Information Links
Related Conferences
Previous Issues Volume 4, Issue 1 - 2023
Myocarditis in a Patient with Diabetic Ketoacidosis: A Case Report
Fatima Saeed*, Geetanjali Gupta, Ayesha Javaid
Manchester Royal Infirmary, England
*Corresponding author: Dr. Fatima Saeed, Manchester Royal Infirmary, England, Tel: 07375737352, Email: [email protected].
Received Date: May 20, 2023
Published Date: June 12, 2023
Citation: Saeed F, et al. (2023). Myocarditis in a Patient with Diabetic Ketoacidosis: A Case Report. Mathews J Anesth. 4(1):12.
Copyrights: Saeed F, et al. © (2023).
ABSTRACT
A case of diabetic ketoacidosis (DKA) complicated by acute myocarditis, which was confirmed by Cardiac MRI. A 27-year-old man with diagnosed type 1 diabetes mellitus was hospitalized with severe DKA, blood sugar on admission was 69.3mmol/l and Hba1c was 104 mmol/mol. The initial ECG showed no acute changes however later he developed ST-T changes on his ECG associated with a significant troponin rise which raised the possibility of Myocarditis. The coronary angiogram ruled out any coronary artery disease, however the diagnosis of Myopericarditis was confirmed based on the echocardiogram findings and cardiac MRI. Viruses are the most common causative agents of myocarditis, our patient described symptoms of fatigue that might indicate the probable underlying viral infection however the excessive alcohol intake and non-compliance with insulin were the contributing factors towards development of diabetic ketoacidosis. The whole viral screen including parvovirus and covid-19 was negative. The Epstein bar virus (EBV) although weekly positive, with minimal viral load couldn’t account for the patient’s symptoms. Another rare condition that can present with myocarditis is fulminant type 1 diabetes mellitus, which is believed to be non-immune condition causing rapid onset of diabetes mellitus, the exact aetiology is still uncertain, but the presence of islet injury accompanied by myocardial inflammation points towards underlying viral infection as the cause of sudden onset of diabetes mellitus. The auto antibodies for Type 1 DM turn out to be negative in these cases, however in our patient they weren’t done because he was a confirmed Type 1 Diabetic. The patient successfully responded to the symptomatic treatment for DKA, implicating that severe DKA was the cause of myocarditis. He was provided education on Type 1 diabetes mellitus and subsequently discharged without any further complications with future outpatient appointment in cardiology clinic.
Keywords: Myocarditis, Diabetic Ketoacidosis, Fulminant Type 1 Diabetes.
ABBREVIATIONS
DKA: Diabetic Ketoacidosis; EBV: Epstein Bar Virus; ECG: Electrocardiogram; ACS: Acute Coronary Syndrome; CMR: Cardiac Magnetic Resonance; CR: Creatinine; UR: Urea.
INTRODUCTION
Diabetic ketoacidosis (DKA) is a common presentation patients with uncontrolled type 1 DM. Patients presenting with DKA can have subtle ECG changes that include non-specific ST-T changes which resolve after treatment of the acidosis [1]. The ECG changes usually appear within 24 hours of DKA most common is ST segment depression, although there maybe T wave inversions and prolongation of the QT interval [2], sometimes attributed to be secondary to a viral infection.
A rare case of severe diabetic ketoacidosis complicated by myocarditis is described below.
Written signed consent was obtained from the patient.
CASE DESCRIPTION
A 27-year-old male known to have type 1 diabetes mellitus was admitted with vomiting, lethargy, polydipsia, and shortness of breath after a weekend of binge drinking of alcohol. He described that he was feeling unwell for the last few days, had been non-compliant with his insulin for the last few days and had a binge of alcohol for the last few days before presenting to the hospital. He had recently moved to new city and was non-compliant with his insulin. He denied having any other significant past medical history. He was non-smoker, had alcohol consumption of 16 units on average per week with occasional binges on weekends, he denied illicit drug use.
On examination he was a slim looking guy, having Kussmaul breathing, appeared tired and dehydrated. He was found to be acidotic, blood glucose (69.3 mmol/l), high ketones (6+) and was found to be in acute kidney injury, AKI- stage 3 with creatinine of 262 umol/L and eGFR of 28 mL/min/l.73m2, diagnosed with diabetic ketoacidosis (DKA) with acute kidney injury. He was immediately started on treatment as per Joint British Diabetes Societies guideline for DKA, he responded well to the treatment. His AKI started to improve with fluid resuscitation, and intravenous insulin.
On Day 2 of admission on the medical ward, he developed severe epigastric pain associated with burning pain radiating to the upper chest. He was given omeprazole and liquid sodium alginate with calcium carbonate and sodium bicarbonate for suspected dyspeptic symptom, his ECG showed ST segment elevation in leads V2-V6. ECG attached below, ECG on admission showed normal sinus rhyhm.Serial troponins were 99 ng/L and 758 ng/L respectively. Patient was subsequently moved from the medical ward to the cardiology ward and started on treatment for acute coronary syndrome (ACS) in view of new ST-T changes and acute troponin rise. He had the trans-thoracic echocardiogram done which showed severe LVSD with EF of 30%. His coronary angiogram revealed normal coronary arteries with no evidence of obstruction or stenosis therefore the ACS treatment was stopped. Subsequently the diagnosis of probable myocarditis was made pending cardiac magnetic resonance angiogram (CMR). All the viral serology, autoimmune and vasculitis screen was negative. Pending cardiac MRI patient self-discharged from the hospital understanding the risks and consequences with the prescription of colchcine,beta blocker and ACE inhibitor.
However, two days later he re-presented to the emergency department with chest pain got re-admitted at that time his troponin was 239 ng/L. The cardiac magnetic resonance (CMR) showed finding of myopericarditis with mild and apical subendocardial necrosis suggestive of ongoing inflammation, normal left ventricle geometry and function. No significant valve disease, small bilateral pleural effusions, which confirmed the diagnosis of Myopericarditis. The left ventricle size and function had improved compared to the echocardiogram before indicative of rapid and complete recovery He was started on Ace inhibitor, beta blocker, colchicine, basal bolus insulin regime with short acting Novorapid insulin TDS and long-acting Lantus insulin OD. His troponin had reduced to 19 ng/L and the AKI had resolved, the graph below shows the trend of the troponin, and he was then discharged, to be followed up in the heart Failure clinic and diabetes outpatient clinic.
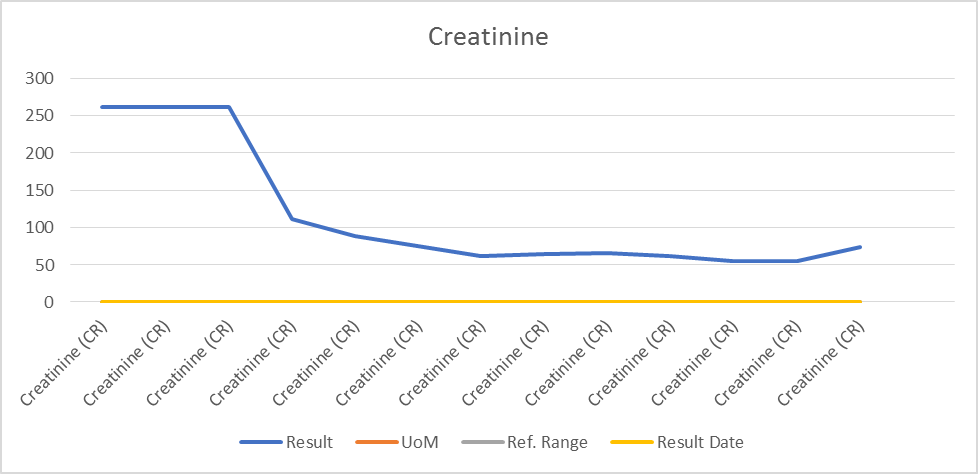
Investigations
|
Test |
Result |
UoM |
Ref. Range |
Result Date |
|
Creatinine (CR) |
262 |
umol/L |
59 -104 |
26-Apr-202108:53 |
|
Creatinine (CR) |
262 |
umol/L |
59 - 104 |
26-Apr-202108:41 |
|
Creatinine (CR) |
262 |
umol/L |
59 - 104 |
26-Apr-202108:43 |
|
Creatinine (CR) |
111 |
umol/L |
59 - 104 |
27-Apr-202100:44 |
|
Creatinine (CR) |
88 |
umol/L |
59 -104 |
27-Apr-202112:33 |
|
Creatinine (CR) |
75 |
umol/L |
59 - 104 |
27-Apr-202123:33 |
|
Creatinine (CR) |
61 |
umol/L |
59 - 104 |
29-Apr-202120:23 |
|
Creatinine (CR) |
64 |
umol/L |
59 -104 |
29-Apr-202111:59 |
|
Creatinine (CR) |
66 |
umol/L |
59 -104 |
01-May-202117:14 |
|
Creatinine (CR) |
62 |
umol/L |
59 -104 |
02-May-202108:25 |
|
Creatinine (CR) |
55 |
umol/L |
59 -104 |
03-May-202110:08 |
|
Creatinine (CR) |
55 |
umol/L |
59 -104 |
03-May-202110:06 |
|
Creatinine (CR) |
74 |
umol/L |
59 - 104 |
05-May-202109:40 |
|
Test |
Result |
UoM |
Ref. Range |
Result Date |
|
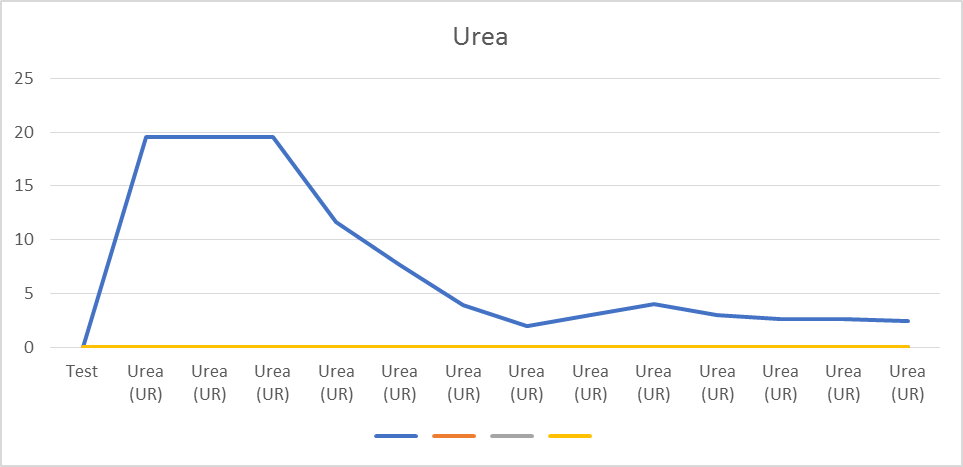
Urea (UR) |
19.5 |
mmol/L |
2.5 - 7.8 |
26-Apr-20210S:43 |
|
Urea (UR) |
19.5 |
mmol/L |
2.5 - 7.8 |
26-Apr-20210S:53 |
|
Urea (UR) |
19.5 |
mmol/L |
2.5 - 7.8 |
26-Apr-20210S:41 |
|
Urea (UR) |
11.6 |
mmol/L |
2.5 - 7.8 |
27-Apr-202100:44 |
|
Urea (UR) |
7.6 |
mmol/L |
2.5 - 7.8 |
27-Apr-202112:33 |
|
Urea (UR) |
3.9 |
mmol/L |
2.5 - 7.8 |
27-Apr-202123:33 |
|
Urea (UR) |
2 |
mmol/L |
2.5 - 7.8 |
29-Apr-202120:23 |
|
Urea (UR) |
3 |
mmol/L |
2.5 - 7.8 |
29-Apr-202111:59 |
|
Urea (UR) |
4 |
mmol/L |
2.5 - 7.8 |
01-May-202117:14 |
|
Urea (UR) |
3 |
mmol/L |
2.5 - 7.8 |
02-May-20210S:25 |
|
Urea (UR) |
2.6 |
mmol/L |
2.5 - 7.8 |
03-May-202110:0S |
|
Urea (UR) |
2.6 |
mmol/L |
2.5 - 7.8 |
03-May-202110:06 |
|
Urea (UR) |
2.4 |
mmol/L |
2.5 - 7.8 |
05-May-202109:40 |
|
Test |
Result |
UoM |
Result Date |
|
eGFR |
28 |
mL/min/l.73m A2 |
26-04-2021 07:37 |
|
eGFR |
78 |
mL/min/l.73m A2 |
27-04-2021 07:37 |
|
eGFR |
>90 |
mL/min/l.73m A2 |
29-04-2021 07:37 |
|
eGFR |
>90 |
mL/min/l.73m A2 |
01-05-2021 16:07 |
|
eGFR |
>90 |
mL/min/l.73m A2 |
02-05-2021 06:27 |
|
eGFR |
>90 |
mL/min/l.73m A2 |
03-05-2021 07:17 |
|
eGFR |
>90 |
mL/min/l.73m A2 |
05-05-2021 06:29 |
|
Test |
Result |
UoM |
Ref. Range |
Result Date |
|
Glucose |
>41.6 |
mmol/L |
3.6 - 5.3 |
26-04-2021 07:32 |
|
Glucose |
>41.6 |
mmol/L |
3.6 - 5.3 |
26-04-2021 09:32 |
|
Glucose |
>41.6 |
mmol/L |
3.6 - 5.3 |
26-Apr-202111:55 |
|
Glucose |
30.7 |
mmol/L |
3.6 - 5.3 |
26-Apr-202114:40 |
|
Glucose |
11.9 |
mmol/L |
3.6 - 5.3 |
26-Apr-202119:31 |
|
Glucose |
12.1 |
mmol/L |
3.6 - 5.3 |
26-Apr-202123:52 |
|
Glucose |
6.4 |
mmol/L |
3.6 - 5.3 |
27-Apr-202108:41 |
|
Glucose |
4.8 |
mmol/L |
3.6 - 5.3 |
27-Apr-202122:46 |
|
Test |
Result |
UoM |
Ref. Range |
Result Date |
|
Troponin- T (TNT) |
99 |
ng/L |
0-14 |
27-Apr-202112:33 |
|
Troponin-T (TNT) |
758 |
ng/L |
0-14 |
27-Apr-202114:50 |
|
Troponin- T (TNT) |
758 |
ng/L |
0-14 |
27-Apr-202115:52 |
|
Troponin- T (TNT) |
1535 |
ng/L |
0-14 |
27-Apr-202123:33 |
|
Troponin-T (TNT) |
850 |
ng/L |
0-14 |
29-Apr-202120:23 |
|
Troponin- T (TNT) |
1014 |
ng/L |
0-14 |
29-Apr-202111:59 |
|
Troponin-T (TNT) |
239 |
ng/L |
0-14 |
01-May-202117:14 |
|
Troponin- T (TNT) |
150 |
ng/L |
0-14 |
02-May-202108:25 |
|
Troponin-T (TNT) |
39 |
ng/L |
0-14 |
03-May-202110:08 |
|
Troponin- T (TNT) |
19 |
ng/L |
0-14 |
05-May-202109:40 |
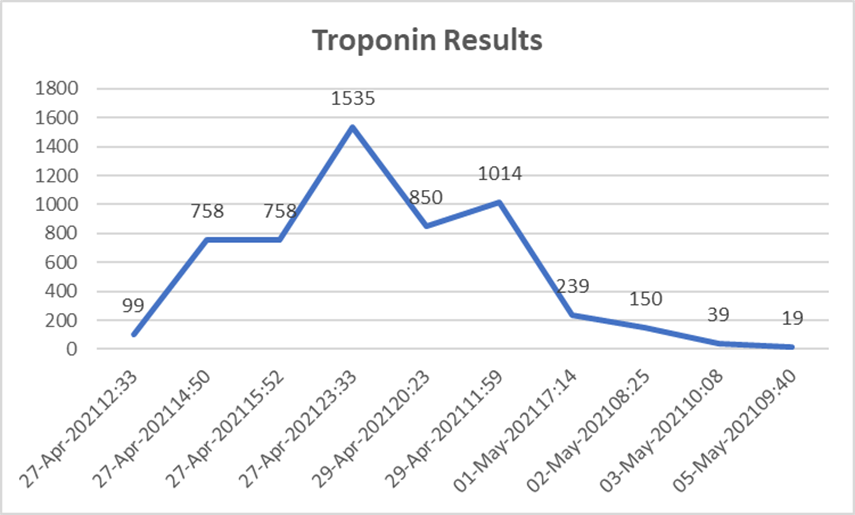
FIGURE-1
|
Virology + Other Investigations |
Result |
|
SARS-CoV-2 RNA |
Not deteceted |
|
Parvovirus B19 DNA |
Not detected |
|
EBV PCR |
Positive at the limit of sensitivity of the test |
|
CMV DNA |
Not Detected |
|
Influenze A Virus |
Not Detected |
|
Influenza B Virus |
Not Detected |
|
Respiratory Syncytial Virus |
Not Detected |
|
HIV 1+2 Antibody |
Not Detected |
|
P24 Antigen |
Not Detected |
|
Blood Culture |
No Growth |
|
Chest X-Ray |
No Acute Pulmonary features |
|
Blood Film |
Neutrophils show toxic granulation. Monocytes activated. |
|
Test |
Result |
UoM |
Ref. Range |
|
White Blood Cells (WBC) |
35.6 |
x10^9/L |
4.0 -11.0 |
|
Red Blood Cells (RBC) |
5.65 |
x10^12/L |
4.50 - 6.00 |
|
Haemoglobin (HB) |
163 |
g/L |
130 -180 |
|
Haematocrit (HCT) |
0.495 |
Ratio |
0.400 - 0.520 |
|
Mean Cell Volume |
88 |
fl |
80 - 98 |
|
Mean Cell Haemoglobin |
28.8 |
pg |
27.0 - 33.0 |
|
Mean Cell Haemoglobin |
329 |
g/L |
320 - 365 |
|
Platelets (PLT) |
375 |
x10^9/L |
150 - 400 |
|
Film (FM) |
Film Prepared |
||
|
Neutrophils (NEUT) |
30.97 |
x10^9/L |
1.80 -7.50 |
|
Lymphocytes (LYMPH) |
2.85 |
xlO^9/L |
.1.00 - 4.00 |
|
Monocytes (MONO) |
1.78 |
x10^9/L |
. 0.20 -1.00 |
|
ESR |
10 |
Mm/1st Hr |
0-5 |
|
Alanine Transaminase |
18 |
Iu/L |
Jan-50 |
|
Alkaline Phosphatase |
160 |
U/L |
30 -130 |
|
Total Protein (TP) |
77 |
g/L |
60 - 80 |
|
Albumin (ALB) |
44 |
g/L |
34 - 48 |
|
Bilirubin (TBIL) |
8 |
umol/L |
0-21 |
|
CRP |
38 |
mg/L |
0-5 |
|
Ttg Iga Antibody |
<0.5 |
kU/L |
0-14.9 |
|
Ss-A Antibody |
<0.2 |
AI |
0-0.9 |
|
Ss-AS2 Antibody |
<0.2 |
AI |
0-0.9 |
|
Ss-A60 Antibody |
<0.2 |
AI |
0-0.9 |
|
55-8 Antibody |
<0.2 |
AI |
0-0.9 |
|
Rnp 68 |
<0.2 |
AI |
0-0.9 |
|
Anti Sm |
<0.2 |
AI |
0-0.9 |
|
Smrnp Antibody |
<0.2 |
AI |
0-0.9 ' |
|
Ribosomal P |
0.2 |
AI |
0-0.9 |
|
Chromatin |
0.2 |
AI |
0-0.9 |
|
Jo~1 |
0.2 |
AI |
0-0.9 |
|
ScI-70 |
0.2 |
AI |
0-1.6 |
|
Antinuclear Ab |
Negative |
||
|
Centromere |
<0.2 |
AI |
0-0.9 |
|
Igg Ds-Dna Ab |
<1.0 |
IU/ML |
0-9.9 |
SERIAL ECGs
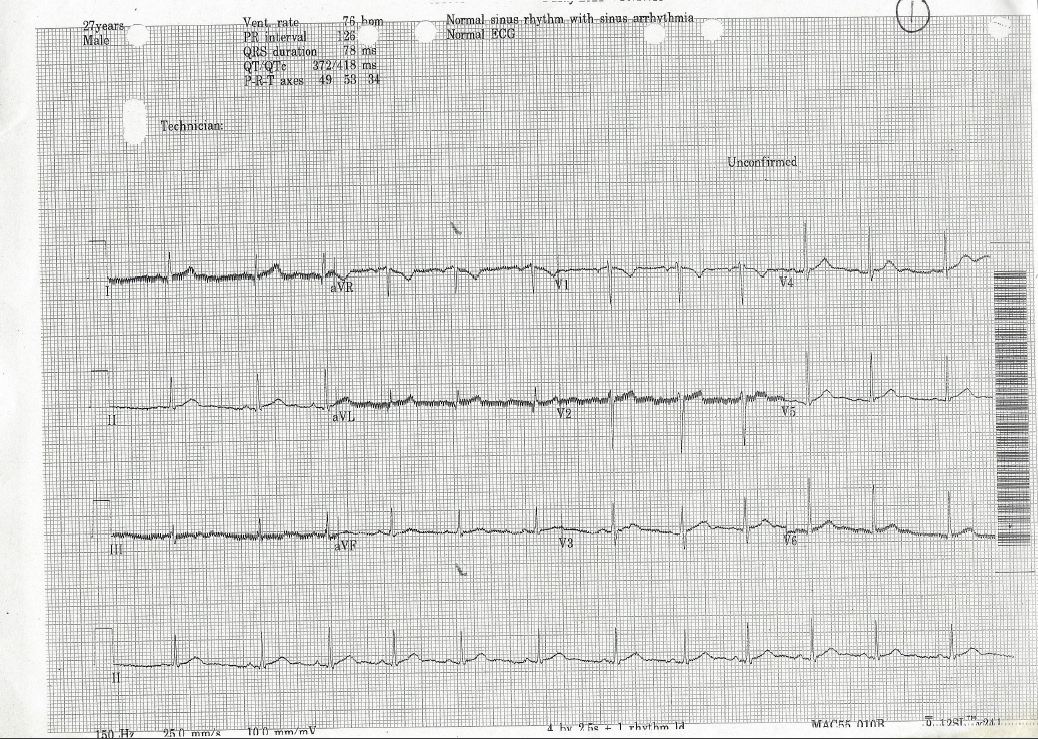
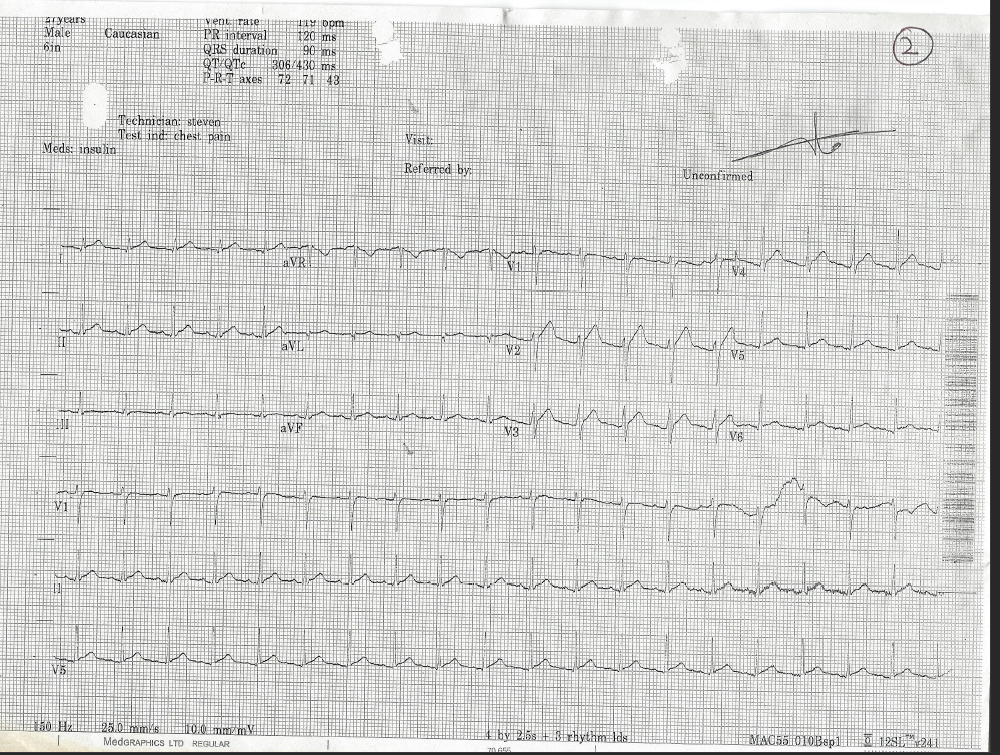
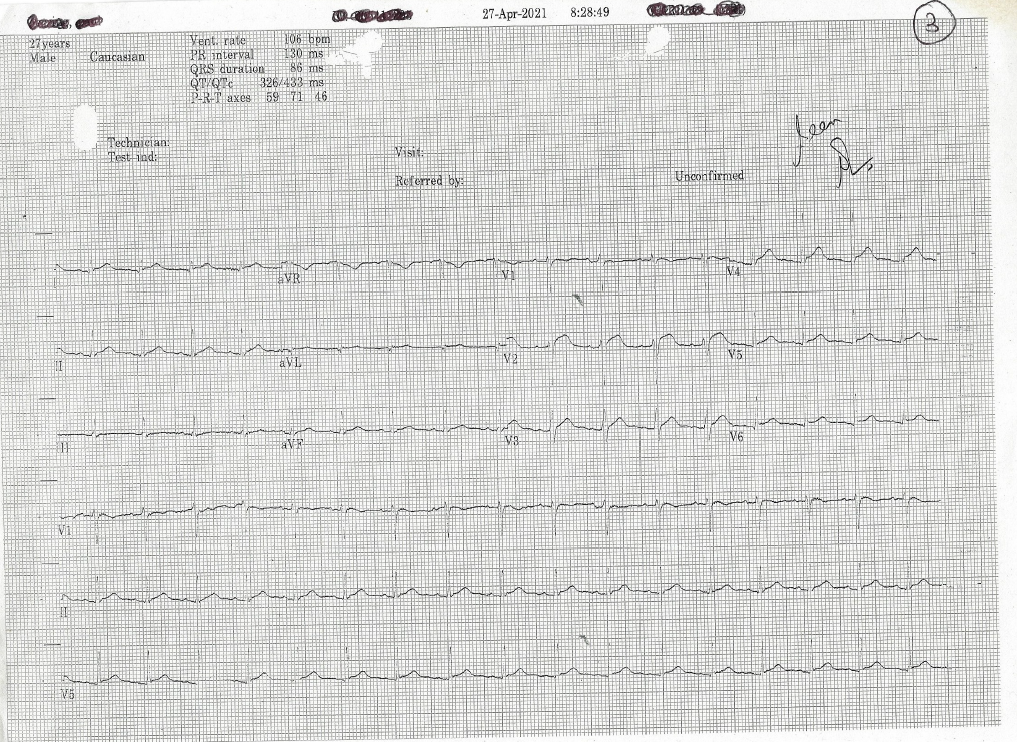
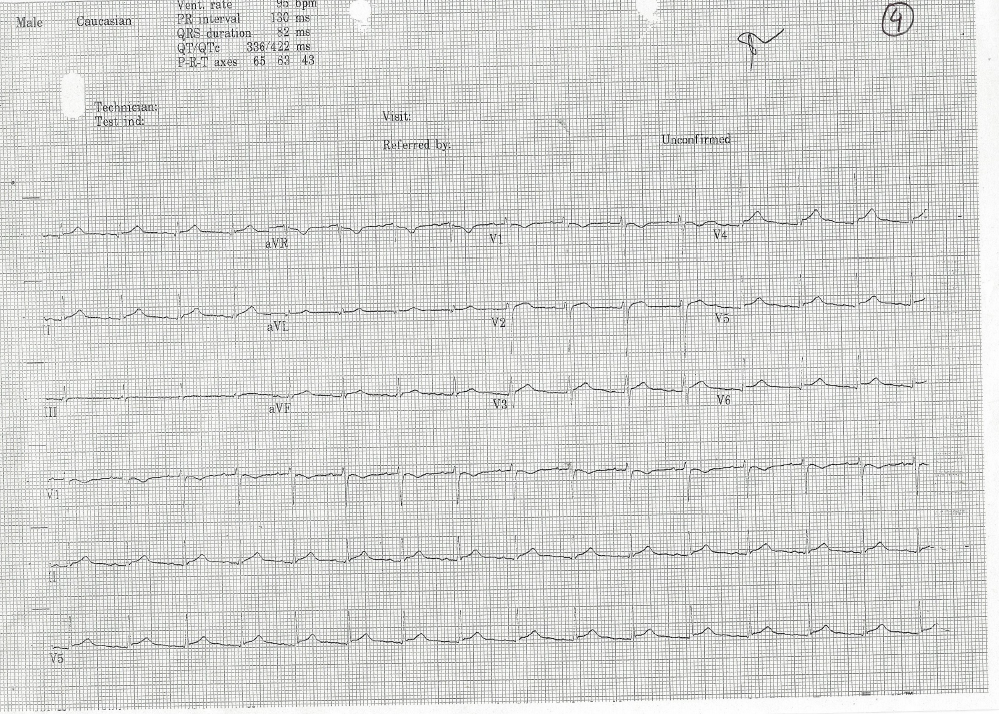
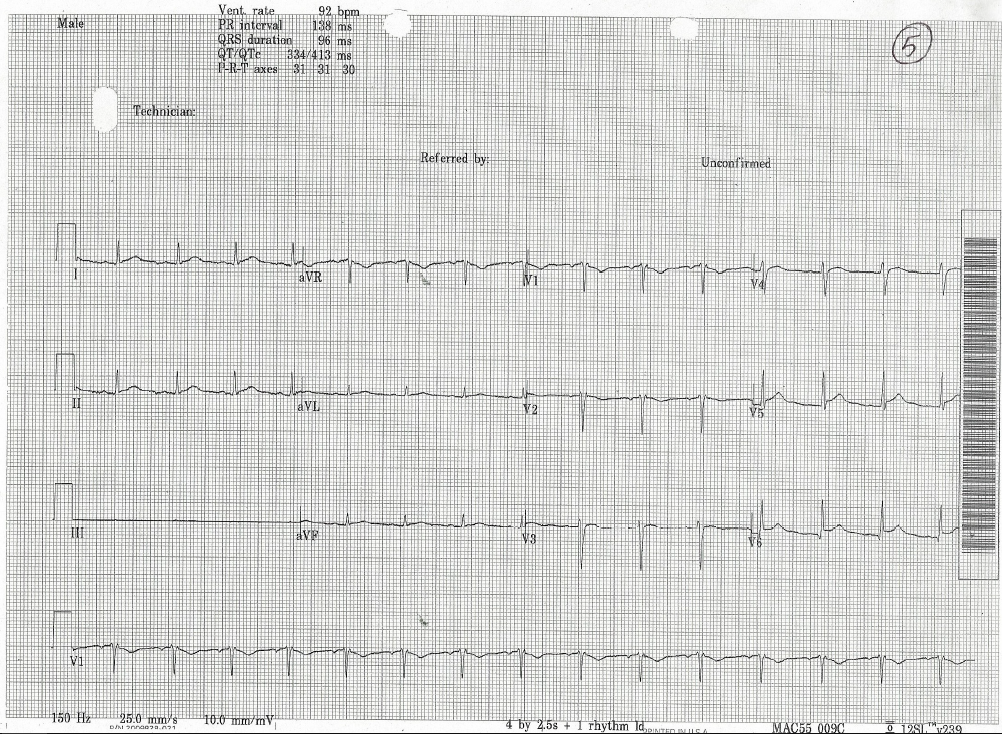
FIGURE-2
CARDIAC MAGNETIC RESONANCE REPORT
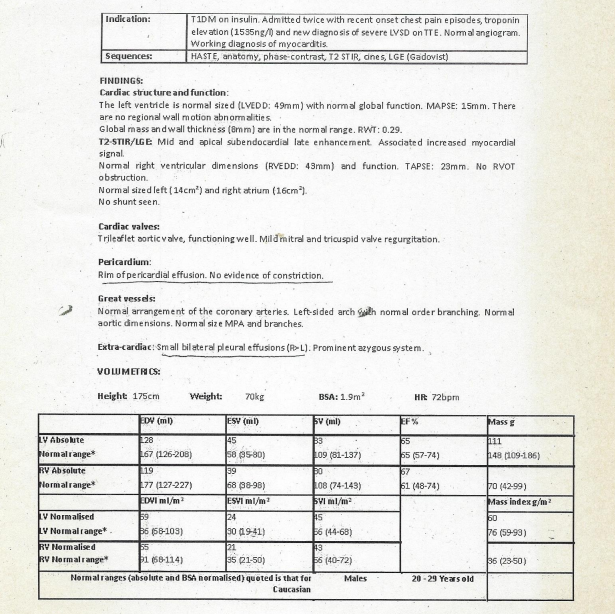
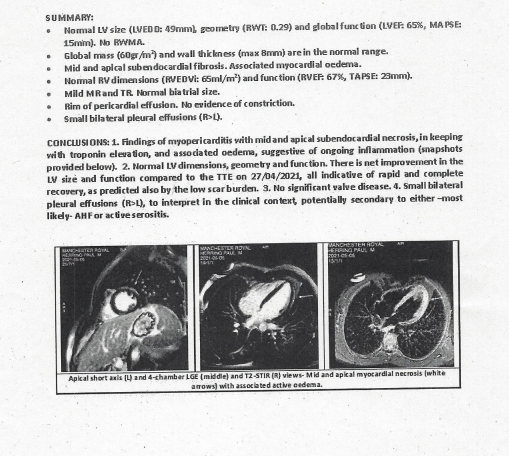
FIGURE-3
DISCUSSION
Myopericarditis is an inflammatory condition of the heart muscle and pericardium caused by various bacteria and viruses such as coxsackie viruses, adenovirus, and parvovirus B19 are the common causes, other viruses also cause myocarditis, such as parainfluenza and COVID-19 [3]. The exact aetiology is unknown. Multiple mechanisms are proposed. The pathogenesis of viral myocarditis is associated with direct damage to the myocardium and immune-mediated cardiac muscle damage after a viral infection, and the cytokine response is essential to cause immune-mediated myocyte damage [3]. Myocarditis in adults with DKA is rarely reported however there are a few cases of myocarditis with DKA reported in children [4]. The aetiology proposed in children was that acidosis might affect the contractility of the cardiac muscle at the cellular level [4].
The usual ECG findings of acute myocarditis are inverted, flat, or biphasic T waves and S-T elevation, but it doesn’t involve the QRS [2].
The ECG changes in our patient couldn’t be explained by the electrolyte abnormalities as all the electrolytes including the phosphate were normal. Low phosphate should be considered as cause of unexplained ECG changes in patients with DKA as hypophosphatemia may play a role in the insufficient cardiac output but does not explain the ST segment elevation or the cardiac MRI findings in our patient [5].
Another rare condition which presents with rapid onset of diabetes as DKA with myocarditis is fulminant type 1 DM. Fulminant type 1 diabetes is relatively new subtype of diabetes which presented with a rapid onset of symptoms, due to complete destruction of pancreatic beta cells, absent auto antibodies, and increased level of pancreatic enzymes in the serum. The exact mechanism of the beta cell destruction isn’t known but an underlying viral infection was proposed to be the likely cause as evidence by mononuclear cell infiltrations, detected in endocrine and exocrine pancreas [6]. The diagnosis of fulminant type 1 DM is made by absent autoantibodies, low HBA1C, low C peptide and urinary C peptide levels. Patients presenting with fulminant type 1 DM have a high mortality [7] therefore that should be considered a differential diagnosis in a patient presenting with new onset DKA and non-specific ECG changes which could point to the myocarditis. Our patient however didn’t fulfil the criteria for fulminant type 1 DM and weakly positive EBV serology didn’t explain the myocarditis.
The incidence of Myocarditis is 12% in adults [8], but no cases of DKA and myocarditis have been reported in literature in adults so far. There have been case reports of DKA with myocarditis in children [9].
The complications of Myocarditis can lead to dilated cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and heart failure [8] therefore it is very important to make early diagnosis and manage accordingly.
CONCLUSION
We report a case of myocarditis in a patient with diabetic ketoacidosis. It is important to consider other aetiologies in any patient who presented with DKA and found to have unexplained an ECG change that is fulminant type 1 DM or electrolyte abnormalities which were ruled out in our case. Cardiac MRI remains an important non-invasive tool to diagnose myocarditis.
REFERENCES
- Mokuno T, Sawai Y, Oda N, Mano T, Hayakawa N, Kato R, et al. (1996). A case of myocarditis associated with IDDM. Diabetes Care. 19(4):374-378.
- Gibbs P. (1974). Three cases of acute ketotic diabetes mellitus with myocarditis: a common viral origin? Br Med J. 3(5934):781-783.
- Ohara N, Kaneko M, Kuwano H, Ebe K, Fujita T, Nagai T, et al. (2015). Fulminant Type 1 Diabetes Mellitus and Fulminant Viral Myocarditis. International heart journal. 56(2):239-244.
- Halloum A, Al Neyadi S. (2019). Myocardial dysfunction associated with diabetic ketoacidosis in a 5-year-old girl. SAGE Open Med Case Rep. 7:2050313X19847797.
- Hiramatsu S, Komori K, Mori E, Ogo A, Maruyama S, Kato S. (2011). A case of fulminant type 1 diabetes mellitus accompanied by myocarditis. Endocr J. 58(7):553-557.
- Makino K, Nishimae I, Suzuki N, Nitta S, Saitoh H, Kasao M, et al. (2013). Myocarditis with fulminant type 1 diabetes mellitus diagnosed by cardiovascular magnetic resonance imaging: a case report. BMC Res Notes. 6:347.
- Kinoshita T, Kaneto H, Kawasaki F, Anno T, Kurihara T, Yamada H, et al. (2018). Fulminant Type 1 Diabetes Mellitus Complicated with a Life-threatening Electrolyte Abnormality and Abnormal Electrocardiogram Findings. Intern Med. 57(18):2685-2688.
- Zhang T, Miao W, Wang S, Wei M, Su G, Li Z. (2015). Acute myocarditis mimicking ST-elevation myocardial infarction: A case report and review of the literature. Exp Ther Med. 10(2):459-464.
- Abbas Q, Arbab S, Haque AU, Humayun KN. (2018). Spectrum of complications of severe DKA in children in pediatric Intensive Care Unit. Pak J Med Sci. 34(1):106-109.