Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2022
Nephroprotective Activity of an Aqueous Extract of Alchornea Cordifolia Stapf. (Euphorbiaceae) on Acute Kidney Injury Induced by Paracetamol in Rat
Iriga Trobich GNAKO, Arsene MEA*, Yapi Romaric EKISSI, Kouakou Jean-Claude ABO
Laboratory of Biology and Health, Felix Houphouët Boigny University, Abidjan, Côte d’Ivoire
*Corresponding author: Arsene MEA, Laboratory of Biology and Health, Felix Houphouët Boigny University, Abidjan, Côte d’Ivoire, Phone: +2250707757913; Email: [email protected]
Received Date: June 14, 2022
Published Date: December 07, 2022
Citation: Arsene MEA, et al. (2022). Nephroprotective Activity of an Aqueous Extract of Alchornea Cordifolia Stapf. (Euphorbiaceae) on Acute Kidney Injury Induced by Paracetamol in Rat. Mathews J Pharma Sci. 6(1):10.
Copyrights: Arsene MEA, et al. © (2022).
ABSTRACT
Paracetamol, an analgesic frequently used by patients in poor countries because it is cheaper and available by self-medication on all markets. Its excessive consumption induces proven kidney and liver damage. As an indicator of the state of renal function, the serum level of urea, creatinine, and total protein are considered reliable markers. Thus, an increase in blood urea and serum creatinine followed by a decrease in total serum protein levels is indicative of kidney damage. During this study, the rats which received 1000 mg/Kg of paracetamol died on the fourth and fifth day of experimentation. The analyzes show an increase in the level of urea and serum creatinine of more than 150% and a decrease in total proteins of more than 150%. The rate thus goes from 0.288 g/l to 0.720 g/l for urea; from 7.307 mg/l to 18.267 mg/l for creatinine and from 57.168 g/l to 14.292 g/l for total proteins. This suggests nephrotoxicity in rats. In the rats which received 250 and 500 mg/Kg of paracetamol, the serum level of urea which was 0.288 g/l, goes to 0.452 g/l and 0.661 g/l respectively; an increase of 58.07% and 129.60%. The serum creatinine level is 7.307 mg/l in normal rats. This rate goes from 7.705 mg/l and 8.450 mg/l respectively. That is an increase of 5.16% and 15.64%. The total proteins in the normal rats had a level of 57.168 g/l, and the treated rats have a serum level of 54.715 g/l and 49.873 g/l respectively, at the end of the experiment. That is a decrease of 4.25% and 12.76% respectively. These parameters are characteristic of the progressive onset of acute renal failure (ARI or ARF). Alchornea cordifolia (Euphorbiaceae) is a plant in the African pharmacopoeia. This plant reduces the serum level of urea and creatinine and brings back the total proteins to their reference value when it is administered in pre-treatment and also in post-treatment. Alchornea cordifolia. Therefore, possesses secondary compounds capable of reducing paracetamol-induced nephrotoxicity in rats.
Keywords: Paracetamol, Alchornea cordifolia, Nephrotoxicity, Serum Level
In many African countries, patients with certain pathologies deemed to be chronic such as cancer, diabetes, cardiovascular disease, and chronic renal failure are cared for by traditional therapists once the hospital diagnosis has been made. The results obtained depend on the state of progress of the pathologies of the patients. However, many convincing and verifiable results are observed every day confirming that natural therapy is the first medicine of humanity. Thus, many patients recover with regularized or improved biological parameters. The use of X-rays and CT can show the anatomic-structural improvements of the affected organs. Acute and chronic renal failure is an increasing pathology in the African population. Many traditional healers claim to treat this pathology. Paracetamol is the best-selling drug in the world, particularly in Africa. It is suspected of being toxic at high doses when taken regularly, affecting certain vital organs.
In Africa, paracetamol is present in more than 80% of drugs sold both in authorized pharmacies and in our self-medication markets. This makes this product the drug most consumed by our population.
In this study, we show how paracetamol administered in high doses induces nephrotoxicity. Then, the effect of Alchornea cordifolia, a plant of the African pharmacopoeia, on renal failure induced by paracetamol.
MATERIAL AND METHODS
Biological material
Plant
Alchornea cordifolia (Euphorbiaceae), is an erect shrub 4 to 5 m long sometimes climbing with numerous branches starting from the base, flared and slightly drooping. The leaves are glabrous, stellate pubescent, alternate broadly ovate, broadened and cordate at the base and with an entire, toothed margin [1]. The plant is widespread in the renewed forests of tropical Africa and in riverine forest. It is found on marshy or dry sites and on acidic sands [2].
Alchornea cordifolia is used fresh or dried, in all its organs, alone or in association with other plants in the pharmacopoeia.
Thus, the decoction of the leaves treats dysentery and stomach aches. In girls of puberty age and adult women this decoction serves as an intimate toilet. Leaf powder applied topically is a rapid healer of wounds and ulcers [3]. Its anti-dermatophyte and antimicrobial properties have been demonstrated by authors [4]. Stem bark has antimicrobial activity against Staphylococcus aureus, Bacillus subtilis, Escherichia coli, and Klebsiella pneumoniae [5]. The plant has antifungal activity on Microsporon canis and Trichophyton mentagrophytes [6].
The leaves used were identified at the national center of floristics (N.C.F.) housed within the Félix Houphouet-Boigny University of Abidjan-Cocody
Animals
The animal sample consists of 80 nulliparous and non-pregnant female rats (Rattus norgevicus) of the Wistar strain weighing between 120 and 150 g. The animals are fed pellets provided by an animal feed company, tap water and benefited from day and night light. The rats are bred in the Animal Physiology Laboratory of the Félix Houphouet-Boigny University. All procedures comply with animal health and use standards published by the National Institute of Public and Animal Health of Côte d'Ivoire and international standards for the use of laboratory animals.
Technical material
The work required the use of a Vacutherm Vacuum Oven brand oven (France) for drying the total leaf extract. Pasteur pipette for blood collection. The samples are analyzed using a Cobas Hitachi C311 turbidimeter (immuno-turbidimeter, Roche, Germany) and various other small laboratory equipment.
Methods
Preparation of the aqueous extract of Alchornea cordifolia (AEAc)
Alchornea cordifolia leaves are dried at room temperature (31 to 32°C). They are reduced to powder. One hundred grams (100 g) of this powder are weighed and boiled for 15 minutes in 1 liter of distilled water. After cooling, the decoction is filtered on cotton, then on Wattman filter paper n°2 according to a proven method [7]. The filtrate obtained is dried in a Vacutherm Vacuum Oven brand oven (France) at 40°C. The dry pellet is scraped and crushed according to the method provided by the authors [8]. A brown powder is obtained and constitutes the aqueous extract of Alchornea cordifolia (Euphorbiaceae) (AEAc) which will be weighed and diluted to constitute the different doses.
Method of induction of IRA by paracetamol
To determine the dose of paracetamol that induces failure without killing the animals, we used a method proven by some authors [9].
Before any treatment, the measured biochemical parameters of study were determined: urea, creatinine and total proteins. All measured parameters were recorded on all animals. The various treatments are carried out by force-feeding.
Forty (40) fingerlings are divided into 4 batches of 10 fingerlings. The animals fasted for 12 hours before the treatment. The animals are fed appropriately for days following the treatment and received different doses at the same time once a day for 7 days.
For this, the forty (40) rattles will be subdivided into two sub-groups (SG1 and SG2) with twenty (20) rattles in each group, comprising 4 batches of five (5) rattles.
-The subgroup (SG1) of twenty (20) rats is used for oral toxicity tests and the dose effect of paracetamol on biochemical parameters. The animals only receive different doses of paracetamol. This is the induction subgroup of acute renal failure (AKI). Thus, the behaviour, mortality, and biochemical parameters of rats are recorded at the end of the experiment, which lasts one week (7 days). Thereby:
- Batch 1, receives 1ml of distilled water
- Batch 2, receives 1 ml of 250 mg/ml of paracetamol
- Batch 3, receives 1 ml of 500 mg/ml of paracetamol
- Batch 4, receives 1ml of 1000 mg/ml of paracetamol
-The subgroup (SG2) of twenty (20) rats will be used for post-treatment with the extract of (AEAc). Thus, the animals will first receive the doses of paracetamol; and thereafter, at 1 hour after the initial dose of AEAc. Here, the positive control is batch 1 treated with paracetamol which does not receive AEAc. Therefore:
- Batch 1, receives 1ml of 500 mg/ml of paracetamol (positive control; PC)
- Batch 2, receives 1 ml of 250 mg/ml of paracetamol then 1 hour after AEAc
- Batch 3, receives 1 ml of 500 mg/ml of paracetamol then 1 hour after AEAc
- Batch 4, receives 1ml of 1000 mg/ml of paracetamol then 1 hour after AEAc
Method of treatment with aqueous extract of Alchornea cordifolia (AEAc)
Forty (40) rats are divided into 4 batches of 10 rats fasted before treatment. Then the forty (40) rats will be subdivided into two sub-groups (SG1 and SG2), twenty (20) rats with each group comprising the 4 previous batches. Each subgroup lot includes five (5) rattles.
Then perceive by force-feeding:
-The first subgroup (SG1) of twenty (20) rats makes it possible to determine the dose-response effect of AEAc on behavior, toxicity and biochemical parameters. These animals are gavaged:
- Batch 1, receives 1 ml of distilled water (Control)
- Batch 2, receives 1 ml of 200 mg/ml of AEAc
- Batch 3, receives 1 ml of 500 mg/ml of AEAc
- Batch 4, receives 1 ml of 1000 mg/ml of AEAc
The second subgroup (SG2) of twenty (20) rats allows pre-treatment with paracetamol. Thus, the rats treated with AEAc will receive the following, 1 hour after the doses of paracetamol:
- Batch 1, receives 1 ml of 500 mg/ml of AEAc (positive control PC)
- Batch 2, receives 1 ml of 200 mg/ml of AEAc then paracetamol
- Batch 3, receives 1 ml of 500 mg/ml of AEAc then paracetamol
- Batch 4, receives 1 ml of 1000 mg/ml of AEAc then paracetamol
Method for assaying biological or biochemical parameters
The colorimetric creatinine assay method was used. Creatinine in alkaline solution reacts with picrate to form an orange-yellow complex. Picric acid (17.5 mmol/l) and sodium hydroxide (0.29 mmol/l) are therefore used as reagents. The complex (product) is read at the wavelength of 492 nm. The reagent serves as reference (zero).
The urea assay method was done kinetically. Urea is hydrolyzed by urease to ammonia and carbon dioxide. The second reaction catalyzed by glutamate dehydrogenase converts ammonia and α-ketoglutarate to glutamate and water with simultaneous oxidation of reduced nicotinamide-adenine-dinucleotide to nicotinamide-adenine-dinucleotide. The decrease in optical density at 340 nm is proportional to the urea concentration of the sample according to the method described by certain authors [10]. The proteins react with copper sulphate in Biuret's reagent to form a blue-violet complex that can be quantified by a spectrometer at a wavelength of 550 nm. The intensity of the staining of the complex is proportional to the total proteins of the sample according to the method provided by the authors [11].
Determination of secondary compounds of AEAc
The staining test in different tubes with different reagents according to the method of Wagner and Bladt [12] revised by Gabriela et al. [13] then improved by Mea et al. [14] makes it possible to determine the presence of secondary compounds.
Blood collection
A blood sample was obtained at 24 hours after the administration of the last different doses in all animals of the same batch by using a Pasteur pipette containing 1 ml of 9‰ sodium chloride, at the level of the retro-orbital sinus. of the eye. The recovered blood was centrifuged at 3000 revolutions/min. for 15 minutes. The serum was collected in EDTA tubes and stored at -20°C. for the analysis of biochemical parameters.
Pharmacological substances
- Paracetamol in tablet of 500 mg
- Ethyl ether (ETHER Gifrer)
- Sodium chloride 9‰
Statistical analysis
GraphPad Prism 5 and GraphPad InStat 5 scientific software were used to produce the graphs and analyze the results. The values are given as means with the standard errors (MEAN+SEM) and the difference between the values was determined by the Student-Newman-Keuls comparison test. This allowed us to consider a probability > 5% (p> 0.05) not significant, a probability < 5% (p< 0.05⁎) significant, a probability <1% (p<0.01⁎⁎) very significant and a probability < 0 .1% (p<0.001⁎⁎⁎) more significant.
RESULTS
Determination of secondary compounds
Phytochemical screening showed the presence of sterol and polyterpenoid compounds, polyphenols, flavonoids, saponosides, alkaloids, quinones, and catechuic tanins. There is an absence of galenic tanins (Table 1).
Table 1. Phytochemical screening of the aqueous extract of Alchornea cordifolia (AEAc).
|
Compounds searched |
Result |
|
|
Sterols and polyterpenoid |
+ |
|
|
Polyphenols |
+ |
|
|
Flavonoids |
+ |
|
|
Quinones |
+ |
|
|
Saponosides |
+ |
|
|
Catechuic |
+ |
|
|
Tanins |
Gallic |
- |
The animals were divided into four (4) groups of five (5) rats, as described in the methodology section (SG1).
The animals receive 1 ml of distilled water (batch 1) then 1 ml of 250 mg (batch 2), 1 ml of 500 mg (batch 3) and 1 ml of 1000 mg (batch 4) of paracetamol.
On the fourth day, two (2) rats of batch 4 died. On the fifth day (D5), all the animals in batch 4 died. At the end of the experiment, there was no live rat from batch 4. Serum samples on D5 showed an exaggerated increase in creatinine and urea levels of around 150% and the total protein level decreased by 150%.
In fact, in animals before treatment, the average urea level was 0.288+/-0.062 g/l, creatinine 7.307 =/- 1.648 mg/l, and total protein 57.164±1.27 g/l.
At the end of the experiment, which lasts one week, i.e., seven (7) days, significant modifications were observed in the serum biochemical parameters in the treated rats.
The creatinine levels of the animals of batches 2 and 3 which received 250 and 500 mg of paracetamol were 7.780 =/- 1.493 and 8.452 +/- 0.281 mg/l, respectively, an increase of 06.47% (p>0.05) and 15% (p<0.01).
While the urea rate went from 0.288±0.061 to 0.452 ±0.030 g/l and 0.661 ±0.065 g/l; an increase of 56.94% (p<0.01) and 129% (p<0.001).
The total protein increase was 54.715 g/l and 49.872 g/l; i.e., an increase of 04.28% (p>0.05) and 12.75% (p<0.05). Table 2 gives a summary of this experience on D7.
Table 2. Induction of acute renal failure (ARI) by paracetamol in one week.
|
|
Control |
Para 250 |
Para 500 |
Para 1000 |
|
Urea (g/l) x 100 |
28.80±2.10 |
45.20±3.05* |
66.10±6.50*** |
---------- |
|
Creat mg/ml) x10 |
73.07±6.48 |
77.80±4.30 |
84.52±9.81** |
---------- |
|
Tot. Prot. (g/l) |
57.16±1.57 |
54.71±1.82 |
49.87±1.03* |
----------- |
Table 2 shows that the dose of 500 mg daily for one week induces hepatotoxicity in rats. There was an installation of acute renal failure (ARI).
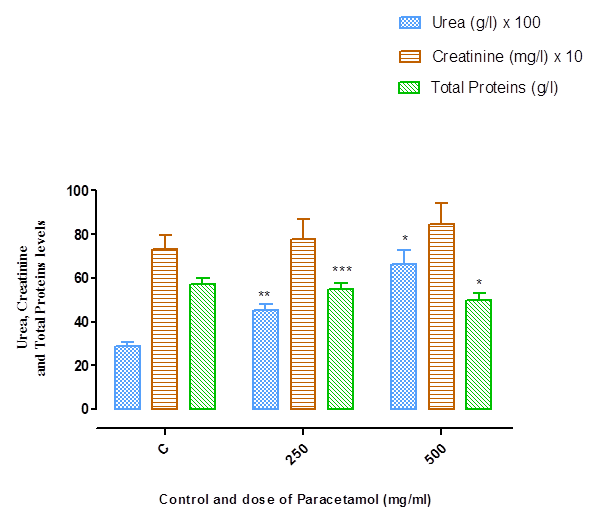
Figure 1. Shows the evolution of the biochemical parameters according to the dose of paracetamol.
Dose-response effects of AEAc on serum biochemical parameters
In this experiment twenty (20) rattles are divided into four batches of five (5) rattles. As notified by protocol (SG1).
The control group consisted of rats that received 1 ml of distilled water.
The animals of batches 2, 3 and 4 received 1 ml of 250 mg, 1 ml of 500 mg and 1 ml of 1000 mg of aqueous extract of AEAc, respectively.
The measured biochemical parameters were urea, creatinine, and total proteins in the animals before treatment and in the control animals were 0.288 ± 0.021 g/l, 7.307 ± 1.648 mg/l, and 57.164 +/- 1.570 g/l, respectively.
At a dose of 250 mg/ml of AEAc, the rate went from 0.288 ± 0.021 g/l to 0.239 ± 0.025 g/l for urea. This equates to a significant decrease of 17.01%. The creatinine levels went from 7.307±0.648 to 6.794±0.861mg/l. i.e., a non-significant decrease of 7.02%. The Total Protein rate went from 57.164±1.570 to 62.240±4.886 g/l. That is a non-significant increase of 8.88%.
At a dose of 500 mg/ml of AEAc, the urea level, which was 0.288 +/- 0.021, dropped to 0.228 ± 0.025 g/l. which equates to a significant drop of 20.83%. The creatinine levels went from 7.307±0.648 to 6.730±0.861 mg/l. This is equivalent to a non-significant decrease of 7.89%. The total protein rate went from 57.164±1.570 to 65.662±1.756 g/l. This equates to an increase of 14.86%.
At a dose of 1000 mg/ml of AEAc, the urea levels went from 0.288±0.021 to 0.214±0.019 g/l; a significant decrease of 25.69%. The creatinine levels dropped from 7.307±0.648 to 6.310±0.243 mg/l, a significant decrease of 13.64%. Total protein levels went from 57.164±1.570 to 70.731 +/- 4.131 g/l, an increase of 23.73%.
Table 3 summarizes the dose-response effect of AEAc on serum parameters.
Table 3. Dose-response effect of AEAc in serum concentrations of biochemical parameters.
|
|
Control |
AEAc 250 mg/ml |
AEAc 500 mg/ml |
AEAc 1000 mg/ml |
|
Urea (g/l) x100 |
28,80±2,10 |
23,90±2,50 |
22,8±0025 |
21,40±1,9* |
|
Creat. (mg/l) x10 |
73,07±6,48 |
67,94±2,29 |
67,30±8,61 |
63,10±2,43* |
|
Tot. Prot. (g/l) |
57,16±1,57 |
62,24±4,88 |
65,66±1,75 |
70,73±4,13* |
Figure 2 shows the variations in serum urea, creatinine, and total protein concentration as a function of AEAc concentration.
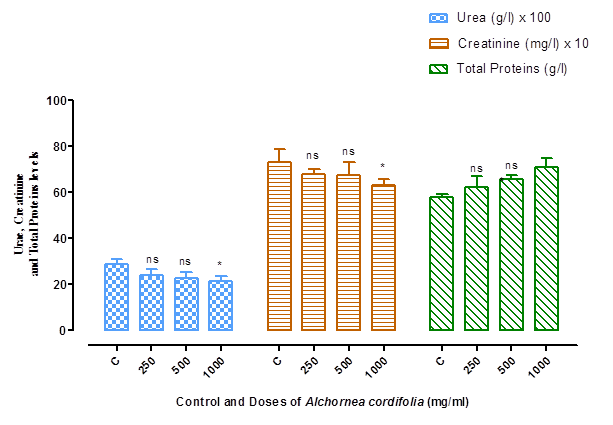
T: control; ns: not significant p<0.05; significant p >0.05*. 250; 500; 1000 [AEAc].
Figure 2. Variation in the serum concentration of urea, creatinine, and total protein concentrations as a function of AEAc concentrations.
The different doses of AEAc at 250 and 500 mg/ml, administered to the animals, significantly improve the serum concentrations of biological parameters (urea, creatinine, and total protein).
The dose of AEAc at 1000 mg/ml significantly lowered the serum concentration of urea and creatinine. Also, the serum concentration of total proteins increased. This is an indication of a properly functioning lever in these animals.
Effects of AEAc on paracetamol-induced acute renal failure (ARI or ARF)
During this experiment, rats first receive paracetamol and then AEAc.
The positive control animals (PC) are those which have been treated with paracetamol alone at a dose of 500 mg. In these animals (positive controls), the biological parameters recorded are successively 0.661±0.065 g/l of urea; 8.452±0.281 mg/l of creatinine, and 49.87±1.033 g/l of total protein. That is an increase of 129.51% in urea, 15.66% in creatinine and a decrease of 15.32% in total proteins.
ARF in pre-treated animals
The rats from the subgroup (SG2) first received AEAc. The animals received the aqueous extract of Alchornea cordifolia at 250, 500, and 1000 mg/ml, respectively, 1 hour before the administration of paracetamol for 7 days.
In pre-treated animals, the serum concentration of urea, creatinine, and total proteins is 0.483±0.014 g/l, 5.706±0.424 mg/l and 57.51±2.023 g/l, respectively.
When compared to positive controls, this equates to decreases of 26.92%; 25.91%, and a 0.61% increase in urea, creatinine, and total protein, respectively.
ARF in post-treated animals
These animals first receive paracetamol 500 mg. Then, each animal received AEAc one hour after. The serum levels of the biochemical parameters were 0.504 +/- 0.014 g/l; 4.504±0.150 mg/l and 57.51 +/- 2.023 g/l for urea, creatinine and total proteins, respectively. This equates to a 75% increase in urea and decreases in creatinine levels of 38.36% and 6.94% in total protein.
Table 4. Shows the different variations in serum concentrations of biochemical parameters (urea, creatinine and total protein) in pre-treated and post-treated animals.
|
Normal Control |
Positive Control |
Pre-treated |
Post-treated |
|
|
Urea (g/l) x100 |
28,80±6,10 |
66,10±6,50 |
50,40±1,50 |
48,30±1,40 |
|
Creat. (mg/l) x10 |
73,07±6,48 |
84,52±4,93 |
45,04±1,50 |
57,06±4,24 |
|
Tot. Prot. (g/l) |
57,161±1,270 |
49,87±1,033 |
53,192±1,88 |
57,512±2,023 |
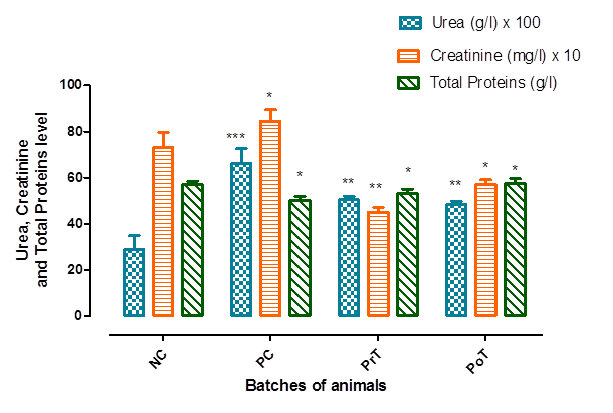
NC: normal control; PC: positive control; PrT: pre-treated; PoT: post-processed
Figure 3. Variation in the serum concentration of biochemical parameters (urea, creatinine, and total proteins) according to the batches of pre-treated and post-treated animals.
Figure 3 presents the evolution of the different biochemical parameter levels (urea creatinine and total proteins) in animals pre-treated and post-treated with AEAc.
In the positive control, the serum urea level was very significant (***p<0.001) compared to the normal control, that of creatinine was significant (*p<0.05) and that of total proteins was significant compared to the normal control (*p<0.05).
In the pre-treated animals, the serum urea concentration was quite significant compared to the positive control (**p<0.01); that of creatinine was also quite significant (**p<0.01), and the concentration of total proteins was significant compared to the positive control (*p<0.05).
In the post-treated animals, serum urea concentration was quite significant (**p<0.01) compared to the positive control; also significant for creatinine (*p<0.05) as well as the concentration of total proteins (*p<0.05) when compared to the positive control.
DISCUSSION
The determination of urea, total proteins and creatinine are reliable serum markers of renal activity [15]. Thus, an increase in serum creatinine and urea levels accompanied by a decrease in total protein is characteristic of kidney damage.
The level of urea in plasma depends on the balance between renal production and excretion. Urea is in fact excreted 90% by the kidneys and 10% by the intestinal tract and the skin.
Blood urea is increased in kidney damage such as glomerulonephritis, pyelonephritis and ischemia [16].
Acute renal failure or the term acute renal failure (ARF) has been replaced by the term acute kidney injury (AKI) which better expresses the fact that it is not just an increase in creatinine but a spectrum of symptoms associated with an abrupt decline in kidney function. This syndrome is characterized by reduced glomerular filtration rate (GFR), retention of urea and other metabolic products such as uric acid or ammonia, as well as dysregulation of extracellular volume and electrolytes [17]. Creatinine is a product of muscle catabolism which is eliminated at a constant concentration and rate by the kidney. Also, serum creatinine levels increase when renal function is impaired [18].
The results of the rats force-fed with paracetamol led to the death of all the animals having received 1000 mg/Kg of paracetamol. before the end of the experiment (one week). The dosage of their sample showed very high levels of serum creatinine and urea, indicating kidney damage. Acute nephropathy (APN) is defined as a rapid and sustained deterioration in glomerular filtration and tubular excretion/reabsorption, associated with the accumulation of waste products such as urea or creatinine [19,20].
These observations are similar to the work of other authors who have induced AKI with cadmium and gentamicin [21]. These authors have observed nephroprotective activity of plant extracts on induced renal failure [22].
Administration of an aqueous extract of Alchornea cordifolia (AEAc) improves serum concentrations of creatinine, urea, and total protein. It can therefore be said that AEAc has nephroprotective activity. The nephroprotective activity of the aqueous extract of Alchornea cordifolia (AEAc) is expressed by an improvement in the serum level of urea which is the end product of protein catabolism.
CONCLUSION
This work led to the conclusion that the aqueous extract of Alchornea cordifolia has a protective effect on the kidney in normal animals and a curative effect on the diseased kidney following induced renal failure. This justifies its use in traditional African pharmacopoeia.
REFERENCES
- Pauwels L. (1993). Nzayilu N’ti: Guide des arbres et arbustes de la région de Kinshasa (Brazzaville). Ed Jardin Botanique de Belgique. 14(5):490.
- Adjanohoun EJ. (1994). Fiche espèce: Alchornea cordifolia. Bull Med Trad Pharm. 8(2):203-213.
- Bouquet A, Debray M. (1974). Plantes médicinales de Côte d’Ivoire. Imprimérie Louis Jean, Paris (France). p 232.
- Dibong SD, Mpondo ME, Ngoye A, Kwin NF. (2011). Plantes médicinales utilisées par les populations Bassa de la région de Douala au Cameroun. Int J Biol Chem Sci. 5(3):1105-1117.
- Ebi GC. (2001). Antimalarial activities of Alchornea cordifolia. Fitoterapia. 72(1):69-72.
- Barry MS, Oulalé K, CamaraN, Vuetinck AJ, Vanden BD, Balde AM. (2002). Evaluation de l’activité antifongique de plantes à usage populaire en Guinée. Poster du symposium international sur la chimie et la pharmacologie des plantes utilisées en médecine traditionnelle en Afrique ; 6-8 Mars à Bamako (Mali).
- Kahou Bi GP, Abo KJC, Mea A, Irie Bi JS., Karou TG. (2016). Antidiabetic and Hypolipemic Effects of vtotal aqueous extract of Pseudarthria hookeri Wight & Arn. (Fabaceae) on hemoglobin glycation in aloxan induced diabetic rats. IJPPR. 7(4):145-156.
- Placide EA, Arsene M, Parfait KBG, Jean SIB, Joseph NK, Jean CAK. (2018). Effect of Picralina nitida on the glycemia and intestinal absorption of glucose in rat. GSC Biological and Pharmaceutical Sciences. 05(03):106-114.
- Paoulomi C, Joel M, Subhangar N. (2012). Les effets protecteurs de l’extrait aqueuse de la feuille d’Aloe barbadensis, la gentamicine sur la néphrotoxicité induite par le cisplatine chez les rats. Asian Pacific Journal de biomédecine tropicale. p. 1754-1763.
- Néné-Bi SA, Soro TY, Zahoui OS, Traore F. (2013). Effet d’une administration aigüe d’un extrait aqueux de Bridelia ferruginea Benth. (Euphorbiaceae) sur la fonction rénale chez le rat. Phytothérapie. 11:359-364.
- Doumas BT, Baye DD, Carte RJ, Peter JT, Schaffer R. (1981). A candidate reference methode for determination of total protein in serum. I Developpement and Validation. II Tests for transferability. Clin Chem. 27(10):1642-1654.
- Wagner H, Bladt S. (2001). Plant Drugs Analisis, a Thin Layer Chromatography. 2nd Edition, Springer-Verlag Berlin, Heidelberg, New York, USA.
- Gabriela STM, Angela BA, Gianni S, Antonella S. (2014). Antioxidant Activity of Cosmetic Formulations Based on Novel Extracts from Seeds of Brazilian Araucaria angustifolia (Bertoll) Kuntze. JCDSA. 4(3):190-202.
- Mea A, Ekissi YHR, Abo KJC, Kahou Bi GP. (2017). Hypoglycaemiant and anti-hyperglycaemiant effect of Justicia secunda M. Vahl (Acanthaceae) on glycaemia in the wistar rat. IJDR. 7(6):13178-13184.
- Adelman RD, Spangler WL, Beasom F, Ishizaki G, Conzelman GM. (1981). Frusemide enhancement of netilmicin nephrotoxity in dogs. J Antimicrob Chemother. 7(4):431-440.
- Zappitelli M. (2008). Epidemiology and diagnosis of acute Kidney injury. Semin Nephrol. 28(5):436-446.
- Park S, Baek SH, Ahn S, Lee KH, Hwang H, Ryu J, et al. (2018). Impact of electronic acute kidney injury (AKI) alerts with automated nephrologist consultation on detection and severity of AKI: A quality improvement study. Am J Kidney Dis. 71(1):9-19.
- Couchoud C, Pozet N, Labeeuw M, Pouteil-Noble C. (1999). Screening early renal failure: Cut-off values for serum creatinine as an indicator of renal impairment. Kidney Int J. 55(5):1878-1884.
- Bellomo R, Ronco C, Kellum JA, et al. (2004). For the ADQI workgroup. Acute renal failure-Definition, outcome measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the acute dialysis quality initiative (ADQI) group. Crit Care. 8(4):R204-R212.
- Vandenberghe W, De Loor J, Hoste EAJ. (2017). Diagnosis of cardiac surgery–associated acute kidney injury from functional to damage biomarkers. Curr Opin Anesthesiol. 30(1):66-75.
- Cheyron D, Terzi N, Charbonneau P. (2008). New biomarkers for diagnosis and prognosis of acute kidney injury. Réanimation. 17(8):775-782.
- Adama L, Lambouado FL, Guissou IP, Nikiema JB. (2010). Traditional medecine in kidney diseases in Burkina Faso. Nephrol Ther. 6:35-39.