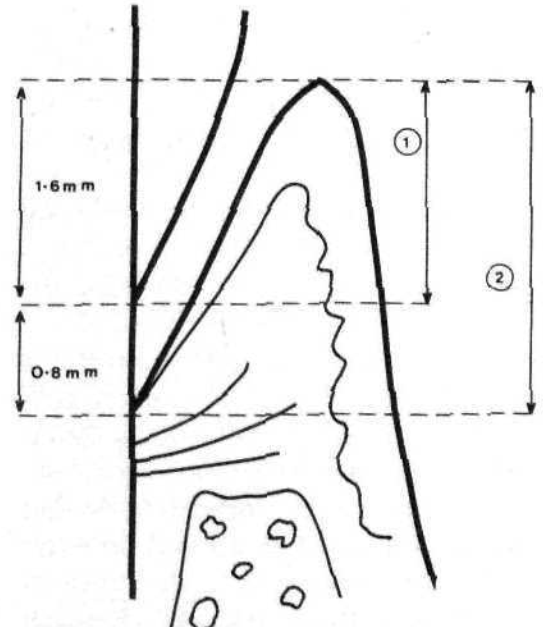
Figure 5: Measurements made in the detection of attachment level when the gingival margin extends onto the enamel (1): cemento-enamel junction to the gingival margin, and (2): gingival margin to the base of the pocket.
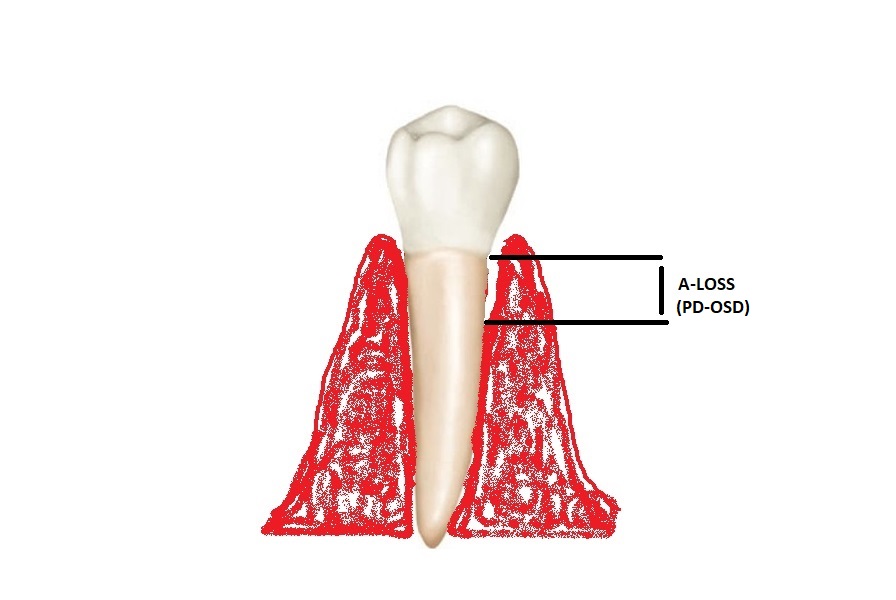
Figure 6: When no GR is obvious, A-LOSS is calculated by subtracting OSD from PD.
Acknowledgments
N/A
REFERENCES
- Chapple IL, Mealey BL, Van Dyke TE, Bartold PM, Dommisch H, Eickholz P, et al. (2018). Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri‐Implant Diseases and Conditions. J Periodont. 89:S74-S84.
- Listgarten MA. (1980). Periodontal probing: what does it mean? J Clin Perio. 7(3):165-176.
- Wei SH, Lang KP. (1981). Periodontal epidemiological indices for children and adolescents: I. Gingival and periodontal health assessments. Pediatr Dent. 3(4):353-360.
- Feldman RS, Dpurlass CW, Loftus ER, Kapur KK, Chauncey HH. (1982). Interexaminer agreement in the measurement of periodontal disease. Journal of Periodontal Research. 17(1):80-89.
- Caton JG, Armitage G, Berglundh T, Chapple IL, Jepsen S, Kornman KS, et al. (2018). A new classification scheme for periodontal and peri‐implant diseases and conditions–Introduction and key changes from the 1999 classification. J Periodont. 89:S1-S8.
- Clark WB, Yang MC, Magnussen I. (1992). Measuring clinical attachment: reproducibility of relative measurements with an electronic probe. J Periodont. 63(10):831-838.
- Clark DC, Quee TC, Bergeron MJ, Chan EC, Lautar‐Lemay C, De Gruchy K. (1987). Reliability of attachment level measurements using the cementoenamel junction and a plastic stent. J Periodont. 58(2):115-118.
- Griffiths GS, Wilton JM, Curtis MA, Maiden MF, Gillett IR, Wilson DT, et al. (1988). Detection of high‐risk groups and individuals for periodontal diseases: clinical assessment of the periodontium. J Clin Perio. 15(7):403-410.
- Ramfjord SP. (1959). Indices for prevalence and incidence of periodontal disease. The J Periodont. - deepblue.lib.umich.edu.
- Badersten A, Nilvéaus R, Egelberg J. (1984). Reproducibility of probing attachment level measurements. J Clin Perio. 11(7):475-485.
- Van der Velden U. (2022). On the reliability of clinical attachment level measurements. J Clin Perio. 49(11):1229.