Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2024
Management of Permanent Immature Teeth with Lateral Luxation: A Case Report
Wided Glii1,*, Amira Kikly2, Ameni Chadlia Belghuith1, Neila Zokkar3, Nabiha Douki3
1Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
2Associate professor, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
3Professor,Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
*Corresponding Author: Wided Glii, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia, Tel: (+216) 93546683, E-mail: [email protected].
Received Date: January 29, 2024
Published Date: February 20, 2024
Citation: Glii W, et al. (2024). Management of Permanent Immature Teeth with Lateral Luxation: A Case Report. Mathews J Dentistry. 8(1):43.
Copyrights: Glii W, et al. © (2024).
ABSTRACT
Introduction: Lateral dislocation is a common type of traumatic dental injury. There may be an associated fracture of the bone table. This injury is common among children and can result in pulp canal obliteration or pulp necrosis. Treatment generally consists of repositioning the tooth and applying retention. Case report: The first clinical case involved a patient who consulted us following an oral trauma. The clinical examination revealed a lateral dislocation of 1 mm of the 11 and 21. A reduction and a contention were done the day of the consultation; the removal of the contention was done 15 days later with regular follow-up. The second clinical case involved a patient who consulted us following an oral trauma. The clinical examination revealed a lateral dislocation of 6 mm for 11 and 12 with an associated alveolar fracture. A reduction and support were performed on the day of the consultation. The support was removed one month later. Follow-up examinations were carried out at 3, 6 and 9 months, and endodontic treatment was performed on 11 and 12 following the onset of root canal obliteration. Results: Various factors can affect the outcome of lateral dislocation. The aim of this article was to highlight the different factors that affect the outcome of treatment of immature teeth and the prognosis. Conclusion: When an anterior tooth suffers a lateral luxation, it's considered a significant dental injury demanding careful evaluation before any treatment begins. To ensure the best possible outcome, a number of factors that can influence treatment decisions need to be carefully assessed.
Keywords: Traumatic Dental Injury, Lateral Luxation, Permanent Immature Teeth.
INTRODUCTION
The prevalence of dislocation injuries is high in young children due to the resilient nature of the alveolar bone and supporting structures. Lateral luxation is characterized by the buccal-lingual displacement of the tooth [1,2]. This traumatic dental injury can affect hard tissue, pulp, periodontium, alveolar bone or gingiva [3]. The time that has elapsed between injury and therapy is of importance, as it will influence the therapeutic approach and prognosis. After dental trauma, x-rays provide information on the stage of development of the root, the size of the pulp space and the root canal (in relation to neighbouring teeth). In addition, the initial radiographs serve as a reference for follow-up appointments. Accurate diagnosis is necessary to determine the extent of damage and plan appropriate treatment [3].
These lesions are at risk of developing complications such as pulpal canal obliteration and pulpal necrosis. Pulpal canal obliteration is described as a progressive narrowing of the pulp space due to accelerated deposition of hard tissue along the walls of the root canal and occurs in teeth following dislocation injuries. What's more, these complications can occur years after treatment, underlining the importance of long-term patient follow-up [3,4]. The aim of this article is to highlight, through two clinical cases, factors that affect treatment planning decisions and prognosis to traumatized immature teeth.
CASE REPORT
First Case report
A healthy 7-years old patient referred to our department of dentistry, “Sahloul Hospital Tunisia” after two days of oral trauma. Exobuccal examination revealed no abnormalities. Endobuccal examination revealed a 1 mm vestibular dislocation of the 11 and a 1 mm palatal dislocation of the 21 (Figure 1). Examination of the occlusion showed a deviation of the interincisal middle (Figure 2).
.png)
Figure 1. Clinical view of maxillary arch.
.png)
Figure 2. Clinical view of occlusion
The table below resumes the results of the diagnostic tests carried out (Table I).
Table I. Diagnostic tests
|
|
11 |
21 |
|
Cold test(inconclusive) |
+ |
+ |
|
Luxation |
Palatine 1 mm |
Buccal 1 mm |
|
Mobility |
Degree 2 |
Degree 2 |
|
Periodontal probing depth |
5 5 5 4 4 4 |
4 4 4 6 6 6 |
.png)
Figure 3. Retro alveolar radiography.
Therapeutic attitude
This case was treated immediately. The table below summarizes clinical stages in the management of restraint (Table II).
Table 2. Clinical steps in the management of restraint
|
Steps |
|
|
1 |
Anaesthesia and manual reduction of 11 and 21 |
|
2 |
Shape of brace: must extend over at least 2 teeth on each side (53,54-63,64) |
|
3 |
3- Etching: - blue acid dots - 30 seconds (Figure 4) |
|
4 |
4- Rinsing-Drying: - water and air from the blower - or wet compress then dry compress → chalky white spots |
|
5 |
5- Adhesive: - Rub the demineralised surface with the microbrush soaked in adhesive - light-cure (5-10 sec per tooth) |
|
6 |
6- application of fluid resin |
|
7 |
7- Passive application of contention and light-curing (10 sec per block) |
|
8 |
8- Make the other dots, finishing with the luxated tooth and light-cure |
|
Tip: smooth the composite with the adhesive before curing. |
|
|
9 |
9- Prescription of soft food for 3 weeks, analgesics, antibiotics for 7 days. |
|
10 |
10-Appointment after two weeks for check-up and removal of restraint |
.png)
Figure 4. Etching: -blue acid dots-30.
.png)
Figure 5. Result after the application of restraint.
At 15 days: Removal of restraint (Figure 6) and inspection, the table below (table III) summarizes the results of the diagnostic tests on 11 and 21 after removal of the restraint.
.png)
Figure 6. Removal of contention after 15 days.
Table III. Diagnostic tests on 11 and 21 after removal of restraint
|
11 |
21 |
|
|
Cold |
+ |
+ |
|
test(inconclusive) |
||
|
Axial percussion |
- |
- |
|
Transverse |
- |
- |
|
percussion |
||
|
Mobility |
- |
- |
A healthy 11-years old patient referred to our department of dentistry, “Sahloul Hospital Tunisia” after two days of oral trauma. Endobuccal examination revealed a 6 mm vestibular dislocation of the 11 and 12 associated with alveolar fracture and in bloc mobility (Figure 7).
.png)
Figure 7. Endobuccal view of the patient during the 1st consultation.
The table below resumes the results of the diagnostic tests carried out (Table IV).
Table 4. Diagnostic tests
|
11 |
21 |
|
|
Cold |
+ |
+ |
|
test(inconclusive) |
||
|
Axial percussion |
- |
- |
|
Transverse |
- |
- |
|
percussion |
||
|
Mobility |
- |
- |
Radiological examination showed that 11 and 21 are immature permanent teeth in Nolla stage 9 (Figure 8a & 8b).
.png)
Figure 8 (a&b). Retro-alveolar radiology.
Therapeutic attitude
This case was treated immediately. The table below summarizes clinical stages in the management of restraint (Table V).
Table 5. Clinical steps in the management of restraint
|
Steps |
|
|
1 |
Anaesthesia and manual reduction of 11 and 12 |
|
2 |
Shape of brace: must extend over at least 2 teeth on each side (53,54-21,22, 63,64) |
|
3 |
Etching: - blue acid dots - 30 seconds(Figure 9) |
|
4 |
Rinsing-Drying: - water and air from the blower - or wet compress then dry compress à chalky white spots |
|
5 |
Adhesive: - Rub the demineralised surface with the microbrush soaked in adhesive - light-cure (5-10 sec per tooth) |
|
6 |
Application of fluid resin |
|
7 |
Passive application of contention and light-curing (10 sec per block) |
|
8 |
Make the other dots, finishing with the luxated tooth and light-cure Tip: smooth the composite with the adhesive before curing. |
|
9 |
Prescription of soft food for 3 weeks, analgesics, antibiotics for 7 days. |
|
10 |
Appointment after one month for check-up and removal of restraint |

Figure 9. Etching: blue acid dots-30.
.png)
Figure 10. Result after the application
At one month: Removal of restraint (Figure 11) and inspection, the table below (table VI) resumes the results of the diagnostic tests on 11 and 12 after removal of the restraint and check-up at 3, 6 months:
.png)
Figure 11. Removal of contention after one month.
Table VI. Results of diagnostic tests on 11 and 12 after removal of restraint and check-up at 3, 6 months
|
11 |
21 |
|
|
Cold |
+ |
+ |
|
test(inconclusive) |
||
|
Axial percussion |
- |
- |
|
Transverse |
- |
- |
|
percussion |
||
|
Mobility |
- |
- |
Clinical control
The clinical examination shows a positive cold test for the 2 teeth. 11 and 12 are not sensitive to either axial or transverse percussion, and there is an absence of mobility with normal crown shade (Figure 12) (absence of dyschromia).
.png)
Figure 12. Check-up at 9 months
X-ray control
The radiological examination showed apical closure of the central and lateral incisors, a reduction in pulp volume due to accelerated apposition of secondary dentine (Figure 3), and a risk of obliteration of the pulp canal, so preventive endodontic treatment was given (Figure 14).
.png)
Figure 13. Radiological check at 9 months.
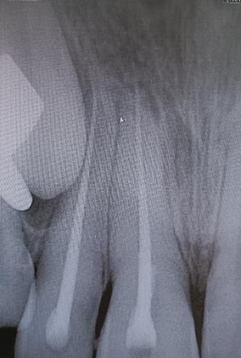
Figure 14. Endodontic treatment of 11 and 12.
DISCUSSION
Lateral luxation is a serious dental trauma that involves the periodontal complex and alveolar bone. However, a multidisciplinary approach and a correct management of the cases, as reported hereby, lead to a successful resolution [5].
Reposition and Stabilization
According to the latest IADT recommendations published in 2020; Reposition the tooth digitally by disengaging it from its locked position and gently reposition it into its original location under local anesthesia. From the pulp's point of view, repositioning displaced teeth is an additional traumatic event; minimising the additional trauma is another important aspect of the treatment, so manual repositioning may seem preferable [7].
The time elapsed between the trauma and the correct diagnosis of lateral dislocation may determine the prognosis for treatment. Late repositioning (>48 hours) is difficult if a clot forms at the end of the tooth socket [5]. In both clinical cases, treatment was initiated within 48 hours.
- Method: Palpate the gingiva to feel the apex of the tooth. Use one finger to push downwards over the apical end of the tooth, then use another finger or thumb to push the tooth back into its socket.
As a general rule, all teeth that have been repositioned require splinting, as do all teeth that are mobile. There are numerous splinting techniques described in the literature. What matters most is that the splints are flexible to allow the physiological movement of teeth, and they should be easy to remove [6].
Times are determined by the severity of accompanying bone injuries. Where teeth are displaced without bone fractures, splinting times are kept to a minimum (1–2 weeks). Where alveolar bone fractures occur, splinting times are of the order of 3– 5 weeks [6].
Follow-up
Follow ups are mandatory after traumatic injuries. Clinical and radiographic assessments are necessary: after 2 weeks, 4 weeks, 8 weeks - after 3 months, 6 months, after 1 year - then every year for at least 5 years. Patients (and parents) should be informed that they should be alert to any unfavourable evolution and that they should return to the clinic if one is observed [7]. Each follow up should include questioning of the patient about any signs or symptoms, plus clinical and radiographic examinations and pulp sensibility testing. Photographic documentation is strongly recommended. Therefore, patients need to understand the importance of maintaining regular follow up appointments [1].
In immature permanent teeth, this is of utmost importance in order to allow continued root development and apex formation and every effort should be made to preserve the pulp.
Factors influencing treatment plan decisions
Many interrelated factors influence pulp survival after trauma and determine when endodontic treatment should be initiated. These include: Type of injury, The severity of injury, The age of patient: For young patients with immature teeth, the pulp has considerable healing capacity after a dislocation injury [7,9]; The size and maturity of the apex: Knowledge of the developmental stages of permanent teeth is essential in trauma assessment since it influences diagnosis, treatment planning and outcomes. A classification proposed by Nolla has been widely used and is particularly useful when considering the treatment of traumatized teeth [6]. The width of the apical foramen plays an important role in traumatic tooth dislocation.
The smaller it is, the more likely the pulp is disrupted and the less likely it is repaired by revascularization [8]. A diameter of less than 1 mm has been described as critical but does not necessarily exclude revascularization. Even for laterally luxated teeth, an apical diameter ranging between 0.1 and 1 mm can still lead to pulp survival in 39% and 22% [3]. The two cases are in Nolla stages 7 and 9 respectively, where the apices are wide open (apical diameter > 1 mm). As a general rule, root canal treatment should not be initiated until there is confirmed evidence of pulp necrosis and infection in the root canal. A lack of response to pulp sensibility testing, particularly during the first few months, is not the sole indication to initiate root canal treatment [3,6].
Complications and managements
Early detection and management of complications improves prognosis [7]. The main post-traumatic complications are as follows: pulp space obliteration (70%), pulp necrosis and infection (11%), several types of root resorption, breakdown of marginal gingiva and bone. In the case of lateral dislocation, pulp canal obliteration was the most frequent complication of immature teeth [1,11], which is the situation in the 2nd clinical case: a clinical and radiological check-up was completed at 3, 6 and 9 months, and at 9 months the radiological examination showed apical closure and apposition of secondary dentine, leading to narrowing of the canal space, with a risk of total canal obliteration. Successful preventive endodontic treatment was accomplished.
In the event of a necrotic pulp diagnosed during follow-up appointments, several treatment options are available for the management of immature permanent teeth, of which, the formation of dentine stops, resulting in a tooth with thin dentine walls that are prone to fracture. Calcium silicate hydraulic cements (CSHCs) such as MTA have been widely used as an apical barrier material for immature teeth with non-vital pulp [3]. Regeneration is an alternative to the apical barrier technique using an MTA plug. Based on the observation that tissue growth and "regeneration" can occur in teeth with an open apex [1]. Regeneration of immature permanent teeth can be achieved using: platelet-rich plasma (PRP) and platelet-rich fibrin (PRF), blood clot revascularisation (BCR) [10]. As more and more reports and case series were published, it was hoped that genuine pulp regeneration could be achieved with these protocols. Regeneration has advantages for the patient: the procedure is less invasive and more biological, as healing can occur, and the root canal can be filled with biological, immunocompetent tissue rather than synthetic material. In addition to the biological benefits, the apposition of hard tissue and the promotion of root growth can lead to considerable mechanical advantages for regenerated teeth. The indication for regeneration includes teeth with incomplete root formation after pulpal necrosis, with or without existing periapical lesions.
CONCLUSION
Lateral luxation of anterior teeth is one of the most severe types of dental injuries. Accurate assessment of the traumatic injury before any treatment is essential. Numerous factors influencing treatment planning decisions must be understood thoroughly so that appropriate treatment decisions can be made. The most frequent complication reported for immature teeth with lateral luxation was pulp space obliteration. Careful follow-up is required to treat complications as early as possible.
REFERENCES
- Clark D, Levin L. (2018). Prognosis and complications of immature teeth following lateral luxation: A systematic review. Dent Traumatol. 34(4):215-220.
- Soares PB, Vilela AB, Moura CC, Estrela C, Bueno MR, Soares CJ. (2020). Lateral luxation of incisor-a case report of using a new cone-beam computed tomography software and reposition guideline. Braz Dent J. 13(31):337-343.
- Krastl G, Weiger R, Filippi A, Van Waes H, Ebeleseder K, Ree M, et al. (2021). Endodontic management of traumatized permanent teeth: a comprehensive review. Int Endod J. 54(8):1221-1245.
- Clark D, Levin L. (2019). Prognosis and complications of mature teeth after lateral luxation: a systematic review. J Am Dent Assoc. 150(8):649-655.
- Soares PB, Vilela AB, Moura CC, Estrela C, Bueno MR, Soares CJ. (2020). Lateral luxation of incisor-a case report of using a new cone-beam computed tomography software and reposition guideline. Braz Dent J. 13(31):337-343.
- Moule A, Cohenca N. (2016). Emergency assessment and treatment planning for traumatic dental injuries. Aust Dent J. 61(1):21-38.
- Bourguignon C, Cohenca N, Lauridsen E, Flores MT, O'Connell AC, Day PF, et al. (2020). International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 36(4):314-3 30.
- Andreasen FM, Kahler B. (2015). Pulpal response after acute dental injury in the permanent dentition: clinical implications—a review. J Endod. 41(3):299-308.
- Levin L, Day PF, Hicks L, O'Connell A, Fouad AF, Bourguignon C, Abbott PV. (2020). International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: General introduction. Dent Traumatol. 36(4):309-313.
- Murray PE. (2018). Platelet-rich plasma and platelet-rich fibrin can induce apical closure more frequently than blood-clot revascularization for the regeneration of immature permanent teeth: a meta-analysis of clinical efficacy. Front Bioeng Biotechnol. 11(6):139.
- Bastos JV, Côrtes MI. (2018). Pulp canal obliteration after traumatic injuries in permanent teeth–scientific fact or fiction? Braz Oral Res. 32(suppl 1):e75.