Previous Issues Volume 1, Issue 1 - 2018
Rib Forked of Lushka
Oscar Alonso Plaza*1,2,3
1National Institute of Legal Medicine and Forensic Sciences, Cali-Colombia.
2Faculty of Health Sciences, Pontificia Universidad Javeriana, Cali-Colombia
3Faculty of Medicine, Santiago of Cali, University, Cali-Colombia.
Corresponding Author: Oscar Alonso Plaza, National Institute of Legal Medicine and Forensic Sciences, Cali-Colombia, E-Mail: [email protected]
Received Date: 13 Mar 2018 Accepted Date: 29 Mar 2018 Published Date: 03 Apr 2018
Copyright © 2018 Plaza OA
Citation: Plaza OA. (2018). Rib Forked of Lushka. Mathews J Foren. 1(1): 002.
ABSTRACT
The anatomical variations of the costal arches are rare and may vary from its usual presentation as are the cervical ribs, to the more unusual such as lumbar ribs, bifurcated, synostosis, presenting these variations frequently in the seventh cervical and first chest. The bifurcated variant of a costal arch at its distal end near the junction of the sternum was described by Lushka in 1860, clinical presentation is asymptomatic and diagnosis is eminently radiological, when the bifurcated rib is associated with two pathologies such as Tumor Queratoquistico Odontogenic jaw and the Gorlin-Goltz syndrome.
KEYWORDS
Rib Forked; Traumatic Injury; Abuse; Surgical Approaches.
INTRODUCTION
Knowledge of the anatomy of the rib cage is crucial for understanding respiratory physiology and for the surgical approach of cervical, thoracic and abdominal pathologies since the presence of anatomical variants of course can modify the treatments and / or procedures established. The bifurcated rib is an anatomical variant of the costal grid associated with alterations of the muscles of the thoracic wall and of the intercostal vessels and nerves. Its presentation may be associated with respiratory difficulties and neurological disorders by modifying the kinematics of respiration by the tension changes that it produces on the thorax muscles when generating compensatory changes due to the asymmetry of the thorax. Generally in these cases the intercostal nerve is divided into two at its distal end. Its presentation is approximately 1.2% of human beings, it is usually unilateral and according to the reviewed literature the anatomical variants of the ribs occur in women and in the right side of the thorax [1]. The bifurcated or Lushka rib has been associated with an aggressive pathology such as the odontogenic keratocystic tumor of the jaw which, when presented with "nevoid basal cell carcinoma", is known as Gorlin-Goltz syndrome [2].
MATERIAL AND METHODS
Two cases of bifurcated ribs are presented as incidental findings in the necropsy process, made in National Institute of Legal Medicine and Forensic Sciences, Cali-Colombia, in one case it is found as an isolated anatomical variant (Figure 1) and the other case is associated with nevical lesions in the face and left inguinal region, facial asymmetry, large ears and poorly molded, which are the most characteristic anomalies of Gorlin-Goltz syndrome. In the first case, a bifurcation of the third right costal arch can be seen at its proximal end and close to the insertion in the sternal bone. The dissection reveals the excision of the intercostal nerve, without alterations in the vasculature. It is noted that the intercostal muscles of the second space are small and the intercostal muscles corresponding to the space immediately below are greater in their length so they will cause asymmetry in the chest wall modifying the kinematics of breathing. In the second case (Figure 2), the bifurcation of the third costal arch can be seen almost from the left costal angle without major alterations in the muscles of the pore intercostal spaces with excision of the intercostal nerve, so it is inferred that there are no major alterations in the kinematics of respiration, but when reviewing the morphometry of the deceased, other anomalies were seen on the face (asymmetry), ears (large and poorly molded), thorax (asymmetric) and nevus lesions on the face and in the left inguinal region, all of which present a good descriptive reference like the one presented in the Gorlin-Goltz syndrome [2]. The first documented description of the bifurcation of a rib was made by Lushka in 1860 [4] and in his honor this eponym was coined.

Figure 1:*Rib forked.
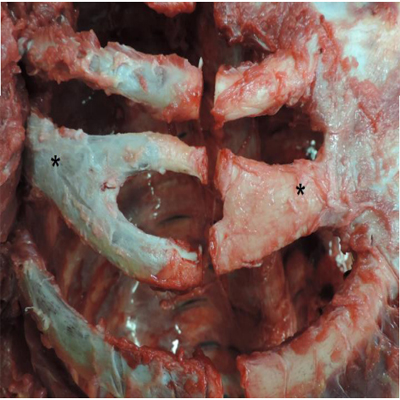
Figure 2:*Rib forked.
RESULTS
The anatomical variations of the costal arches and the intercostal neurovascular bundle are related to the processes inherent to their development. The skeleton originates from the lateral paraxial mesoderm, and neural crest. The paraxial mesoderm forms somites and somitomes. Somites differ in sclerotomes and dermomyotomes; at the end of the fourth week the sclerotome forms the mesenchyme or connective tissue. The ribs are derived from the paraxial sclerotome and are formed from the costal processes (costal processes) of the thoracic vertebrae and are cartilaginous during the embryonic period. The ribs ossify in the fetal period. The normal pattern is that there are seven pairs of true ribs attached to the sternum by its own cartilage (1-7), three joined to the sternum through the cartilage of the other rib (false 8-10) and two floating (11-12) that are not attached to the sternum. During the development process some disorganization may occur and the bifurcation may occur as a consequence of it. In the cases described, cannot speak of congenital deformities since a diagnosis cannot be made because, globally and unambiguously, we cannot speak of a single etiology for these cases. Similarly, a syndrome cannot be determined either because there is no transcendental information (prognosis, risk of recurrence, possibility of prenatal detection, etc.). The usefulness of the presentation of these cases is also focused on the medical-legal field because the anatomical variants can simulate a traumatic injury, since when a radiological examination is performed they can be used for misinterpretations as evidence of abuse [3]. In surgical approaches due to the size of the bifurcation of the costal arch, the thorax may be shortened on one side than on the other due to asymmetry, so this difference may modify the surgical field.
CONCLUSIONS
The bifurcated rib is a rare congenital malformation of the chest wall caused by a disorganization of the embryological process. Although isolated does not cause significant morbidity, its presence may be associated with other congenital abnormalities or aggressive pathologies. A radiological misinterpretation can simulate a costal fracture in cases where abuse is suspected. The sequelae of this isolated malformation can be interpreted from the respiratory point of view since the restriction of the movements of the rib cage can lead to a decrease in the intrathoracic pressure decreasing the venous return to the heart. The other sequelae is usually associated with the surgical approach of renal pathologies through a subcostal incision by altering the anatomy of the surgical field.
REFERENCES
- (2013). Scientific Working Group for Forensic Anthropology (SWGANTH) Age Estimation Issue.
- McKinley, Michael, O'Loughlin and Valerie Dean. (2008). La anatomia humana (2ª ed.). McGraw-Hill. pag. 214. ISBN 978-0-07-128320-5
- Salvador Joaquin and CarreraJose M. (1995). Sindromes Congenitos Malformativos. Masson, SA. 138.
- Pasquale-Styles MA, Crowde CM, Fridie J and Milla SS, (2014). Bilateral First Rib Anomalous Articulations with Pseudarthroses Mimicking Healing Fractures in an Infant with Abusive Head Injury. J Forensic Sci, 59(6): 1668-1671.
- Luschka H. (18 60) Die anomalen Articulationen des ersten Rippenpaares. Wiener Akad. Sitzungsberichte. Math.-Natur. KI. 39:413-430.
- Bergman RA, Afifi AK and Miyauchi R, (2015). Ilustrated Encyclopedia of Human Anatomic Variation.