Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2023
Straight Proximal Humeral Nailing Can Avoid Deltoid Atrophy for Proximal Humeral Fracture: A Comparison with Locking Plating
Joong-Bae Seo, Jae-Sung Yoo*, Kyu Beom Kim, Sung-Joon Choi
Department of Orthopaedic Surgery, Dankook University College of Medicine, Cheonan, Korea
*Corresponding author: Jae-Sung Yoo, M.D., Department of Orthopaedic Surgery, Dankook University College of Medicine, Manghyangro 201, Dongnam-gu, Cheonan, Chungnam 330-715, Republic of Korea; Tel: 82-41-550-3060; Fax: 82-41-556-3238; E-mail: [email protected]
Received Date: December 21, 2022
Publication Date: January 4, 2023
Citation: Joong-Bae Seo, et al. (2023). Straight Proximal Humeral Nailing Can Avoid Deltoid Atrophy for Proximal Humeral Fracture: A Comparison with Locking Plating. Orthop Res J. 5(1):25.
Copyright: Joong-Bae Seo, et al. © (2023)
ABSTRACT
Background: Open reduction and plate fixation are the main surgical treatment methods for proximal humeral fracture. However, it is difficult to avoid iatrogenic deltoid insertion injuries while ensuring a proper plate position. We aimed to compare the deltoid muscle volume in treating proximal humerus fractures using the locking compression plate (LCP) and intramedullary (IM) nail fixation methods. Methods: Fifty-two consecutive patients who underwent surgical fixation for proximal humerus fractures were included in the present study. The participants were divided into two groups: the LCP fixation group and the straight IM nail fixation group. Results: No statistically significant differences were detected in the clinical outcomes between these groups. In the 12th week postoperatively, the union rate was much higher in the IM nail group (87.5%) than that in the LCP group (78.5%; p = 0.011). The deltoid volume ratio (%) was significantly higher in the IM nail group (97.5%) than in the LCP group (91.2%; p = 0.003). Conclusion: When treating proximal humerus fractures, straight IM nail fixation revealed convincing outcomes; thus, it could be a useful treatment option for early bony union and to avoid iatrogenic deltoid insertion injuries compared to LCP fixation.
Level of evidence: Level III, retrospective study.
Keywords: Proximal humeral fracture, Locking plate fixation, Intramedullary fixation, Deltoid
INTRODUCTION
However, it is still challenging to determine the most efficacious surgical treatment for proximal humeral fractures. Although various techniques have been reported, there is a lack of agreement regarding the procedures that offer the best clinical outcomes [1-4] Since the development of locking compression plates (LCPs) and screw systems, osteosynthesis using plates has shown promising results in displaced proximal humeral fractures since the development of locking compression plates (LCPs) and screw systems [5]. However, avoiding iatrogenic deltoid insertion injuries while performing appropriate plate positioning is challenging [6].
Humeral nails have evolved significantly and have been developing for over 40 years [7]. Third-generation straight intramedullary nails (IMNs) provide important biomechanical advantages such as higher tolerance for varus, valgus, and torsional loading [8,9]. Theoretically, a straight design of the IMN could maximize the stability of the proximal nail end, resulting in a safe area between the insertion site of the nail in the humeral head area and the fracture line of the lateral head, avoiding unpredictable cracks [9,10]. Moreover, pain in the rotator cuff area and dysfunction can be diminished using third-generation straight nails rather than curvilinear nails because more medial entry points in straight nails avoid the critical hypovascular zone of the rotator cuff [8,9].
We found no in vivo studies that compared deltoid atrophy after surgery for LCP and IMN fixation in proximal humeral fractures. Thus, our primary goal was to evaluate deltoid atrophy after surgery for LCP in proximal humeral fractures compared to straight IMN fixation. The secondary objective was to clarify the differences in radiological and clinical outcomes between these groups. We hypothesized that the clinical outcomes and complications would not differ between the two procedures, but deltoid atrophy in the IMN group would be lower than that in the LCP group.
PATIENTS AND METHODS
This retrospective study, with a control group, was approved by the Research Ethics Committee of this institute. Informed consent was gained by all patients. 52 patients who underwent internal fixation for proximal humerus fractures between May 2017 and December 2021 were included. A shoulder surgeon (J.S.Y.) with >9 years of experience in treating proximal humeral fractures at our institution performed the procedures.
Patients with two-, three-, or four-part fractures were included in this study based on the Neer classification. Patients aged >50 years who had surgical neck fractures and were deemed unstable by a surgeon were included in the study. The following were excluded: patients who had undergone operation using the minimally invasive plate technique or by using allografts such as allo-fibula, who had been diagnosed with large to massive rotator cuff tears, history of pathologic fractures, fractures with irreparable head and/or tuberosity, stable fractures with intact medial support, and immature patients or follow-up loss before 12 months of enrollment. LCP fixation was used in the first 28 cases and IMN fixation was used in the final 24 consecutive cases. Patient data were collected based on medical records, including sex, age, dominant hand, weight, height, American Society of Anesthesiologist classification [8], time to surgery, mechanism of injury, and smoking history.
DESCRIPTION OF THE LCP FIXATION PROCEDURE
Under regional anesthesia, all operations were performed in the sitting position using a deltopectoral approach. A titanium proximal humerus internal locking system (DePuy Synthes, Zuchwil, Switzerland) plate was positioned. After plate positioning, multiple angularly stable locking screws were placed on the humeral head. After fixation, the 3.5-mm cortical screw was loosened from the longitudinal hole of the plate shaft. In 3- or 4-part fractures, rotator cuff tension sutures were performed with four–five non-absorbable sutures (Ethibond, Somerville, NJ, USA). The sutures were then passed around the cortical screw and tied off [Figure 1] [10].



Figure 1: Simple radiographs of a 39-year-old woman who received conventional locking compression plate fixation. (A) Preoperative radiograph showing a displaced proximal humeral fracture. (B) Postoperative radiograph showing fixation with one cortical and two locking screws. (C) A three-month postoperative radiograph showing union at the fracture site.
DESCRIPTION OF THE IMN FIXATION PROCEDURE
The MultiLoc Proximal Humerus Nail (MPHN) (MultiLoc PHN; Synthes GmbH, Solothurn, Switzerland) was used for the IMN fixation procedures. In a 2-part fracture, small splitting of the deltoid muscle and a small incision of the rotator cuff were made after closed fracture reduction. In 3- or 4-part fractures, the deltopectoral approach was used for rotator cuff tension sutures. Under image intensifier control, the medullary canal was engaged just medial to the greater tuberosity of the humerus using an awl. After engaging the guide wire, the humeral canal was reamed using a hand reamer. The nail connected to the targeting device was inserted through the medullary cavity, following the guide wire. Proximal locking was performed by using drill sleeves with cancellous screws in the humeral head. After nail insertion, distal locking was performed by inserting cortical screws into the upper shaft by targeting the sleeves using cortical screws. Finally, the rotator cuff incision was carefully closed with absorbable sutures. In 3- or 4-part fractures, rotator cuff tension sutures were performed with four–five non-absorbable sutures (Ethibond, Somerville, NJ, USA). The suture was then passed around the proximal cancellous screw and tied (Figure 2).

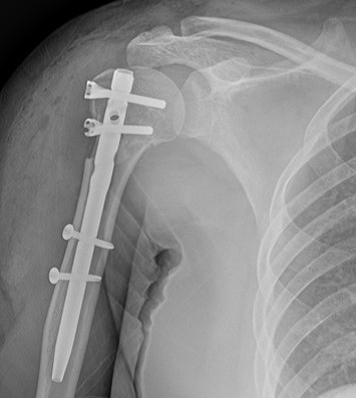
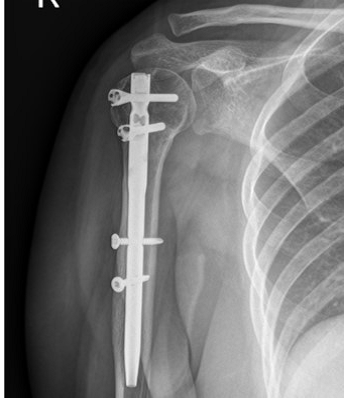
Figure 2: Simple radiographs of a 57-year-old woman who received far cortical locking system fixation. (A) Preoperative radiograph showing a displaced proximal humeral fracture. (B) Postoperative radiograph showing fixation with a straight intramedullary nail fixation. (C) A three-month postoperative radiograph showing union at the fracture site.
POSTOPERATIVE REHABILITATION
After surgery, the surgical site was protected by splint application for one week and then in an abduction sling for the next four weeks. Pendulum exercise, self-assisted circumduction, and incremental passive range of motion (ROM) exercises were initiated 1 week after surgery, if tolerated by the patient. Active ROM exercises were performed four weeks after surgery. Strength exercises were initiated after three months.
CLINICAL AND RADIOLOGICAL EVALUATIONS
Clinical assessments included a constant score, American Shoulder and Elbow Surgeons (ASES) score [11], and ROM at 1 year after surgery. These assessments were recorded by a physician assistant during the final follow-up. Full ROM was collected, and data on abduction, forward flexion, internal rotation, and external rotation were also included. An independent examiner blinded to all the data evaluated the results at each follow-up period.
Radiological evaluation included both clavicular and anteroposterior views taken at regular intervals after surgery (post-operative 3, 6, 12 weeks, 6 months, and 1 year). Union rate, union at 12 weeks, and structural alignment were included as radiological outcomes. The union of the fracture was defined as the existence of a bridging callus in no more than three cortices in two planes. Delayed union was defined as incomplete radiographic consolidation after ≥6 months. The alignment of the fracture site was evaluated immediately after surgery and one year after surgery using the Paavolainen method, which measures the humeral neck-shaft angle (NSA). On anteroposterior radiography, the NSA was determined as an angle between a perpendicular line of the center of the articular surface and another line bisecting the humeral shaft (Figure 3) [12].
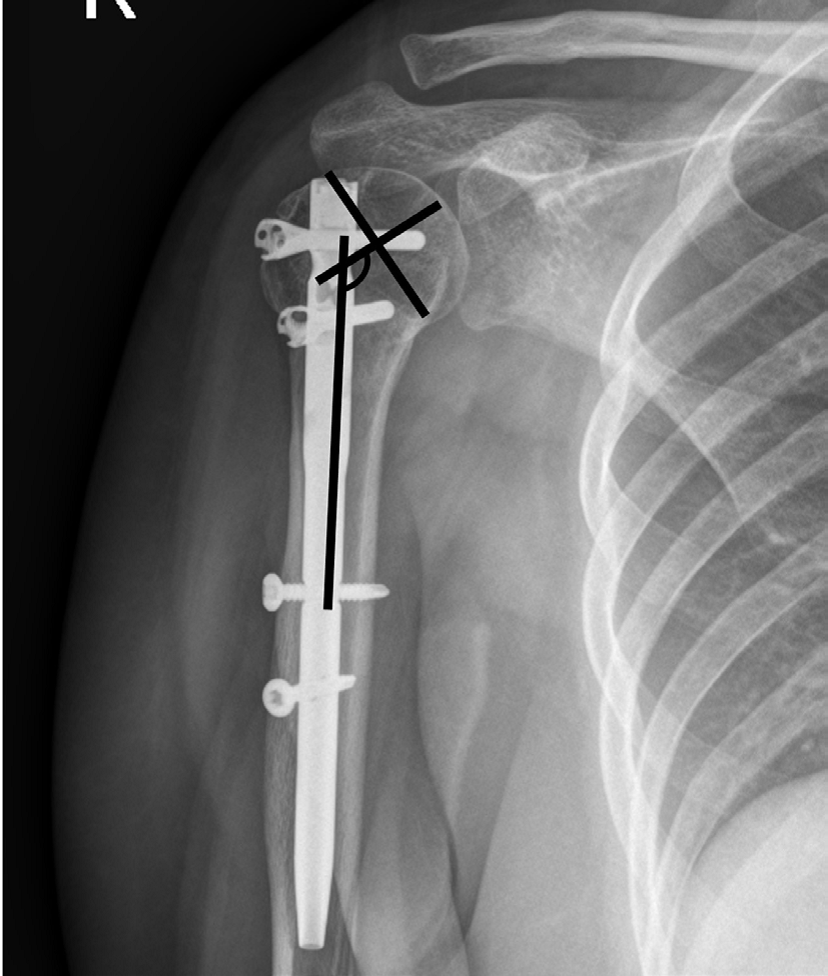
Figure 3: The neck-shaft angle was calculated by the ankle between a perpendicular line of the articular surface center and the line bisecting the humeral shaft was defined as the neck-shaft angle.
For the deltoid muscle volume evaluation, preoperative and l-year postoperative shoulder CT images were used. The deltoid muscle cross-sectional area was measured using axial CT at three positions: the upper edge area, lower edge area, and middle of the glenoid (Figure 4) [10,12]. The mean value of the three positions was calculated for deltoid muscle volume evaluation, and the ratio of the deltoid muscle volume was calculated using the following formula:
Ratio of deltoid volume = 100 × 1 year after deltoid volume/preoperative deltoid volume.
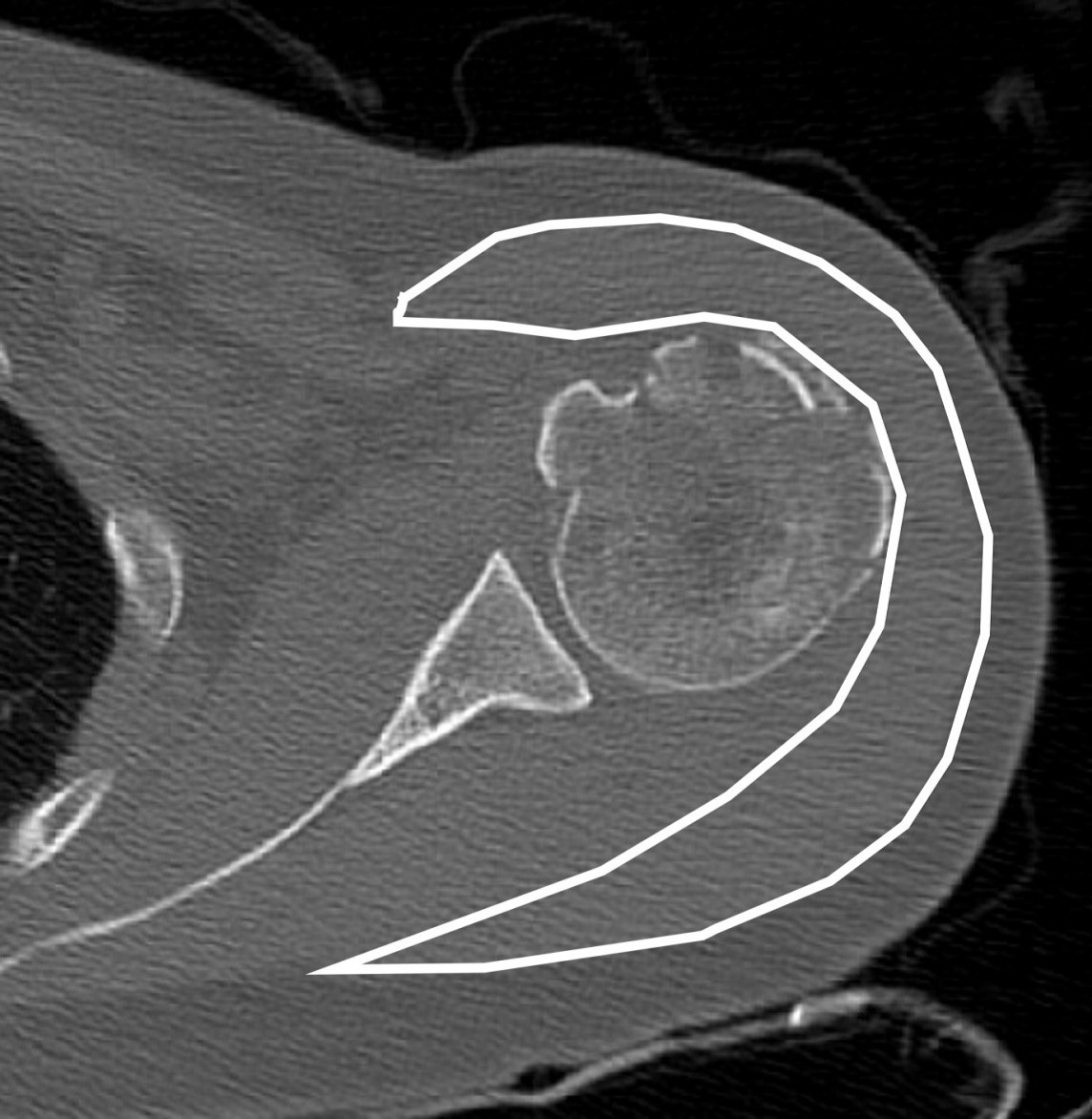
Figure 4: For deltoid muscle volume evaluation, the deltoid muscle cross-section was measured on axial computed tomography.
All radiologic measurements were evaluated by two independent examiners (J.S.Y. and K.B.K.). Individual values were analyzed and the mean numerical values were calculated. All complications, such as fracture collapse, metal failure, screw loosening, infection, avascular necrosis of the humeral head, peri-hardware fracture, shoulder joint stiffness, screw penetration, and resorption or migration of the greater tuberosity, were recorded.
STATISTICAL ANALYSES
The Kolmogorov–Smirnov test was performed for establishing if continuous data were normally distributed. A chi-square and an independent t-test were performed to evaluate continuous and noncontinuous variables, respectively. All statistical analyses were evaluated using Statistical Package for Social Sciences version 25.0 (SPSS, Inc., IBM Co., IL, USA). A p-value of <0.05 represented a statistically significant difference in all the values.
RESULTS
A total of 30 women and 22 men aged 50-87 years were included in the study. The initial injuries were caused by traffic accidents, falls, and sports in 16, 30, and six patients, respectively. No significant differences were found between the two surgical groups in terms of demographic data and time to surgery; however, a significant difference was observed in the mean follow-up period (Table 1).
Table 1: Demographic data.
|
Variable |
Locking plating group (n=28) |
Intramedullary nailing group (n=24) |
p-value |
|
Mean age |
54.2 ± 14.6 |
57.5 ± 17.8 |
0.626 |
|
Gender (Male: Female) |
12 : 16 |
10 : 14 |
0.340 |
|
Dominant arm: Non-dominant arm |
15 : 13 |
11 : 13 |
0.759 |
|
Height (cm) |
161.8 ± 8.7 |
162.4 ± 7.9 |
0.791 |
|
Weight (kg) |
65.2 ± 13.2 |
66.6 ± 14.4 |
0.965 |
|
Smoking: Non-smoking |
7: 21 |
7 : 17 |
0.335 |
|
ASA class (1:2:3) |
11 : 14 : 3 |
7 : 12 : 5 |
0.626 |
|
Mechanism of Injury |
|||
|
Traffic accident Fall Sport injury |
10 15 3 |
6 15 3 |
0.535 |
|
Neer classification (2:3:4) |
6 : 14 : 8 |
7 : 10 : 7 |
0.885 |
|
Time to surgery (day) |
3.4 ± 2.4 |
2.7 ± 2.3 |
0.663 |
|
Mean follow-up (month) |
16.6 ± 6.3 |
15.5 ± 5.1 |
0.389 |
No significant differences were observed in ASES score, constant score, or ROM 1 year after surgery between the two groups. The mean ASES scores were 79.2 ± 18.6 and 80.4 ± 14.8; mean constant scores were 73.3 ± 15.1 and 75.2 ± 12.2; mean forward elevation was 122.8 ± 17.7 and 128.3 ± 16.8, respectively; mean external rotation was 30.0 ± 11.9 and 30.6 ± 11.7°, and mean internal rotation was T10 and T11 in the LCP and IMN groups, respectively (Table 2).
Table 2: Clinical and Radiologic outcomes between the two groups
|
Variable |
Locking Plating group (n=28) |
Intramedullary Nailing group (n=24) |
p-value |
|
ASES score (100) |
79.2 ± 18.6 |
80.4 ± 14.8 |
0.845 |
|
Constant score (100) |
73.3 ± 15.1 |
75.2 ± 12.2 |
0.629 |
|
Range of motion |
|||
|
Forward elevation |
122.8 ± 17.7 |
128.3 ± 16.8 |
0.296 |
|
External rotation |
30.0 ± 11.9 |
30.6 ± 11.7 |
0.878 |
|
Internal rotation |
T10 |
T11 |
0.576 |
|
Union at 12 weeks (%) |
22 (78.5%) |
21 (87.5%) |
0.011 |
|
Neck-shaft angle |
|||
|
Postoperative |
135.9 ± 6.1 |
137.6 ± 12.9 |
0.267 |
|
1 year later surgery |
133.2 ± 6.7 |
136.4 ± 11.9 |
0.257 |
|
Paavolainen Classification |
|
|
0.521 |
|
Good (130° ± 10°) |
24 |
17 |
|
|
Fair (100° - 120°) |
3 |
1 |
|
|
Poor (<100°) |
0 |
0 |
|
|
Deltoid volume ratio (%) |
91.2 ± 27.2 |
97.5 ± 18.5 |
0.003 |
ASES: American Shoulder and Elbow Surgeons
Union rate at 12 weeks after surgery was significantly (p=0.011) higher in the IMN group (87.5% [21/24]) than in the LCP group (78.5% [22/28]) (Table 2). The mean NSA in the LCP group was 135.9 ± 6.1° postoperatively and 133.2 ± 6.7° at 1-year follow-up, whereas the mean NSA in the IMN group was 133.2 ± 6.7° postoperatively and 136.4 ± 11.9° at 12-month follow-up; no statistically significant difference was detected between these groups (postoperatively, p = 0.267; 1-year follow-up, p = 0.257). The Paavolainen method revealed that 44 cases (84.6%) presented with a good mean NSA of 130° ±10°, whereas eight (15.4%) presented with a fair mean NSA of 100–120°. However, no significant difference in mean NSA was found between the two groups (p = 0.521; Table 2). The deltoid volume ratio was significantly (p=0.003) lower in the LCP group (91.2 ± 27.2) than in the IMN group (97.5 ± 18.5) (Table 2).
Nineteen patients (19/52; 36.5%) had complications, including fracture collapse (1/52, 1.9%), screw loosening (1/52, 1.9%), shoulder stiffness 1 year after surgery (11/52, 21.6%), humeral head avascular necrosis (1/52, 1.9%), and resorption or migration of the greater tuberosity (5/52; 9.6%) (Table 3). Two patients showed shoulder stiffness 1 year after the initial surgery, and a brisement procedure under general anesthesia was performed. No further complications such as fracture collapse, metal failure, screw loosening, screw penetration, infection, or peri-hardware fracture were observed (Table 3).
Table 3: Complications between the two groups
|
Variable |
Locking Plating group (n=28) |
Intramedullary Nailing group (n=24) |
|
Overall complications (n, %) |
10 (35.7 %) |
9 (37.5%) |
|
Fracture collapse (%) |
- |
1 (4.2%) |
|
Metal failure (%) |
- |
- |
|
Screw loosening (%) |
- |
1 (4.2%) |
|
Infection (%) |
- |
- |
|
Peri-hardware fracture (%) |
- |
- |
|
Stiffness at 1 year after surgery (%) |
6 (21.4%) |
5 (20.8%) |
|
Avascular necrosis with screw penetration (%) |
1 (3.6%) |
- |
|
Resorption or migration of the greater tuberosity (%) |
3 (10.7%) |
2 (8.3%) |
DISCUSSION
Consistent with our initial hypothesis, the results disclosed that there were no statistically significant differences in clinical outcomes, NSA, or complication rates between the two groups. The union rate at 12 weeks after surgery and deltoid volume ratio was higher in the IMN fixation group than in the LCP fixation group.
Numerous surgical techniques for the treatment of proximal humeral fractures have been introduced and have evolved, with osteosynthesis using a locking plate often considered the treatment of choice [14]. However, in this technique, numerous complications have been reported, and varus displacement, including screw cut-out, is the most devastating result [13]. Moreover, as the deltoid insertion may bother the distal extent of the plate of the lateral humerus, partial detachment of the deltoid is often unavoidable [14,15].
Conventionally, several studies have reported problems of antegrade nailing, which are related to the difficulty of reduction of the fracture site by indirect methods and injury to the rotator cuff [9, 10]. However, straight IMN has a satisfactory union rate with a much lower incidence of complications. Furthermore, pain and dysfunction in the rotator cuff area can be resolved with the use of straight nails [9,10]. Additionally, IMN fixation for proximal humeral fractures can avoid deltoid insertion iatrogenic injury. As few studies have reported on this topic, we suppose that this report is the first to compare deltoid atrophy between LCP and IMN fixation for proximal humeral fractures.
The surgical technique and method of locking plate fixation have gradually developed and improved biomechanical efficacy compared with other methods of fixation in osteoporotic bone [6]. However, many studies have reported post-operative stiffness caused by locking plate fixation, thus, the patients might not have gained the required sufficient interfragmentary motion to provoke callus formation during the healing process of the fracture [6]. In this study, the union rate at 12 weeks after surgery was superior in the IMN fixation group than in the LCP fixation group. We believe that the increased flexibility of the IMN facilitates secondary bone healing and improves the fracture union.
There are several limitations in this study. First, this was not a randomized retrospective study. Second, 24 patients were included in the IMN group. A small sample size often leads to a type II error, although the adequacy of the present study was proven based on the post hoc analysis results with a power of 82.3%. Third, CT is the gold standard for evaluating bone union but, in our case, simple radiography without CT evaluation was performed to define union. To increase the precision of the union analysis, cases in which the two shoulder surgeons did not agree were not defined as unions. Fourth, patients with surgical neck fractures with two-, three-, or four-part fractures were included in this study. Although differences were not detected in the ratio of the Neer classification between the two groups, it was difficult to compare surgical neck fractures with epiphyseal fractures. Finally, although previous studies have reported that osteoporosis may contribute to the outcomes of surgery, bone matrix density analysis was not performed in all patients; thus, we were not able to assess the effects of osteoporosis.
In conclusion, when performed for proximal humeral fractures, straight IMN fixation showed satisfactory clinical and radiological outcomes compared to LCP fixation. Straight IMN fixation can achieve early union and prevent deltoid atrophy related to lateral plating.
COMPLIANCE WITH ETHICAL STANDARDS
Conflict Of Interest
The authors declare that they have no conflict of interest.
Funding
There is no funding source.
Ethical Approval
This article does not contain any studies with human participants or animals performed by any of the authors.
REFERENCES
- Thanasas C, Kontakis G, Angoules A, Limb D, Giannoudis P. (2009). Treatment of proximal humerus fractures with locking plates: a systematic review. J Shoulder Elbow Surg. 18(6):837-44.
- Sproul RC, Iyengar JJ, Devcic Z, Feeley BT. (2011). A systematic review of locking plate fixation of proximal humerus fractures. Injury. 42(4):408-413.
- Badman B, Frankle M, Keating C, Henderson L, Brooks J, Mighell M. (2011). Results of proximal humeral locked plating with supplemental suture fixation of rotator cuff. J Shoulder Elbow Surg. 20(4):616-624.
- Karataglis D, Stavridis SI, Petsatodis G, Papadopoulos P, Christodoulou A. (2011). New trends in fixation of proximal humeral fractures: a review. Injury. 42(4):330-338.
- Esser RD. (1994). Open reduction and internal fixation of three- and four-part fractures of the proximal humerus. Clin Orthop Relat Res. 299:244-251.
- Seo JB, Yoo JS, Kim YJ, Kim KB. (2020). Assessment of the efficacy of the far cortical locking technique in proximal humeral fractures: a comparison with the conventional bi-cortical locking technique. BMC Musculoskelet Disord. 21(1):800.
- Gracitelli ME, Malavolta EA, Assuncao JH, Kojima KE, dos Reis PR, Silva JS, et al. (2016). Locking intramedullary nails compared with locking plates for two- and three-part proximal humeral surgical neck fractures: a randomized controlled trial. J Shoulder Elbow Surg. 25(5):695-703.
- Lopiz Y, Garcia-Coiradas J, Garcia-Fernandez C, Marco F. (2014). Proximal humerus nailing: a randomized clinical trial between curvilinear and straight nails. J Shoulder Elbow Surg. 23(3):369-376.
- Lopiz Y, Garriguez-Perez D, Martinez-Illan M, Garcia-Fernandez C, Marco F. (2022). Third-generation intramedullary nailing for displaced proximal humeral fractures in the elderly: quality of life, clinical results, and complications. Arch Orthop Trauma Surg. 142(2):227-238.
- Seo JB, Kwak KY, Yoo JS. (2020). Comparative analysis of a locking plate with an all-suture anchor versus hook plate fixation of Neer IIb distal clavicle fractures. J Orthop Surg (Hong Kong). 28(3):2309499020962260.
- Richards RR, An KN, Bigliani LU, Friedman RJ, Gartsman GM, Gristina AG, et al. (1994). A standardized method for the assessment of shoulder function. J Shoulder Elbow Surg. 3(6):347-352.
- Paavolainen P, Bjorkenheim JM, Slatis P, Paukku P. (1983). Operative treatment of severe proximal humeral fractures. Acta Orthop Scand. 54(3):374-379.
- Plath JE, Kerschbaum C, Seebauer T, Holz R, Henderson DJH, Forch S, et al. (2019). Locking nail versus locking plate for proximal humeral fracture fixation in an elderly population: a prospective randomised controlled trial. BMC Musculoskelet Disord. 20(1):20.
- Gardner MJ, Griffith MH, Lorich DG. (2005). Helical plating of the proximal humerus. Injury. 36(10):1197-1200.
- Gardner MJ, Weil Y, Barker JU, Kelly BT, Helfet DL, Lorich DG. (2007). The importance of medial support in locked plating of proximal humerus fractures. J Orthop Trauma.