Information Links
Related Conferences
Previous Issues Volume 4, Issue 1 - 2023
Prospective General Inhalation Anesthesia for Pediatric Patients Undergoing Radiotherapy. Pilot Project with 25 Children without Venous Access
Luiz Eduardo Imbelloni1,*, Débora Baroni2, Patrícia L Procópio Lara3, Sylvio Valença de Lemos Neto4, Ana Cristina Pinho5, Anna Lúcia Calaça Rivoli6, Geraldo Borges de Morais Filho7
1Senior Researcher of Nacional Cancer Institute (INCA), Rio de Janeiro, RJ, Brazil
2Resident of the 3rd year of Anesthesiology at INCA, Rio de Janeiro, RJ, Brazil
3Anesthesiologist at the National Cancer Institute (INCA), Rio de Janeiro, RJ, Brazil
4Anesthesiologist at the National Cancer Institute (INCA), Responsible for the CET-SBA of the National Cancer Institute, Rio de Janeiro, RJ, Brazil
5Anesthesiologist at the National Cancer Institute (INCA), Co-Responsible for the CET-SBA of the National Cancer Institute, Rio de Janeiro, RJ, Brazil
6Anesthesiologist at the National Cancer Institute (INCA), Responsible Coreme Residence INCA
7Master in Labour Economics, UFPB, João Pessoa-PB, Brazil & Statistician of the Complexo Hospitalar Mangabeira, João Pessoa-PB, Brazil
*Corresponding author: Luiz Eduardo Imbelloni, MD, PhD, Senior Researcher of Nacional Cancer Institute (INCA), Av. Epitácio Pessoa, 2356/203-Lagoa, 22411-072-Rio de Janeiro, RJ, Brazil, Tel: + 55.11.99429-3637, ORCID ID: 0000-0003-3808-5858; Emails: [email protected]; [email protected].
Received Date: March 17, 2023
Published Date: March 28, 2023
Citation: Imbelloni LE, et al. (2023). Prospective General Inhalation Anesthesia for Pediatric Patients Undergoing Radiotherapy. Pilot Project with 25 Children without Venous Access. Mathews J Anesth. 4(1):11.
Copyrights: Imbelloni LE, et al. © (2023).
ABSTRACT
Background: Radiation therapy is a cornerstone in the treatment of cancer in children. Although painless, there is a requirement for the child to lie still by themselves in the radiation treatment room. Most RT services use intravenous sedation or anesthesia. The aim of the study was to describe the technique of inhalational anesthesia with sevoflurane without venoclysis for general anesthesia during RT from January to December 2022, as a pilot project in 25 children. Methods: It is an observational, descriptive, and prospective study of a series of cases. Pediatric patients aged 2 to 13 years diagnosed with cancer, underwent RT under sevoflurane anesthesia without venous access. RT is performed five days a week, with only Tuesdays selected, with the same anesthesiologist and anesthesia resident. patients were monitored with a cardioscope, pulse oximetry, capnography, and gas analyzer. During the procedure, the following were evaluated: the expired fraction of sevoflurane and the corresponding Minimum Alveolar Concentration (MAC) for induction and maintenance, anesthesia and awakening time, place and time of irradiation, and immediate and late adverse effects (after awakening until discharge hospital). Finally, the time of hospital discharge and complications were evaluated after completion. Results: A total of 25 patients diagnosed with cancer and receiving radiotherapy were studied. No difference was observed between genders, with 96% of children between 2 and 8 years old, and 60% being 4 and 5-year-old children. Sevoflurane was administered to 100.0% of patients in all treatment sessions. Mean anesthesia time was 22.96 minutes, mean irradiation time was 10.84 minutes, and mean awakening time was 6.12 minutes. Side effects were more frequent when they reached values greater than or equal to 1.5 MAC. Conclusions: In pediatric patients diagnosed with cancer, the use of sedation and anesthesia during radiotherapy treatment was required mainly in young children. Sevoflurane as monotherapy without venous access turned out to have no severe complications, however, sevoflurane MAC increases above 1.5 were associated with the onset of complications. The awakening was quick (6 minutes) as well as the discharge for residence (19 minutes).
Keywords: Radiotherapy, Pediatric, Oncology treatment, Sevoflurane, Inhalation Anesthesia.
KEY POINTS
What is already known?
- Radiotherapy (RT) is a fundamental part of cancer treatment in pediatric patients.
- Sedation and/or general anesthesia are commonly utilized to facilitate radiotherapy treatment in children.
- All intravenous drugs such as midazolam, propofol, ketamine, and dexmedetomidine were indicated for sedation anesthesia for the RT procedure.
- Propofol has become the drug of choice at various institutions.
- Few studies with inhaled agents have been published.
- Sevoflurane is an ether inhalation general anesthetic agent.
What this article adds.
- Prospective study with only one inhalational agent without venoclysis, and without tracheal intubation.
- Sevoflurane proved to be a fast-acting agent with smooth induction and awakening in around 6 minutes.
- There were few side effects during the procedure.
- None of the children had complications in the PACU or at the residence.
- With this technique, there is no need to perform venipuncture in children.
- Hospital discharge occurred around 19 minutes after RT.
INTRODUCTION
The number of new cases of childhood cancer is expected in Brazil, for each year of the triennium 2020-2022, there will be 4,310 new cases in males and 4,150 for women [1]. These values correspond to an estimated risk of 137.87 new cases per million for males and 139.04 per million for females [1]. The predominant types of cancer in the age group 0-19 years published by the American Cancer Society in 2019 are leukemia (28%), central nervous system (26%), and lymphomas (8%) [2].
Unlike adult cancer, childhood cancer is predominantly of embryonic nature and usually affects blood system cells and tissues of support. The most common childhood cancers include leukemia, brain and CNS tumors, and lymphomas, with neuroblastomas, Wilms tumors, and sarcomas being less common [3].
Radiotherapy (RT) is a fundamental part of cancer treatment in pediatric patients. Radiation therapy is used to target tumors in specific locations. Depending on the clinical context of disease in each patient, treatment paradigms can vary markedly from single-modality therapy to combinations of surgery, systemic therapy, targeted agents, and/or RT [4]. The use of RT has historically been one of the great successes in the treatment of pediatric cancers [5]. Today, around 80% of children and adolescents affected by the disease can be cured if diagnosed early and treated in specialized centers [1].
RT can be delivered in two ways, externally and internally. The majority of pediatric cancers are treated with external radiation. For the topography precision that these techniques require maintaining the same position and immobility during procedures is imperative [6]. Sedation and/or general anesthesia are commonly utilized to facilitate RT treatment in children. Performing safe and effective anesthesia for pediatric cancer patients undergoing RT presents several challenges Precise positioning and immobilization of the patient during treatment is essential to ensure that high-energy radiation can be delivered to the tumor, whilst minimizing exposure to healthy surrounding tissues [7]. Treatment with RT is usually short-lived, but they must remain immobile and often lie down [7]. In addition, childhood must be continuously monitored by the cardiovascular and respiratory systems, through remote control [7].
Our primary objectives in the present study were to determine the technique of inhalational anesthesia with sevoflurane and without venous access and the incidence of anesthesia-related complications in children aged 2 to 13 years undergoing RT at the National Cancer Institute (INCA). As secondary objectives we also checked the pharmacologic regimens, monitoring techniques, need for venous access or the use of access previously present, preoperative fasting time, duration of the procedure, and release time for residency.
METHODS
This is a descriptive, observational, and prospective study during the period of January 2022 to December 2022. This study was registered in Plataforma Brasil (CAAE: 91507318.1.0000.5274) and was approved by the Ethics Committee Scientist in Instituto Nacional de Câncer (INCA) with number 2.762.022. The informed consent form was signed by one of the children's parents. The data were obtained from the clinical records of each patient and were integrated into the electronic sheet, to later carry out the processing of the information and descriptive statistical analysis of the study variable.
Inclusion criteria were pediatric population aged 2 to 13 years of age undergoing general inhalation anesthesia without venous access undergoing RT, with confirmed oncological diagnosis and regardless of histological type or staging. Patients older than 13 years, who refused a legal guardian, used intravenous anesthesia, and had simulation sessions were excluded from the study.
All RTs were performed with the TrilogyTM device. The TrilogyTM lineae accelerator from Varian Medical Systems was used to perform the radiotherapy, which presents the techniques of 3D-CRT (conformational radiotherapy), IMRT (intensity-modulated beam radiotherapy), and IGRT (image-guided radiotherapy). Pre-molded thermoplastic masks were used in simulation sessions to ensure complete immobilization during radiotherapy in patients with central nervous system, neuraxial, and head and neck tumors.
Each day a different anesthesiologist is always accompanied by an anesthesiology resident. Due to the different conducts, a day was selected for the implementation of the inhalation anesthesia protocol with sevoflurane without venipuncture, with the same anesthesiologist, and accompanied by the same resident.
Patients were monitored with a cardioscope, non-invasive blood pressure, pulse oximetry, capnography, and gas analyzer to perform the procedures. The anesthetic technique performed was general inhalation anesthesia with sevoflurane and 100% oxygen (4 l/min) flow under a face mask (without tracheal intubation) in a semi-closed pediatric circuit, valved, with a CO2 absorber and bacterial filter or Baraka circuit (Mapleson A). The anesthesia device used in this research with children was the Carestation 620 (GE Healthcare) suitable for smaller spaces such as RT. This device (Carestation 620) allows the evaluation of MAC, capnometry, capnography, analysis of gases used, inspired and expired fractions. Its eco-flow software visually represents oxygen flow and anesthetic agent usage. Peripheral venous accesses were not punctured during the sessions and venous accesses previously punctured in other sectors were not used.
We collected demographic data, including age, weight, height, sex, ASA physical status, oncology diagnosis, and local RT procedure. The information collected from the anesthesia record included anesthesia duration (interval between first administration of drugs and completion of RT procedure), anesthetic drugs used (selection of drugs, use of adjuvant drugs, total dose), patient position, fasting time, number of RT sessions, need for venous access, irradiation time, tumor site, awakening and length of stay in the post-anesthetic care unit (PACU).
During the procedure, the following were evaluated: the expired fraction of sevoflurane and the corresponding Minimum Alveolar Concentration (MAC) for induction and maintenance, anesthesia and awakening time, place and time of irradiation, and immediate and late adverse effects (after awakening until discharge hospital). Finally, the time of hospital discharge and complications were evaluated after completion. After completing the procedure, the children were awakened and referred to the PACU, and the time for discharge to residency was recorded.
The anesthesia-related complications were: oxygen desaturation (saturation <90%), apnea (absence of respiratory effort for >15 s), airway obstruction (required interventions), and minor airway complications. Hemodynamic complications were defined as any recorded variations in heart rate.
Statistical analysis
For the analysis of continuous variables, we used the Wilcoxon-Mann-Whitney test. The Wilcoxon-Mann-Whitney test is used to compare two groups to verify whether they belong to the same population. It is used when the samples are independent. For the analysis of qualitative variables, we used the Chi-Square test. The Chi-Square independence test is used to find out if there is an association between the row variable and the column variable in a contingency table constructed from sample data. We used the significance level of 5%.
RESULTS
A total of 693 RTs were performed between January 2022 and December 2022 with the TrilogyTM device. Of this total, 154 RT in children were performed on Tuesday and 539 RT on other days. 129 RT were excluded and 25 children submitted to RT under inhalation anesthesia with sevoflurane without venipuncture were analyzed as a pilot project, according to the flow diagram consort (Figure 1). Five children previously had venous access, and it served as a control for side effects and whether they would need to use it.
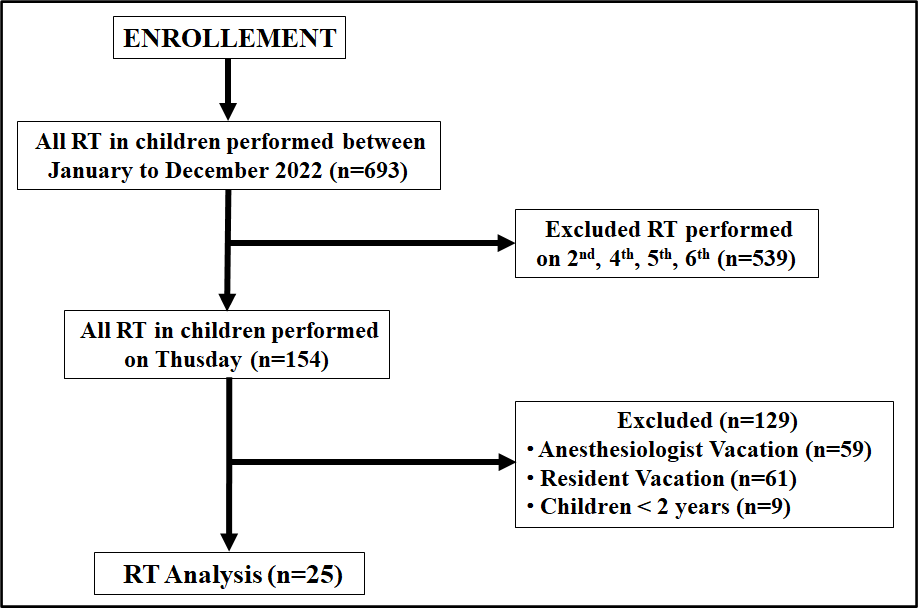
Figure 1. Consort flow diagram.
Demographic data for the 25 children are in Table 1, Figure 2. All children were considered Physical Status ASA II. Twenty-four (96%) of the 25 children were between 2 and 8 years old. Sixteen (60%) were 4 and 5-year-old children. Regarding the oncological diagnosis, the following tumors were found: rhabdomyosarcoma with a total of 6 patients, Wilms' tumor with of 4 patients, medulloblastoma with of 4 patients, glioma with of 4 patients, sialoblastoma with of 3 patients, brain stem tumor with of 3 patients, and cerebral tumor not determined with 1 patient. In this way, several sites were irradiated according to the type and location of the tumors. The skull and neuroaxis were irradiated in 12 children, followed by the face in 8 children, the thorax in 2 children, and the flank, pelvis, and lower limb in 3 children.
Table 1. Patients’ characteristics regarding age, weight, height, and sex (Mean±SD).
|
VARIABLE |
CHILDREN |
|
Number |
25 |
|
Age (years) (Minimum-Maximum) |
4.80±2.14 (2 – 13) |
|
Weight (kg) (Minimum-Maximum) |
20.93±8.14 (12 – 47) |
|
Height (cm) (Minimum-Maximum) |
111.20±15.40 (90 – 151) |
|
Gender: F / M |
12 / 13 |
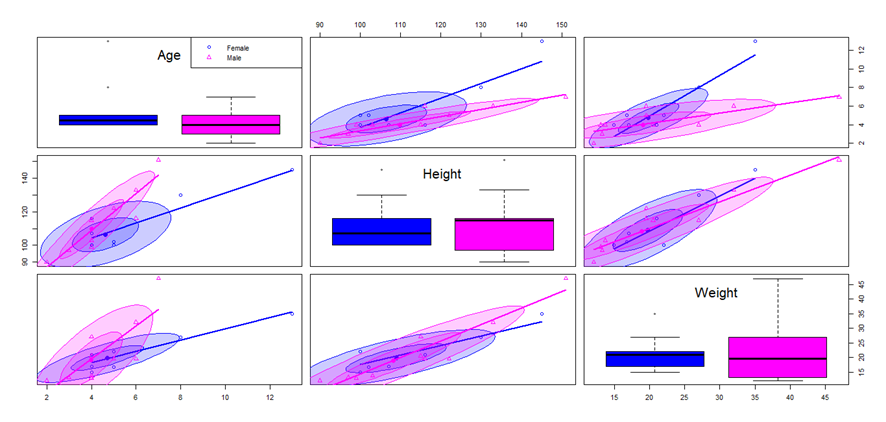
Figure 2. Anthropometric data.
With regard to medications in use, 16 children were not using any medication, 7 patients were using dexamethasone to control cerebral edema caused by the tumor, 3 children were associated with omeprazole, 1 child was using risperidone to treat autistic spectrum and 1 child was using morphine for pain control.
All children were anesthetized for RT on an outpatient basis, having arrived at the hospital on the morning of the procedure. Thus, the fasting time of the children was 10.12±1.61 hours, ranging from 8 to 14 hours. During anesthesia, venous accesses were not punctured, but 5 patients already had a previous implantable venous catheter, which was not used during the RT session.
All children were monitored with a cardioscope, pulse oximetry, and capnograph, but non-invasive blood pressure was never used. The pediatric semi-closed circuit with CO2 absorber and bacterial filter was the most used in 18 children, the Baraka circuit (Mapleson A) in 6 children, and in 1 child the semi-closed adult system was used. For anesthetic induction, sevoflurane was used with an average MAC value of 1.5±0.3 (ranging from 09 to 2.5) and an average value for anesthetic maintenance was 0.8±0.2 (ranging from 0.5 to 1.3) (Table 2).
Table 2. Comparing immediate adverse effects (n=10) with the absence of adverse effects (n=15) and possible correlations.
|
VARIABLES |
NOT=15 |
YES=10 |
P-VALUE |
|
Age (years) |
5.40±2.55 |
3.90±0.73 |
0.04435* |
|
Weight (kg) |
22.32±9.49 |
18.86±5.36 |
0.5969* |
|
Height (cm) |
115.86±17.78 |
104.20±7.05 |
0.05444* |
|
Gender: F / M |
7 / 8 |
5 / 5 |
1.0000** |
|
Fasting Time (h) |
10.26±1.83 |
9.90±1.28 |
0.8198* |
|
MAC Sevoflurane Induction |
1.47±0.39 |
1.75±0.31 |
0.07727* |
|
MAC Sevoflurane Maintenance |
0.83±0.19 |
0.89±0.24 |
0.8218* |
|
Anesthesia Time (min) |
23.60±7.59 |
22.0±5.77 |
0.5771* |
|
Irradiation Time (min) |
12.06±6.05 |
9.0±2.78 |
0.2423* |
|
Wake-up Time (min) |
6.06±2.46 |
6.20±2.89 |
0.9777* |
|
Hospital Discharge (min) |
20.20±6.67 |
17.30±6.56 |
0.3152* |
Mean anesthesia time was 22.96±6.84 minutes (ranging from 12 to 38 minutes), mean irradiation time was 10.84±5.16 minutes (ranging from 4 to 26 minutes), and mean awakening time was 6.12±2.58 minutes ( ranging from 2 to 11 minutes). All children were discharged from the hospital in 10 to 35 minutes, with an average of 19.04±6.65 minutes (Table 2).
Ten children had side effects during and upon awakening, and 15 children had no immediate adverse effects. Agitation was observed at the end of the procedure in 5 children, bradycardia in 4 children during the anesthetic with no hemodynamic instability, and 1 child had laryngospasm that was easily recovered with positive pressure ventilation.
Inferential statistical analysis showed that the only study variable that showed a significant difference in the increased risk of immediate adverse effects was the expired fraction of sevoflurane and the corresponding MAC used in anesthetic induction (Table 2). Furthermore, these effects were more frequent when they reached values greater than or equal to 1.5 MAC.
None of the children had complications in the PACU or at the residence, by follow-up via telephone. None of the children in this study with inhalational anesthesia with sevoflurane without venipuncture required orotracheal intubation or hospitalization after RT.
DISCUSSION
Radiotherapy is of fundamental importance for the treatment of pediatric cancer, and the vast majority of children who will undergo RT will require sedation or anesthesia. The first objective of this study showed that inhalational anesthesia with sevoflurane without venoclysis was perfectly feasible and safe, with a low incidence of side effects in outpatients with hospital discharge in an average of around 20 minutes. There was no significant difference between the incidence of men and women, and 96% of children were younger than 8 years.
Ideal anesthetic agents for use in RT should show a rapid onset of action, with sedation, hypnosis, and amnesia, have a short duration of effect, show a safety profile with repeated administration together with a low risk of tachyphylaxis, minimal adverse effects, and good relationship cost-effectiveness. In this way, it facilitates painless administration of anesthetic, to achieve immobilization and with it maintain in a single position to the patient, as well as ensuring a patent airway in a variety of positions according to each case, all this with the purpose that this intervention entails a minimum interference with daily activity [7].
Sevoflurane is an ether inhalation general anesthetic agent with a lower solubility in blood than isoflurane or halothane but not desflurane and fulfills all the requirements of an ideal anesthetic for inhalation use in children. The low solubility and the absence of pungency facilitate rapid mask induction; the low blood solubility also expedites wash-out and therefore recovery from anesthesia. Sevoflurane allowed a smooth and rapid induction with an average of 1.5 MAC, maintenance with 0.8 MAC, an average wake-up time of 6.12 minutes, and hospital discharge with an average of 19.04 minutes, without complications. Other services prefer the use of propofol in 100% of children, but venipuncture is necessary [7,8]. The rate of anesthesia-related complications was low (1.3%) in a study with propofol has become the drug of choice at your institution [7].
At the INCA, with the advent of sevoflurane, the use of inhalational anesthesia without venoclysis has been used for years, but no study has been carried out on this technique. The objective of this study was to demonstrate, in a pilot study with 25 children, the possibility of performing RT without the use of venous access, which was obtained in all children, with a low incidence of complications, and became the technique of choice in our institution. This pilot study confirmed what was done for a long time without the aim of a scientific study, showing that the technique is safe, feasible, easily performed, non-invasive, and low-cost (mono drug).
An estimated 11,060 new cancer cases will be diagnosed among children ages 0 to 14 years in the US in 2019 [2]. The number of new cases of childhood cancer estimated for Brazil, for each year of the triennium 2023 to 2025, is 7,930 cases, which corresponds to an estimated risk of 134.81 per million children and adolescents [9]. It is estimated that approximately 430,000 new cases of cancer occur among children and adolescents (from 0 to 19 years old). The main types of cancer that occur in children are leukemias, CNS tumors, and lymphomas. The embryonic tumors (neuroblastoma, renal tumors, and retinoblastoma) mostly affect children, while in adolescents aged 15 to 19 years, tumors are more frequent epithelial cells, such as thyroid and carcinomas, and melanomas [9]. Treatment for childhood cancer is based mainly on the type and stage (extent) of cancer. The main types of treatment used for childhood cancer are surgery, radiation therapy, and chemotherapy. Radiation exposure to the brain can predispose one to hearing loss, impaired neurocognition, and neuroendocrine dysfunction, among other functional deficits [10]. It was not the object of this study to evaluate the complications of RT.
In a recent review, almost all intravenous drugs such as midazolam, propofol, ketamine, and dexmedetomidine were indicated for sedation-anesthesia for the radiation therapy procedure [11]. In this review, the technique used in this study, sevoflurane without performing venipuncture, essential for intravenous anesthesia, was not suggested. This technique in this pilot study with 25 children proved to be safe and easy to perform. The pediatric semi-closed circuit with CO2 absorber and bacterial filter was the most used in 18 children, the Baraka circuit (Mapleson A) in 6 children, and only one child was 13 years old when she was anesthetized with an adult circuit. The majority of children who require anesthetic intervention can tolerate the daily therapeutic regimen with only monitored anesthesia care [12]. In the review article, the intravenous route is the preferred method of administering medication to these patients [12].
A total of 9,328 were administered to 340 children retrospective reviews of anesthetic records for patients treated with proton therapy, all patients received TIVA with spontaneous ventilation and oxygen delivery by face mask or nasal cannula. None required daily endotracheal intubation. Two episodes of bradycardia and one episode each of; seizure, laryngospasm, and bronchospasm were identified for a cumulative incidence of 0.05% [13]. In this study, sevoflurane monotherapy without venous access, and oxygen through a mask or nasal cannula, presented a low incidence of easily corrected complications, being a new option for RT, and no need for tracheal intubation. Sevoflurane has negligible airway irritant effects, which facilitates a smooth induction in pediatric patients, and makes sevoflurane especially amenable to rapid induction of anesthesia and rapid awakening.
Administration of sevoflurane in doses ranging from 0.4 to 1.2 MAC is associated with a stable [14]. In this study with sevoflurane monotherapy showed an increased risk of immediate adverse effects, with the expired fraction of sevoflurane and the corresponding MAC used in anesthetic induction. These effects were more frequent when they reached values greater than or equal to 1.5 MAC.
In this study, the average pre-procedure fasting time was high in relation to the current recommendations of 6 hours for solid foods and 1 hour for clear liquids, according to a consensus published in Pediatrics [15]. In this context, prolonged fasting time may increase the risk of dehydration, arterial hypotension, bradycardia and cause discomfort to the patient. This fact may explain the bradycardia without hemodynamic instability in the four patients in the study since they had fasted for more than 8 hours. Despite this, this study did not present statistical significance in the inferential analysis of the data, when relating fasting time with the risk of adverse effects during anesthesia.
CONCLUSION
Radiation therapy has proved to be an important armamentarium for cancer management in children. The procedure also requires a motionless child to deliver the radiation at the intended site and thus avoid unnecessary radiation exposure. The delivery of safe and effective anesthesia for pediatric oncology patients undergoing RT presents several challenges. Providing anesthesia for children undergoing radiation treatment is both challenging and rewarding. The vast majority of cited and researched articles prefer to use intravenous anesthesia with different types of drugs. Sevoflurane as monotherapy without venous access turned out to be a safe technique, easy to perform with no severe complications, with rapid awakening and hospital discharge and is the preferred method of choice in these children in our institution.
FINANCIAL SUPPORT
None.
CONFLICT OF INTEREST
None.
CONTRIBUTION
No.
IRB
No.
DISCLOSURES
Name: Luiz Eduardo Imbelloni, MD, PhD.
Contribution: This author helped with study conception and design, this author helped perform background research, statistical analysis, generation of tables and figures, analysis and interpretation of data, selected all the references used for the preparation of the study, wrote the entire manuscript, and gave final approval of the manuscript.
Name: Débora Baroni, MD.
Contribution: Anesthesiologist resident scheduled to perform RT under inhalational anesthesia, and monitor the children's evolution. Revised the manuscript critically for intellectual content, and gave final approval of the manuscript.
Name: Patrícia L. Procópio Lara, MD.
Contribution: Anesthesiologist resident scheduled to perform RT under inhalational anesthesia, and monitor the children's evolution. Revised the manuscript critically for intellectual content, and gave final approval of the manuscript.
Name: Sylvio Valença de Lemos Neto
Contribution: This author helped with study conception and design, and gave final approval of the manuscript.
Name: Ana Cristina Pinho
Contribution: This author helped with study conception and design, and gave final approval of the manuscript.
Name: Anna Lúcia Calaça Rivoli
Contribution: This author helped with study conception and design, and gave final approval of the manuscript.
Name: Geraldo Borges de Morais Filho, MSc.
Contribution: This author performed statistical analysis, generation of figures, analysis, and interpretation of data, revised the manuscript critically for intellectual content, and gave final approval of the manuscript.
This manuscript was handled by: Luiz Eduardo Imbelloni, MD, Ph.D.
REFERENCES
- Schilithz AOC, Lima FCS, Oliveira JFP, Santos MO, Rebelo MS. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2020: incidência de câncer no Brasil/Instituto Nacional de Câncer José Alencar Gomes da Silva.–Rio de Janeiro: INCA, 2019. ISBN 978-85-7318-388-7.
- American Cancer Society. Cancer Facts & Figures 2019. Atlanta: American Cancer Society; 2019. Global Headquarters: American Cancer Society Inc. 250 Williams Street, NW, Atlanta.
- Ries L, Melbert D, Krapcho M, et al. (2012). SEER Cancer Statistics Review, 1975–2004. Bethesda, MD: National Cancer Institute.
- DeNunzio NJ, Yock TI. (2020). Review modern radiotherapy for pediatric brain tumors. Cancers. 12(6):1533. DOI: 10.3390/cancers12061533.
- O’Leary M, Krailo M, Anderson JR, Reaman GH. (2008). Progress in childhood cancer: 50 years of research collaboration, a report from the Children's Oncology Group. Semin Oncol. 35(5):484-493.
- McFadyen JG, Pelly N, Orr RJ. (2011). Sedation and anesthesia for the pediatric patient undergoing radiation therapy. Curr Opin Anaesthesiol. 24(4):433-438. DOI:10.1097/aco.0b013e328347f931.
- Anghelescu DL, Burgoyne LL, Liu W, et al. (2008). Safe anesthesia for radiotherapy in pediatric oncology: St. Jude Children`s research hospital experience, 2004-2006. Int J Radiation Oncology Biol Phys. 71(2):491-497. DOI:10.1016/j.ijrobp.2007.09.044.
- Alvarado-Valverde AM, Ramírez-Montero A, Esquivel-González J, Rodríguez-Rodríguez C. (2021). Use of sedation and anesthesia in the pediatrics patients undergoing radiotherapy. Acta Méd Costarric. 63(1):14-20.
- Instituto Nacional de Câncer (Brasil). (2022). Estimativa 2023: incidência de câncer no Brasil. Instituto Nacional de Câncer. Rio de Janeiro: INCA. p. 60-61.
- DeNunzio NJ, Yock TI. (2020). Modern radiotherapy for pediatric brain tumors. Review. Cancers. 12(6):1-16. DOI: 10.3390/cancers12061533.
- Gupta M, Garg R. (2017). Radiation therapy for children: periprocedural anaesthetic concerns. Review Article. J Anesth Crit Care Open Access. 8(2):1-3. DOI: 10.15406/jaccoa.2017.08.00297.
- Harris EA. (2010). Sedation and anesthesia options for pediatric patients in the radiation oncology suite. Int J Pediatr. 2010:870921. DOI:10.1155/2010/870921.
- Owusu-Agyemang P, Grosshans D, Arunkumar R, et al. (2014). Non-invasive anesthesia for children undergoing proton radiation therapy. Radiother Oncol. 111(1):30-34. DOI: 10.1016/j.radonc.2014.01.016.
- Patel SS, Goa KL. (1996). Sevoflurane. A review of its pharmacodynamic and pharmacokinetic properties and its clinical use in general anaesthesia. Drugs. 51(4):658-700.
- Thomas M, Morrison C, Newton R, Schindler E. (2018). Consensus statement on clear fluids fasting for elective pediatric general anesthesia. Paediatr Anaesth. 28(5):411-414. DOI: 10.1111/pan.13370.