Information Links
Related Conferences
Previous Issues Volume 8, Issue 2 - 2023
Sickle Cell Crisis and Emergency Department Visits: Is There a Correlation with the Weather and Seasons?
Mehvish Ahmed DO1, James Espinosa MD2,*, Syrita Farrow DO1, Alan Lucerna DO3 Victor Scali DO4
1Department of Emergency Medicine, Virtual Health System, Voorhees, NJ, USA
2Department of Emergency Medicine, Jefferson Health-New Jersey Stratford, NJ, USA
3Program Director, Emergency Medicine, Jefferson Health-New Jersey Stratford, NJ, USA
4Director of Problem-Based Learning and Faculty, Rowan University School of Medicine, Stratford, NJ, USA
*Corresponding Author: James Espinosa, MD, Department of Emergency Medicine, 18 East Laurel Road, Stratford, NJ 08084, USA; Email: [email protected]
Received Date: May 26, 2023
Publication Date: June 9, 2023
Citation: Ahmed M, Espinosa J, Farrow S, Lucerna A, Scali V. (2023). Sickle Cell Crisis and Emergency Department Visits: Is There a Correlation with the Weather and Seasons? Mathews J Emergency Med. 8(2):51.
Copyright: Ahmed M, et al. © (2023)
ABSTRACT
Background: One of the medical issues related to sickle cell disease is sickle cell pain crisis. Weather has been discussed as a trigger for sickle cell pain crisis. Aim of Study: The aim of this study was to the study relationship between sickle cell pain crisis presentations in the emergency department (ED) population of three community hospital emergency departments and local weather patterns. Materials and Methods: The study was a retrospective review of data from the ED information system, coding for the number of sickle cell pain crisis presentations per day, for selected random days. Variable studied included maximum wind speed per day, humidity (in percent), average air temperature, days with a max air temperature >80 degrees F, days with a minimum air temperature <32 degrees, maximum wind speed/humidity (calculated), rainfall, and presentations by season. Results: The relationship of rainfall to sickle cell presentations was statistically significant in the directions of significantly less sickle cell presentations on above average rainfall days. [p=0.045] The number sickle cell patient visits did not show a statistically significant relationship to the remaining variables. Conclusion: Our data support the finding of a decrease in sickle cell presentations on below average rainfall days. We did not find a relationship to high wind speed and low humidity or other variables other than rainfall. Our result may be a lag effect from days with higher rainfall. The precipitating trigger may be the days with higher rainfall with presentations after such days but not on such days. It may be that there were other precipitants and triggers that are cleared by higher rainfall, such as dust or environmental pollutants. Further study would be needed to evaluate such a hypothesis.
Keywords: Sickle Cell Pain Crisis, Sickle Cell Pain Crisis and Emergency Department, Sickle Cell Pain Crisis and Weather
INTRODUCTION
Sickle cell disease is a group of disorders that affects hemoglobin. Patients with this disorder have atypical hemoglobin molecules called hemoglobin S, which can distort red blood cells into a sickle, or crescent shape [1]. In sickle cell anemia, there is a point mutation that occurs (glutamic acid is replaced by valine at the 6th position) on the beta-globin chain of hemoglobin. This change causes an interlocking to occur between the affected beta chain and a normal chain in the deoxygenated state. This change causes an interlocking of the affected chain with adjacent hemoglobin in the deoxygenated state. This connection causes the formation of bundles of parallel rods called tactoids. These polymers grow to form a p-crystalline gel and then a crystal. This gel formation is facilitated by low pH and reduced by the presence of other hemoglobins, such as hemoglobin F. The result is a sickle-shaped cell [1]. Common signs and symptoms of sickle cell include anemia, periodic pain crises, and frequent infections. When sickling of the red blood cells occur, they can become stiff, which increases the blood’s viscosity and results in sludging of the blood leading to the inability of the sickled cells to pass freely and easily in small blood vessels. When the sickled cells cause occlusion, the results can be deprivation of oxygen rich blood to vital tissues and organs such as brain, kidneys, spleen, and lungs. Painful sickle cell crisis can occur. It may lead to various acute and chronic complications, some of which can be life threatening. Management of sickle cell disease pain crisis is a function not only of treatment with medications, but also of prevention of acute crisis through the understanding of triggers. Possible triggers for acute crisis include infection, alcohol intoxication, pregnancy, acidosis, dehydration/hypovolemia, hypoxia, folic acid deficiency, stress. Several members of our study team have noted that many sickle cell patients have expressed a belief that the weather had been a precipitating factor for their sickle cell pain crisis presentation. A review of the literature (PubMed) showed that an association of weather and sickle cell crisis has been the object of some interesting research, reflecting an international interest in the topic.
MATERIALS AND METHODS
Purpose: The purpose of this study was to determine if the number of ED visits by sickle cell patients in pain crisis has a correlation with weather variables that have been discussed in the literature. Methods: The study was a retrospective review of data from the ED information system, coding for the number of sickle cell pain crisis presentations per day, for selected random days and for sickle cell pain crisis presentations.
A full five years were studied for season vs. sickle cell pain crisis episodes. For weather parameters 72 randomly selected observational days (approximately 10% random sample) were studied from the five years. The random days selected were studied in relationship to weather data for a number of parameters, available through the National Weather Service/National Oceanic and Atmospheric Administration (NOAA) database. [http://www.weather.gov]
The following variables were studied:
- maximum wind speed per day
- humidity (in percent)
- average air temperature
- days with a max air temperature >80 degrees F
- days with a minimum air temperature <32 degrees F
- maximum wind speed/humidity (calculated)
- rainfall
Patients over the age of eighteen years of age who had a discharge diagnosis of sickle cell pain crisis or equivalent diagnosis were included. Patients less than eighteen years of age were excluded from our study.
The study was approved by the Institutional Review Board (IRB).
RESULTS
For observational days, the number of sickle cell pain crisis visits, maximum wind speed per day, humidity (in percent), average air temperature, maximum wind speed/humidity and rainfall are detailed in Table 1. The number of days with a max air temperature >80 degrees F and the number of days with a minimum air temperature <32 degrees F (from the observational day cohort) are detailed in Table 2.
The number of sickle cell presentations in below average days and above average days for the 7 variables are noted in Tables 3-4. The relationship of rainfall to sickle cell presentations was statistically significant in the directions of significantly greater sickle cell presentations on below average rainfall days. (p=0.045)
Sickle cell pain presentations by season are presented in Figure 1. A trend analysis showed the data by season to be relatively normal, with some evidence of non-normality at the tails. The trend analysis with MAPE (mean absolute percentage error), MAD (mean absolute deviation), and MSD (mean squared deviation) did not show statistical evidence of seasonality. [Figure 2].
Table 1: Number of patients with sickle cell pain crisis visits for observational days (non-air-temperature variables).
|
n=75 |
N |
Average |
StDev |
Min |
Median |
Max |
|
Number of patients with sickle cell pain visits for observational days |
75 |
0.67 |
0.66 |
0.00 |
1.00 |
2.00 |
|
Maximum wind speed per day |
75 |
13.56 |
5.60 |
2.00 |
13.00 |
35.00 |
|
Humidity (in percent) |
75 |
73.77 |
13.52 |
29.00 |
74.00 |
97.00 |
|
Average air temperature |
75 |
58.44 |
16.90 |
22.00 |
59.00 |
86.00 |
|
Maximum wind speed/humidity |
75 |
0.19 |
0.10 |
0.03 |
0.17 |
0.62 |
|
Rainfall |
75 |
0.20 |
0.49 |
0.00 |
0.00 |
3.02 |
Table 2: Air temperature related variables.
|
Days with a max air temperature >80 degrees F |
24 |
|
Days with a minimum air temperature <32 degrees F |
15 |
Table 3: Sickle cell pain crisis presentations in below average days and above average days.
|
Presentations below average days |
Presentations above average days |
||||||
|
N |
mean |
SD |
N |
mean |
SD |
P-value |
|
|
Maximum wind speed per day |
34 |
0.79 |
0.69 |
33 |
0.54 |
0.66 |
0.137 |
|
Humidity (in percent) |
35 |
0.74 |
0.66 |
40 |
0.60 |
0.67 |
0.350 |
|
Average air temperature |
35 |
0.69 |
0.63 |
40 |
0.65 |
0.70 |
0.817 |
|
Maximum wind speed/humidity |
48 |
0.70 |
0.60 |
27 |
0.60 |
0.63 |
0.460 |
|
Rainfall |
61 |
0.68 |
0.64 |
14 |
0.36 |
0.50 |
0.045 |
Table 4: Sickle cell pain crisis patient presentations in below average days and above average days, days with a max air temperature >80 degrees F.
|
Presentations days >80 F |
Presentations days <80 F |
||||||
|
N |
mean |
SD |
N |
mean |
SD |
P-value |
|
|
Days with a max air temperature >80 degrees F |
24 |
0.53 |
0.6 |
51 |
0.7 |
0.7 |
0.10 |
Table 5: Sickle cell pain crisis patient presentations in below average days and above average days, days with a minimum air temperature <32 degrees F.
|
Presentations days>32 F |
Presentations days <32 F |
||||||
|
N |
mean |
SD |
N |
mean |
SD |
P-value |
|
|
Days with a minimum air temperature <32 degrees F |
60 |
0.66 |
0.7 |
15 |
0.66 |
0.72 |
1.00 |
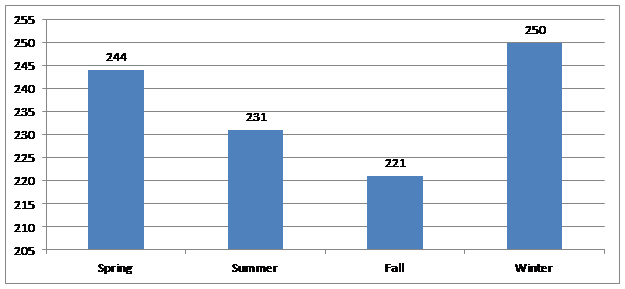
Figure 1: Total Sickle Cell Presentations by Season.
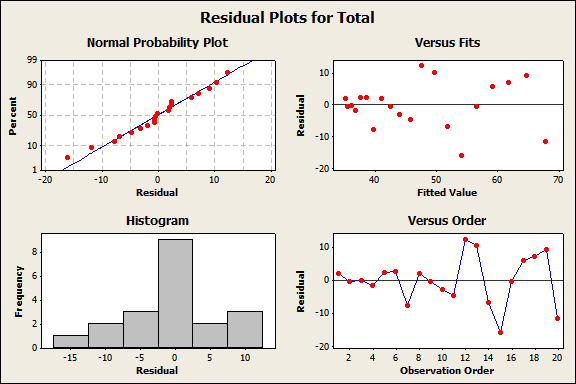
Figure 2: Residual plots, seasonality.
DISCUSSION
The relationship of rainfall to sickle cell presentations was statistically significant in the directions of significantly more sickle cell pain crisis presentations on below average rainfall days.
The number sickle cell patient visits did not show a statistically significant relationship to the remaining variables.
A trend analysis did not show statistical evidence of seasonality.
Jones, et al. noted that vaso-occlusion is a complex process, “involving red cells, white cells, platelets and vascular endothelium, with nitric oxide playing a central role. The importance of climatic factors as precipitants has been recognized for 30 years and several studies have shown an increase in painful crisis in cold and rainy seasons” [2].
A study by Slovis, et al. [3], and Smith [4] found an inconsistent relationship between weather and ED visits and hospital admissions for painful crisis. This is consistent with our findings.
We did not find a relationship to high wind speed and low humidity. “The effect of high wind speed and low humidity is likely related to skin cooling” [2].
Nolan et al found a relationship between higher wind speed and sickle cell pain crisis events. They noted that their data “lends support to physiological and clinical studies that have suggested that skin cooling is associated with sickle vaso-occlusion” [5].
Several studies have noted that there are prevention implications to understanding weather as a possible precipitant. A review of sickle cell vaso-occlusive crisis notes that cold weather may be a precipitant and advises measures to avoid extreme cold [6].
Rezar et al specifically advise against cold water swimming. The article notes that cold water immersion increases red cell viscosity [7].
It is possible that weather related variables would have had more correlation to sickle cell pain crisis episodes in the pediatric population. However, no correlation to wind speed was identified in a pediatric study by Almuqumam [8]. A correlation was seen between sickle cell pain crisis and colder weather days and higher wind speed in pediatric patients [9] and with rainfall and wind speed [10].
There has been a suggestion of a correlation of environmental pollutants and sickle cell pain crisis presentations which might explain our finding of increased presentations on lower rainfall days. The same study also showed a 12 to 15 hour lag effect in change in weather conditions on presentations [11]. Our study did not look at lag effects. It is possible that the finding that the more dry than average effect seen was a lag effect from previous rainfall.
It is also possible that various studies have come to different conclusions concerning that effect of weather on sickle cell pain crisis presentations based on local climate conditions [12].
CONCLUSIONS
The relationship of rainfall to sickle cell presentations was statistically significant in the directions of significantly more sickle cell presentations on below average rainfall days. [p=0.045]
The number sickle cell patient visits did not show a statistically significant relationship to the remaining variables.
It is possible that our result was a lag effect from days with higher rainfall. It may be that there were other precipitants and triggers that are cleared by higher rainfall, such as dust or environmental pollutants. Further study would be needed to evaluate such a hypothesis.
A trend analysis did not show statistical evidence of seasonality. Winter and spring are the seasons with the greatest number of presentations. The difference was not statistically significant.
REFERENCES
- Janz TG. (2010). Rosen's Emergency Medicine Concepts and Clinical Practice 7th edition. Emerg Med. 119: 1568-1571.
-
Jones S, Duncan ER, Thomas N, Walters J, Dick MC, Height SE, et al. (2005). Windy weather and low humidity are associated with an increased number of hospital admissions for acute pain and sickle cell disease in an urban environment with a maritime temperate climate. Br J Haematol. 131(4):530-533.
- Slovis CM, Talley JD, Pitts RB. (1986). Non relationship of climatologic factors and painful sickle cell anemia crisis. Chronic Dis. 39(2):121-126.
- Smith WR1, Coyne P, Smith VS, Mercier B. (2003). Temperature changes, temperature extremes, and their relationship to emergency department visits and hospitalizations for sickle cell crisis. Pain Manag Nurs. 4(3):106-111.
- Nolan VG1, Zhang Y, Lash T, Sebastiani P, Steinberg MH. (2008). Association between wind speed and the occurrence of sickle cell acute painful episodes: results of a case-crossover study. Br J Haematol. 143(3):433-438.
- Yale SH, Nagib N, Guthrie T. (2000). Approach to the vaso-occlusive crisis in adults with sickle cell disease. Am Fam Physician. 61(5):1349-1356, 1363-1364.
- Resar LM1, Oski FA. (1991). Cold water exposure and vaso-occlusive crises in sickle cell anemia. J Pediatr. 118(3):407-409.
- Almuqamam M, Ahuja K, Wassef I, Kilaikode S, Sedrak A. (2021). Effect of Weather on Frequency of Vaso-Occlusive Crisis in Children With Sickle Cell Disease. Cureus. 13(8):e17254.
- Rogovik AL, Persaud J, Friedman JN, Kirby MA, Goldman RD. (2011). Pediatric vasoocclusive crisis and weather conditions. J Emerg Med. 41(5):559-565.
- Piel FB, Tewari S, Brousse V, Analitis A, Font A, Menzel S, et al. (2017). Associations between environmental factors and hospital admissions for sickle cell disease. Haematologica. 102(4):666-675.
- Mekontso Dessap A, Contou D, Dandine-Roulland C, Hemery F, Habibi A, Charles-Nelson A, et al. (2014). Environmental influences on daily emergency admissions in sickle-cell disease patients. Medicine (Baltimore). 93(29):e280.
- Davis RE, Markle ES, Windoloski S, Houck ME, Enfield KB, Kang H, et al. (2020). A comparison of the effect of weather and climate on emergency department visitation in Roanoke and Charlottesville, Virginia. Environ Res. 191:110065.