Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2024
Non-vital Tooth Bleaching from Root Canal Retreatment to Restoration: A Case Report
Amira Kikly1, Sabra Jaâfoura2, Emna Garouachi3, Neila Zokkar4, Nabiha Douki4,*
1Associate Professor, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
2Associate Professor, Department of Dental Biomaterials, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Laboratory of Dento-Facial, Clinical and Biological Approach (ABCDF) LR12ES10, University of Monastir, Tunisia
3Department of Dentistry, university hospital, Sahloul, Faculty of Dental Medicine, University of Monastir, Research Laboratory LR12ES11, Tunisia
4Professor, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
*Corresponding Author: Nabiha Douki, Professor, Professor, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia; Email: [email protected]
Received Date: February 7, 2024
Publication Date: March 22, 2024
Citation: Kikly A, et al. (2024). Non-vital Tooth Bleaching from Root Canal Retreatment to Restoration: A Case Report. Mathews J Dentistry. 8(1):45.
Copyright: Kikly A, et al. © (2024)
ABSTRACT
Today, the concept of a beautiful smile is all about white teeth. Several solutions can be proposed to reduce dyschromia of non-vital teeth. Internal bleaching is the least mutilating technique. This technique gives good results if the indications are well defined, the operative protocol followed and the precautions taken. Internal bleaching uses bleaching agents placed in the pulp chamber, possibly supplemented by ambulatory bleaching with carbamide peroxide. The aim of this paper is to present, through a case study, the various clinical steps involved in the management of a dyschromic non-vital anterior tooth.
Keywords: Pulpless tooth, Internal bleaching, sodium perborate, Carbamide peroxide
INTRODUCTION
Since time immemorial, people have been striving to find the secret of a miracle recipe to achieve a much-desired lightening effect. Several solutions can be proposed to reduce the discoloration of pulpless teeth. Dental dyschromia resulting from trauma is the most common. Tooth discoloration occurs either as a result of degeneration of the necrotic pulp parenchyma, or as a result of pulp hemorrhage invading the dentinal tubules. Hemolysis then releases hemoglobin, which in turn releases various products responsible for different stains. The internal bleaching technique is the least mutilating. It consists of internally bleaching a devitalized tooth with little or no decay. This is achieved by placing bleaching agents in the pulp chamber, possibly supplemented by the use of a night splint. Hydrogen peroxide can be used as a bleaching agent with or without activation. Sodium perborate is the most recommended bleaching agent. It is an oxidizing product applied intracoronally after careful cleaning. This technique gives good results if the indications are well defined, the surgical protocol well respected and precautions well taken. Therapeutics for thinning pulpless teeth give excellent results, but care must be taken in choosing the method used. Establishing the indication is the most precise procedure, and the technique is straightforward, but must remain under the practitioner's watchful eye throughout the treatment [1,2].
The aim of this paper is to present, through a case report, the various clinical steps involved in the treatment of a dyschromic pulpless anterior tooth.
CASE REPORT
This is a 28-year-old female patient who consulted the dental medicine department of Sahloul hospital, Tunisia, for aesthetic discomfort related to a dyschromic right central incisor (11) (Figure 1). Clinical examination revealed previous oral trauma and a coronal amelodentinal fracture in the right central incisor (11) with an old composite resin restoration. Radiological examination revealed inadequate endodontic treatment (Figure 2). Management of the causal tooth included endodontic retreatment (Figure 3) and internal bleaching. The coronal section and access cavity were shaped by reducing the root canal filling apically by 2mm below the enamel-cement junction (Figure 4). A cervical plug of fluid resin was placed (Figure 5). A mixture of sodium perborate and distilled water was then applied (Figure 6), followed by a temporary coronal filling (Figure 7). A check-up was performed at one-week intervals (Figure 8) and the bleaching agent was renewed 5 times (Figure 9).
Finally, 16% carbamide peroxide was used for ambulatory bleaching (Figures 10-12), followed by a composite resin restoration (Figure 13,14).

Figure 1: Preoperative clinical view showing dyschromia and an old, defective restoration on the right central incisor (11).

Figure 2: Retroalveolar radiograph showing defective root canal filling.

Figure 3: Radiograph after endodontic retreatment of the right central incisor (11).

Figure 4: Disobturating the canal 2 mm below the amelo-cementary junction.
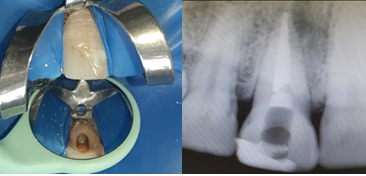
Figure 5: Placement of a fluid resin cervical plug and radiological control.
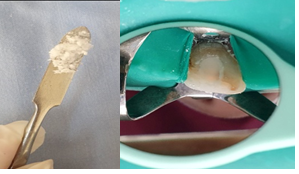
Figure 6: Preparing a mixture of sodium perborate + saline solution (consistency of wet sand) + placement in prepared cavity.

Figure 7: Temporary coronal filling of the tooth.

Figure 8: One-week control.

Figure 9: Result after bleaching agent renewal (5 applications).
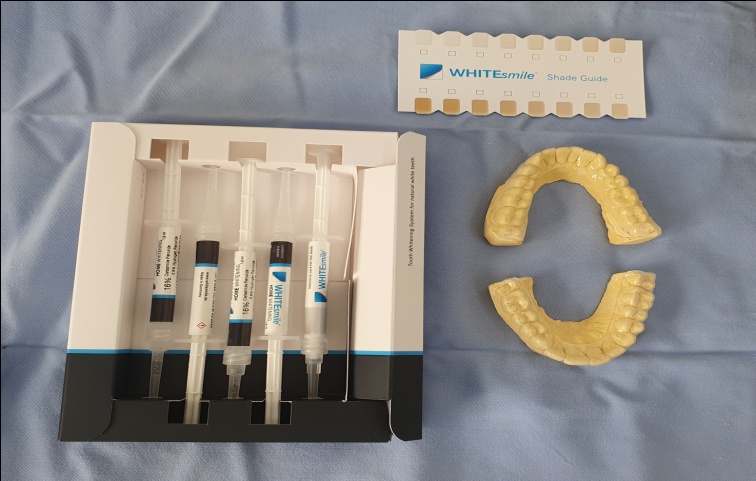
Figure 10: Ambulatory bleaching agent: carbamide peroxide 16%+ thermoformed guard.

Figure 11: Inside-outside technique: bleaching the pulpless tooth and adjacent teeth.

Figure 12: Result after ambulatory bleaching.

Figure 13: Final result after restoration using the anatomical composite resin layering technique.

Figure 14: 12-month follow-up.
DISCUSSION
In the presence of pulpal necrosis, degradation products are liberated and can penetrate the dentinal tubules, resulting in dentin discoloration. This degree of dyschromia correlates with the presence of necrotic tissue over time. During the hemolysis reaction, bacteria produce hydrogen sulfide. This releases the ferric ion from the hemoglobin to form iron sulfide, the main molecule responsible for the dark-gray color of the pulped tooth [2.3].
Bleaching of pulpless teeth using sodium perborate mixed with hydrogen peroxide or saline is a simple, easy, fast and reproducible technique, provided the operating protocol is followed.
The aim of this bleaching technique is to fragment pigmented molecules through oxidation. This result is obtained by the action of an oxidizing agent, which only acts on organic pigments (blood, necrotic residues). It is therefore necessary to specify the etiology of dental dyschromia during a meticulous clinical examination [1].
The patient will be asked questions about the history of the dyschromic tooth. A specific medical questionnaire may also be proposed. The endobuccal clinical examination will first focus on the soft tissues surrounding the tooth. It is essential to check for spontaneous inflammation or bleeding of the gingiva. Both are signs of good oral hygiene.
In order to better study the tooth in question, it is preferable to clean it beforehand, using a brush and polishing paste, to remove any extrinsic stains staining the tooth. This will make it easier to determine the etiology of the discoloration. The initial color of the discoloured tooth needs to be defined. This can be done with the help of shade guides. Photography is also an excellent tool for checking the progress of treatment step by step, and thus better assessing its effectiveness [4.5]. The radiological examination is essential before starting the treatment to bleach the pulpless tooth, as it enables us to confirm the clinical observations, check for the absence of carious lesions that could not be detected clinically, assess the extent of composite restorations and their condition, visualize the integrity of the dental root and finally observe the quality of the root canal filling, which must be densely sealed and three-dimensional.
Before starting treatment, the patient should be aware of the limitations and risks involved, such as treatment failure or risks to the tooth itself, and that no guarantee of results is possible [4,6]. The patient also needs to be motivated, as it is impossible to predict in advance how many times the bleaching treatment will have to be renewed in the pulp chamber.
Exposing the root canal entrance creates space for the application of root sealing material. The root canal filling must be reduced by 2mm apically below the enamel-cement junction.
The use of a ball bur or heated instrument has been recommended. A millimeter probe, measuring the distance between the bottom of the cavity and the incisal edge, enables us to check this length vestibularly. Alternatively, this distance can be measured using tweezers, the edges of which are placed inside and outside the vestibular part of the cavity. The use of a cervical plug, based on fluid resin or glass ionomer cement, is designed to prevent the penetration of the bleaching agent into the periodontium via the dentinal tubules. It protects the cement-amel junction from the risk of external cervical resorption. It's important to locate the protective barrier correctly. A high position increases the risk of external cervical resorptions, while a low position prevents bleaching. The sodium perborate-distilled water mixture is renewed every week until the desired color is achieved [7,8].
It is recommended that the color of the bleached tooth should be slightly lighter than that of the adjacent teeth, to avoid a possible relapse of color in the days that follow. Indeed, even if the bleaching agent is removed from the tooth, oxygen residues remain, leading to changes in the optical qualities of the tooth [9]. It is essential to neutralize by applying a calcium hydroxide paste for 10 days, to improve adhesion of the final coronal restoration. A two-week delay is required for the final composite resin restoration (waiting for color stabilization). At present, catalase can be used to eliminate oxygenated residues, enabling immediate definitive coronal restoration. A combination of intracoronal and extracoronal applications of 16% carbamide peroxide was an effective bleaching technique for pulpless teeth with dyschromia. In fact, the internal-external technique provides better aesthetic results [10].
CONCLUSION
At present, the scientific consensus is that the ambulatory method, using sodium perborate combined with distilled water, remains a safe method. It is easy to use, economical, painless and safe for the tooth. It also offers highly satisfactory results in cases of simple dyschromia.
The use of hydrogen peroxide, carbamide peroxide, light or heat activators in internal bleaching techniques for discolored teeth considerably increases the risk of external cervical resorption. These pathologies, which are unfortunately difficult to control, compromise tooth preservation in the short to medium term. The practitioner must always choose the technique best suited to each case, and the least mutilating. So it's vital to maintain professional control over bleaching techniques.
REFERENCES
- Charis Frank A, Kanzow PH, Rödig T, Wiegand A. (2022). Comparison of the Bleaching Efficacy of Different Agents Used for Internal Bleaching: A Systematic Review and Meta-Analysis. J Endod. 48(2):171-178.
- Barakah R, Alwakeel R. (2019). Non-vital Endo Treated Tooth Bleaching with Sodium Perborate. Curr Health Sci J. 45(3):329-332.
- Pandey SH, Patni PM, Jain P, Chaturvedi A. (2018). Management of intrinsic discoloration using walking bleach technique in maxillary central incisors. Clujul Med. 91(2):229-233.
- Zimmerli B, Jeger F, Lussi A. (2010). Bleaching of nonvital teeth. A clinically relevant literature review. Schweiz Monatsschr Zahnmed. 120(4):306-320.
- Patil AG, Hiremath V, Kumar RS, Sheetal A, Nagaral S. (2014). Bleaching of a nonvital anterior tooth to remove the intrinsic discoloration.J Nat Sci Biol Med. 5(2):476-479.
- Dahl JE, Pallesen U. (2007). Bleaching of the discolored traumatized tooth. In : Andreasen F, Andreasen J, Andersson L, eds. Textbook and color atlas of traumatic injuries to the teeth. Oxford: Blackwell. 2007:852-860.
- Chng HK, Yap AU, Wattanapayungkul P, Sim CP. (2004). Effect of traditional and alternative intracoronal bleaching agents on microhardness of human dentine. J Oral Rehabil. 31(8):811-6.
- Cavalli V, Shinohara MS, Ambrose W, Malafaia FM, Pereira PN, Giannini M. (2009). Influence of intracoronal bleaching agents on the ultimate strength and ultrastructure morphology of dentine. Int Endod J. 42(7):568-575.
- Setien VJ, Roshan S, Nelson PW. (2008). Clinical management of discolored teeth. Gen Dent. 56(3):294-300.
- He AM, Liu QL, Wang Y. (2010). Bleaching of non-vital discolored tooth: clinical analysis of 30 cases. Shanghai Kou Qiang Yi Xue. 19(2):129-132.