Information Links
Related Conferences
Previous Issues Volume 7, Issue 3 - 2023
In Vitro Analysis of Surface Treatment, Titanium and Zirconia Used in Prosthetic Dentistry, on Osteoblast Cultures
Renato Carlos Burger1,*, Elizabeth Ferreira Martinez2, Flavia Lucisano Botelho do Amaral1
1Department of Restorative Dentistry, Faculty of Dentistry, São Leopoldo Mandic University, Campinas, São Paulo, Brazil
2Department of Microbiology, Faculty of Dentistry, São Leopoldo Mandic, Campinas, São Paulo, Brazil
*Corresponding Author: Renato Carlos Burger, Rua Otavio Tarquinio de Souza, 624 – Campo Belo – São Paulo – SP – Brazil – CEP 04613-002; Email: [email protected]
Received Date: October 13, 2023
Publication Date: December 04, 2023
Citation: Burger RC, et al. (2023). In Vitro Analysis of Surface Treatment, Titanium and Zirconia Used in Prosthetic Dentistry, on Osteoblast Cultures. Mathews J Dentistry. 7(3):41.
Copyright: Burger RC, et al. © (2023)
ABSTRACT
This In Vitro study aimed to evaluate the effect of surface treatment on osteoblastic cells in terms of proliferation, viability and osteopontin expression. The Trypan blue, MTT vitality tests and enzyme-linked immunosorbent assay (ELISA) were used to assess the response of cell cultures to titanium surfaces and zirconia ceramics used in dental prosthodontics. The ultrastructural topographic features and cellular morphology on the different surfaces were assessed using scanning electron microscopy at 500X magnification (72 hours). The aforementioned surfaces were treated with aluminum oxide sandblasting (AO), silica-modified aluminum oxide (SMAO) and a control group based on non-sandblasted surfaces (MA). Quantitative data were tabulated and analyzed using ANOVA and Tukey tests at a significance level of 5%. The results showed that osteoblast proliferation was higher and significantly different on zirconia compared to titanium surfaces at 72 h, with no significant differences between surface treatments. Cell viability was significantly higher on OA-treated zirconia surface. Quantification of osteopontin was similar across all surfaces except for OA-treated surfaces, where a significantly lower concentration of osteopontin was observed. Photomicrographs showed increased roughness between treatments accompanied by different morphological features of the cells, according to surface type and surface treatment. In conclusion, all surfaces and treatments promoted cell proliferation and maintained cell viability in the time periods evaluated.
Keywords: Biomaterial, Osteoblasts, Surface treatment
INTRODUCTION
Titanium remains the material of choice for dental implants (Zarb, 1983) [1], though ceramics have emerged as a potencial contender to replace it, especially regarding the prosthetic components associated to it (Azevedo et al., 2008; Andreluolo et al., 2011) [2,3]. Metal-free materials are desirable as metal exert potentially deleterious effects in the oral cavity, such as metal ions and particle leakage, corrosion and allergy-related problems (Tschernitschek et al., 2005; Möller et al., 2012) [4,5].
Technological advancements in the making of new ceramics have resulted in the development of novel categories of ceramics that in many physicomechanical aspects resemble metals (Della Bona 2009) [6]. Mechanically resistant ceramics developed for the aforementioned purposed are based on a metallic element, zirconium, which are combined to oxides during the manufacturing process to produce zirconia, which in turn can be combined with yttrium oxide, for example, to produce yttria-stabilized zirconia-based ceramics with excellent properties (Andreluolo et al., 2011) [3] from a biomechanical viewpoint. This allows, for example, the manufacturing of intracanal posts, ceramic copings for dental prostheses, surgical burs and osseointegrating implants (Wenz 2008; Özkurt et al., 2010) [7,8]. Zirconia-stabilized materials used for dental implants should comply with a number of constituents according to the NBR ISO 13356 (ABNT NBR ISO 13356, 2009). When analyzing the composition of zirconia ceramics for dental prostheses, the basic components therein are not different from those used in zirconia for dental implants, including in terms of their physical and mechanical properties (Moraes, 2004) [9].
The Bone-Implant Contact (BIC) rate of zirconia implants is close to that of titanium implants (Hoffmann et al., 2006; Andreiotelli et al., 2009; Möller et al., 2012) [5,10,11]. However, to date, it is not known whether zirconia ceramics for dental prosthesis, which have a similar constitution, would share the same bone affinity as titanium implants.
When an analogy is made with adhesive dentistry, micro-retentions created in the restorative materials enhance the bond between tooth and restoration (Yamashita & Yamani, 1982; Renk & Hartmann, 1982) [12,13]. The proposed microblasting of the inner aspect of the prosthetic parts prior to cementation has shown a substantial increase in micromechanical bond, surface energy, wettability of the cement in a simple and effective way (Kühl & Renk, 1982; Swift Jr, 1989; Lin et al., 1990; Isidor et al.,1991; Mc Caughey, 1993) [14-18]. A method developed for the repair of metal-ceramic or metalloplastic restorations, the CoJet System (3M ESPE), combines sandblasting with adhesive systems for laboratory metals, particularly those forming a layer of silica on the metal surface (Latta, Barkmeier, 2000; Watanabe et al., 2008) [19,20]. This method improves adhesion on both metal and resin as well as ceramic surfaces (Frankenberger et al., 2000, Hermann et al., 2000 a, b Castro 2010, Sarmento et al., Baldissara et al., 2013, Della Bona et al., 2015) [21-26].
Following this trend to create a surface with microroughness for a better bond between two materials, when the concept of surface treatment was introduced in osseointegrated dental implants to create micro and nano surface textures, promising findings on bone neoformation were reported, which has allowed faster osseointegration with possible immediate implant loading (Matsuzaka et al., 2003; Gapski, 2003; Wieland et al., 2005) [27-29].
Considering new avenues for the use of dental restorative Zirconia in the manufacturing of osseointegrated dental implants, which can be further customized using CAD/CAM systems, and with a view to verify whether such material would stimulate cellular behavior in a similar fashion as that observed with titanium, the aim of this study was to analyze the effect of titanium and zirconia surface treatments on cell/substrate interaction.
Experimental details
For this In Vitro experiment, grade IV titanium (commercially pure – INP – São Paulo – Brazil) and zirconium ceramics for dental prosthesis (LavaTM, 3M ESPE, MN, USA) were used. A total of 117 square-shaped titanium specimens measuring 5 x 5 mm by 2 mm and 117 specimens of tetragonal yttrium-stabilized zirconia (Y-TZP) with the same dimensions were made. The Lava Frame blocks were cut into shape using a double-sided diamond disk (Dedeco, Long Eddy, New York, USA) mounted on a mandrel and a micro-motor (190 Strong 210, Saeshin Precision Co., LTd Daegu, Korea) to obtain square shapes 20% larger than the final size to allow for sintering shrinkage.
Surface treatments were assessed on three levels: MA – machined only, i.e. no surface treatment; AO – Aluminum Oxide microblasting and SMAO – Silica-modified Aluminum Oxide. One third (1/3) of the titanium specimens and 1/3 of the zirconia ceramics specimens received no surface treatment (MA). For the test specimen in Titanium (MA), the machined surface was considered “smooth” (control) for the purpose of topographic features when comparing against the treated surfaces. The zirconia test specimen that did not receive surface treatment (MA) was also considered a smooth surface. One-third (1/3) of the specimens were sandblasted on one of their surfaces using a Standart micro-sandblaster (Bio-Art Equipamentos Odontológicos LTDA – São Paulo – Brazil) and aluminum oxide powder (50 μm particles) and 60-80 lb/in2 compressed air pressure for 5-10 seconds at a right angle with the specimen surface from a distance of 5.0 cm. The pressure of the compressed air was checked using a pressure gauge (Schulz S / A, Joinville, St Catarina, Brazil). These specimens were rinsed and cleaned in distilled water, using an ultrasonic device (Digital Ultrasonic Cleaner – Kondortech – Equipamentos Odontológicos Ltda, São Carlos, SP, Brazil) for 180 seconds and then dried with jets of air jets using a three-way syringe free from moisture and grease. One-third (1/3) of the specimens were sandblasted on one surface with the same sandblaster using 30 μm particles of silicic acid-modified alumina powder (CoJet Sand – 3M ESPE, Neuss, Germany) at 60 – 80 lb/in2 compressed air pressure for 5-10 seconds, at a right angle with the surface of the specimen, maintaining an average distance of 5.0 cm. The specimens were then cleaned (removal of abrasive dust) using grease and moisture-free air jets from the triple-syringe for 10 seconds following the manufacturer’s instructions. All specimens were stored in sterilizing pouches (VedaMax® - Zermatt Indústria e Comércio Ltda – Itatiba – SP – Brazil) for steam autoclave sterilization. The steam autoclave (Vitale 12 liters Analog – Cristófoli Equipamentos de Biossegurança Ltd, Campo Mourão – PR – Brazil) was set at 126°C to 129°C, 1.7 to 1.8 kgf/cm2 for 16 minutes and a drying cycle of 30 minutes.
To verify the surface topography of the specimens after treatment, an ultrastructural analysis was performed using SEM (JEOL-JSM 7401 F, Jeol USA Inc., Peabody, MA, USA) at X500 magnification.
The cell line used was pre-osteoblasts from rat calvaria (MC3T3-E1) obtained from the American Type Culture Collection (ATCC, EVA). The cells were cultured in alpha-modified Minimum Essential Medium (α-MEM) (Nutricell®, Campinas, SP, Brazil) supplemented with 10% fetal bovine serum (Cultilab®, Campinas, SP, Brazil) and 1% antibiotic-antimycotic solution (Sigma, St. Louis, Missouri, USA) supplemented with 10 Mm beta-glycerophosphate (Sigma®) mineralizing factors and 50 μg/ml ascorbic acid (Invitrogen®). All procedures were carried out in a laminar flow hood (Bio Seg 09 – Veco do Brasil – Campinas – São Paulo – Brazil) to maintain the sterility of materials and substances used for cell culture. The cells were kept in an oven at 37ºC (Thermo Cientific – Spectrun – São Paulo – SP – Brazil) in a humid atmosphere containing 95% air and 5% carbon dioxide. The culture medium was changed every 2-3 days for a period of approximately 15 days and the progression of the cultures followed up under inverted phase microscopy (Nikon Eclipse TS 100 – Spectrun – São Paulo – Brazil) until sufficient cells were available for the experiment. The initial cell density for all experiments was 110 cells/mm2. All experiments were performed in triplicate and then repeated.
For the evaluation of cell proliferation, the vital Trypan blue exclusion method was used at 24h, 48h and 72h of culture on the surfaces of the specimens and the control surface (polystyrene). The cells were detached using trypsin and the cell pellet resulting from centrifugation (Centrifuge 5804 R – Eppendorf – Hamburg, Germany) was suspended in 1 ml of medium. 10 μl of the cell suspension was collected to which 10 μl of Trypan blue was added and 1 μl of this stained suspension was placed in a hemocytometer (Neubauer-Fisher Scientific chamber, Pittsburgh, PA, USA) and assessed under an inverted phase microscope (Nikon Eclipse TS 100 – Spectrun – São Paulo – SP – Brazil) for cell counting.
Cell cultures were tested for viability using the MTT assay. After 24h, 48h and 72h of seeding on the different surfaces, 10 μl of the MTT solution (5 mg / Ml – SIGMA, USA) diluted in serum-free DMEM culture medium were added to the treated cultures and incubated for 3 hours at 37°C. 100μl of 10% DMSO (dimethylsulfoxide) solution was added. After solubilization of the crystals, quantification was obtained from optical density measurements on a microplate reader (ELX800, Biotek Instruments, Inc., USA) at 590 nm.
The quantification of secreted osteopontin by the osteoblastic cells plated on the different surfaces was evaluated by enzyme-linked immunoassay (ELISA) at 24h, 48h and 72h. The supernatant from each specimen was collected and centrifuged at 5000g for 15 minutes at 4°C. Aliquots from each sample were evaluated by ELISA to determine PGE-2 levels according to the manufacturer’s recommendations (Ebioscence, San Diego, CA, USA). After that, 100 μl of the detection antibody was added to all wells, except in the control well and incubated overnight (18h) at 4°C. The plates were washed with buffer solution, for further addition of the standard antibody and samples. After the incubation time, the plates were washed again and incubated with 200 μl of the conjugated antibody for 30 min at room temperature and protected from the dark. The reaction was quenched by adding 50 μl of sulfuric acid solution and the color was measured in a spectrophotometer (Epoch, Biotek, Winooski, VT, USA) at 570 nm. The total amount of osteopontin was determined as treatment (pg/ml). The results were calculated using the standard curve created for each assay.
SEM images (JEOL – JSM 7401 F, Jeol USA Inc., Peabody, MA, USA) were made to assess osteoblast morphology (X500). Cells were cultured, according to the aforementioned cell culture procedures. The analysis took place at 72 hours of culture. Cells were fixed in 4% formaldehyde and 0.1% glutaraldehyde solution in 0.05% sodium cacodylate buffer for subsequent dehydration to critical point using HMDS (hexamethyldisilazane). The specimens were then sputter-coated with 20 nm of gold and mounted on metal platforms for SEM analysis.
The data regarding cell proliferation and viability were analyzed using two-way ANOVA and the Tukey test post hoc at a significance level of 5%. All calculations were performed on SPSS 23 (SPSS Inc., Chicago, IL, USA).
RESULTS AND DISCUSSION
Surface Features
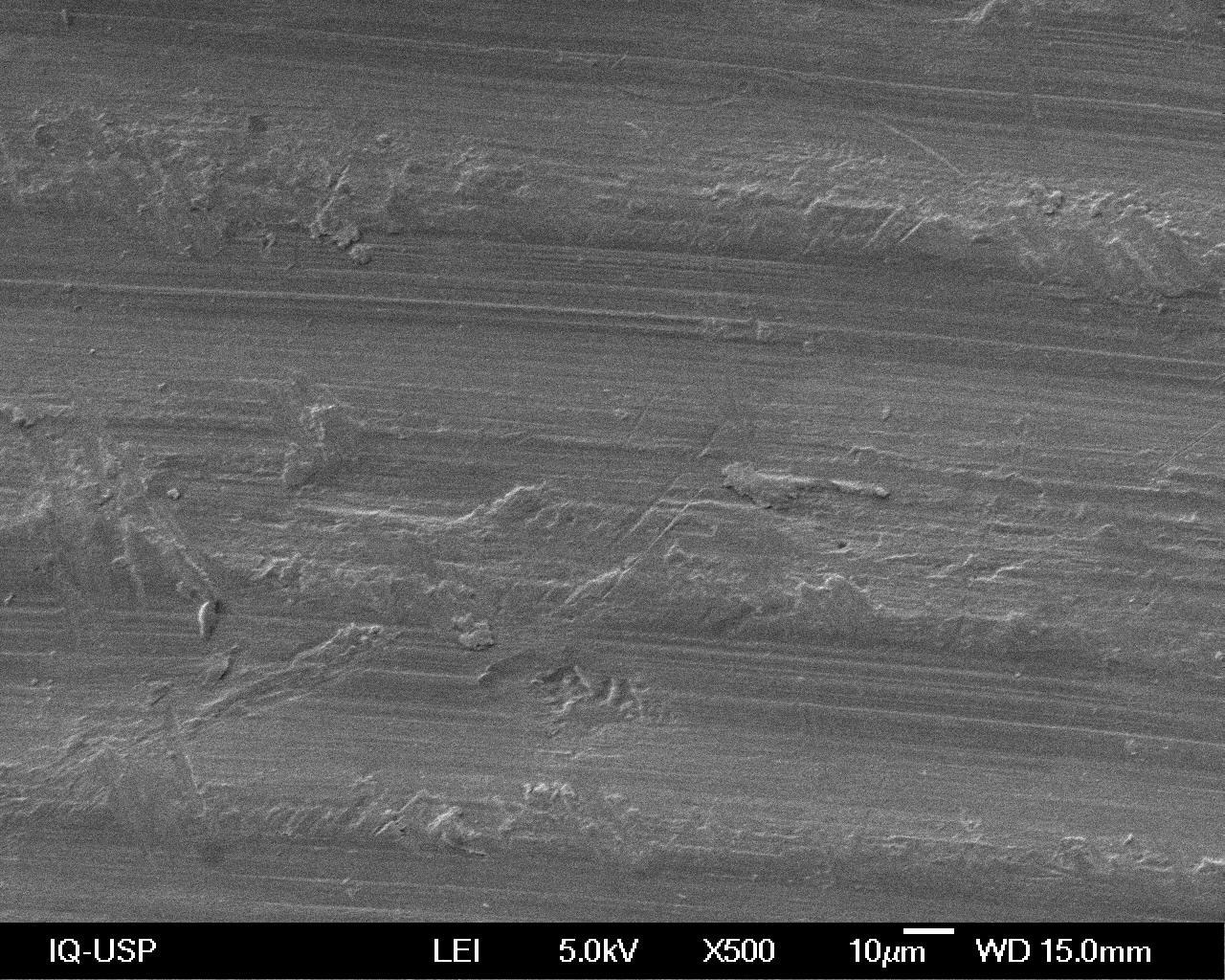
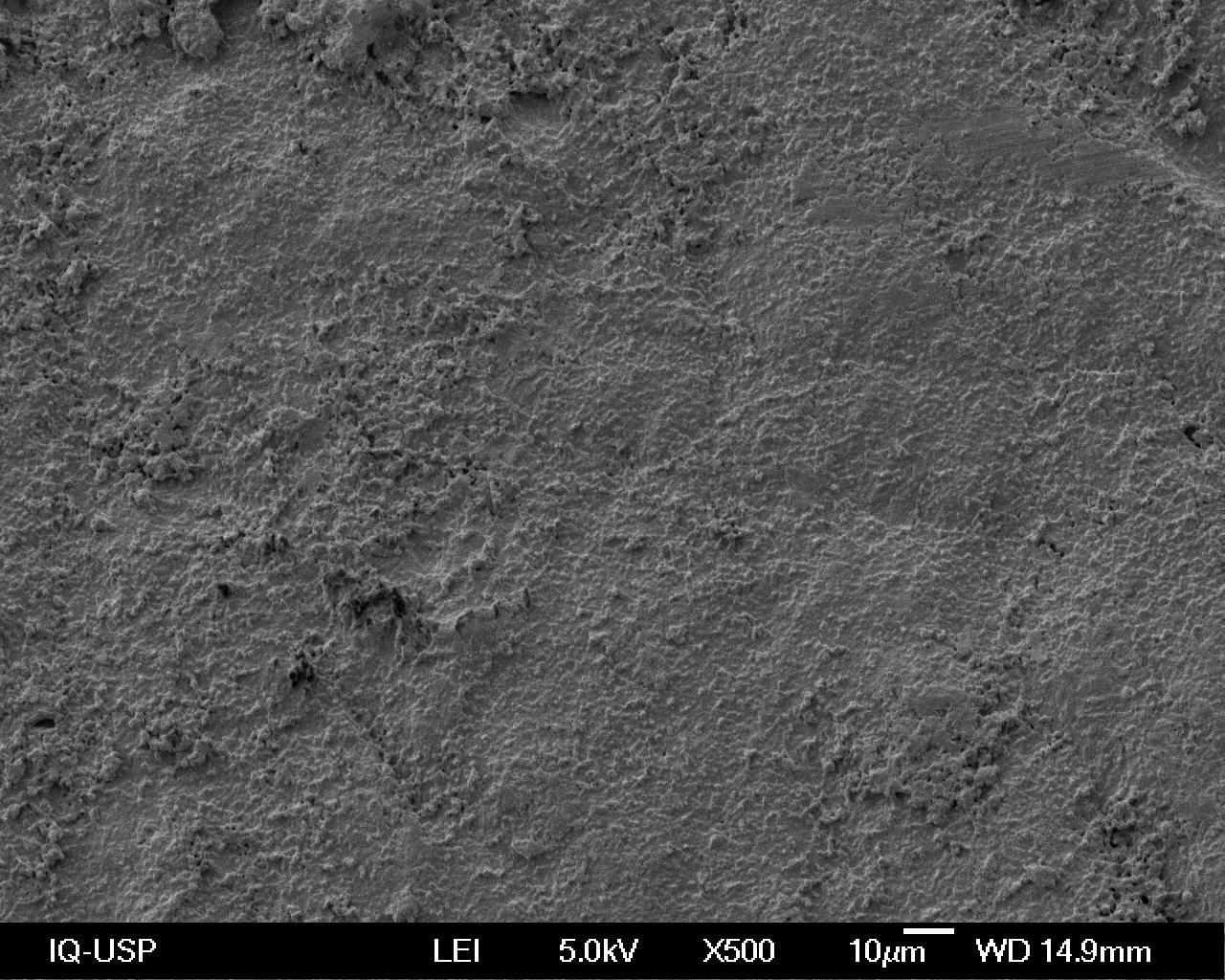
Figure 1 shows the surfaces of Titanium and Zirconia (Y-TZP) considered smooth due to the machining and treatment processes of the MA group. 1A shows a smooth appearance with scratches left by the machining process, while in 1B the appearance is irregular due to manual treatment with abrasive sandpaper.
A B
Figure 1: The smooth surface of the Titanium specimens is illustrated in A, and the smooth surface of the Zirconia (Y-TZP) in B, due to machining and treatment respectively (MA).
When the so-called smooth zirconia surface (Y-TZP) was evaluated (Figure 1B), a difference in roughness pattern was observed when compared to the smooth surface of the titanium (Figure 1A), suggesting a lesser a degree of smoothness on the zirconia (Kohal et al. al., 2009) [30]. The grooves did not conform to a parallel pattern such as in the machined titanium, probably because they were obtained from different methods. On the zirconia, surface treatment was performed manually with circular and decreasing grain of abrasiveness, resulting in a different final appearance of the smooth titanium surface, which was planned using the manufacturers own mechanical polishing method (Yamashita et al., 2009) [31].
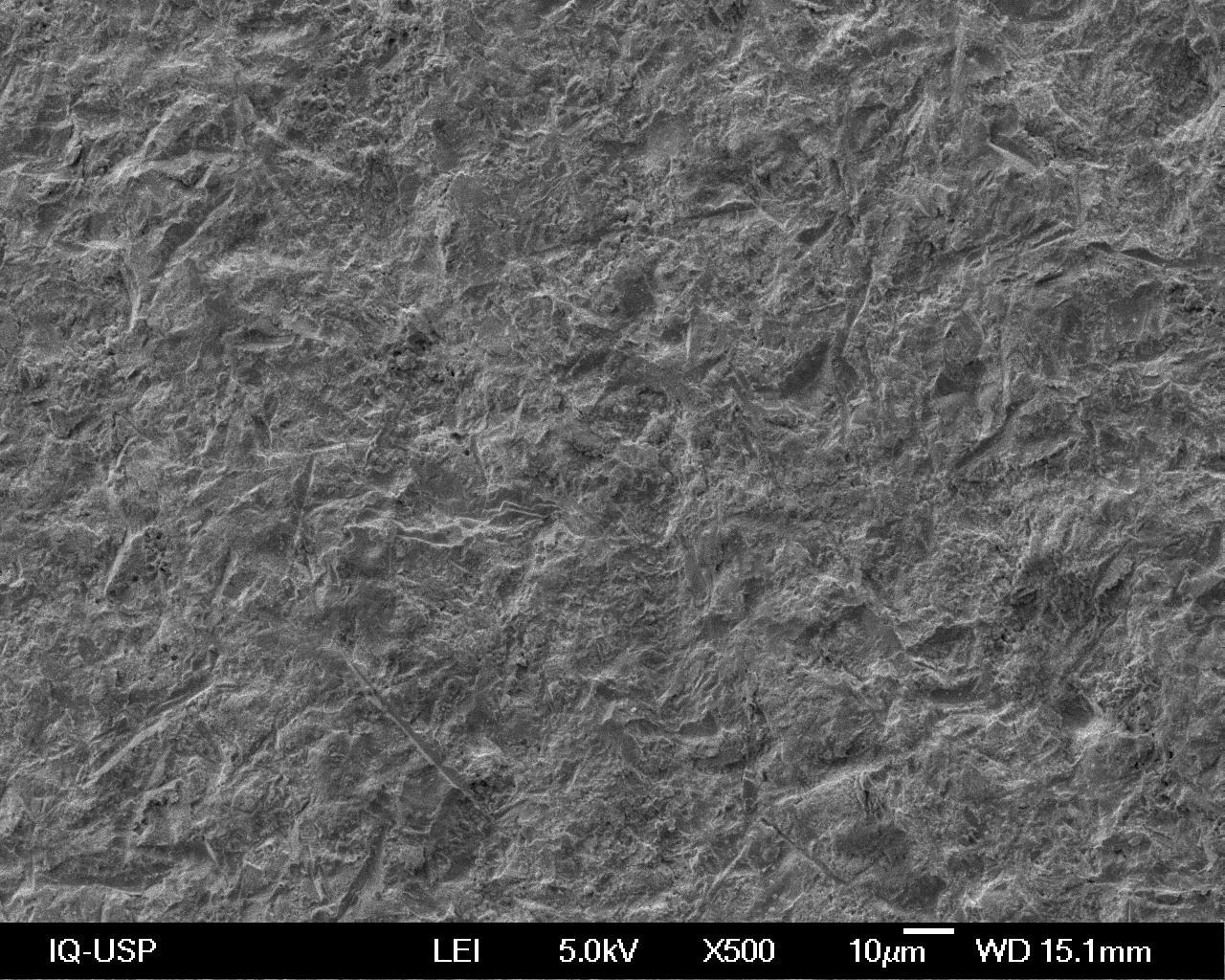
Figure 2 illustrates the surface topographies in Titanium and Zirconia (Y-TZP) after micro-sandblasting with aluminum oxide (AO) treatment. It is observed that the treatment with AO created a more irregular topography than that observed in figure 1, for both materials.
A B
Figure 2: A and B surfaces of Titanium (A) and Zirconia (Y-TZP) (B) after microblasting with aluminum oxide (AO).
The creation of textures on the surface of titanium implants, in turn, favors cell stimulation and bone formation, shortening treatment time (Matsunaka et al., 2003; Santiago et al., 2005) [32,33]. Such textures aim to increase chemical and mechanical bonding to the bone (Zhu et al., 2004) [34] and can be obtained by surface treatment methods, such as coating, mechanical treatment and chemical treatment (dos Santos, 2008; Gardin et al., 2014) [35,36]. In this study, the mechanical treatment of blasting was selected aiming at increasing surface roughness as well as topography of the implants creating irregular and retentive areas (Coelho et al., 2009) [37]. The mechanical treatment of blasting may be performed using microparticles of titanium, aluminum, silica or calcium phosphate (Dos Santos, 2008; Coelho et al., 2009; Hofstetter et al., 2013; Gardin et al., 2014) [35-38], which is known as microblasting. Microblasting (a term used in this study) is a simple, cost-effective procedure that promotes cleaning and increased surface energy (Belo et al., 2013) [39]. The surface energy of a biomaterial is an important factor to be taken into account, since it can also influence cell adhesion and proliferation (Santiago et al., 2005, Kubies et al., 2011, Aboushelib et al., 2013, Altmann et al., 2013) [33,40-42].
The visual analysis of the photomicrographs in Figure 2 (AO) compared to those of Figure 1 (MA) revealed clear retentive areas as well as changes to surface topography promoted by AO, which may favor cell adhesion, proliferation and differentiation (Wenz et al., 2008; Tomsia et al., 2011; Gardin et al., 2014) [7,36,43]. Qualitative analysis suggested at first that the surfaces of the two materials resemble each other after microblasting (Ozkurt & Kazazoglu, 2011) [44]. However, closer examination of figure 2B shows that AO-treated zirconia (Y-TZP) resulted in sligh more rounded and less pronounced retentions when compared to titanium (figure 2A), which is also observed in the relevant literature (Hempel et al., 2010, Altmann et al., 2013) [40,45]. This may be explained by the hardness of the zirconia, which would prevent the same pattern from being observed on titanium (Della Bona et al., 2007) [46].
Figure 3 shows the surface topography features in Titanium and Zirconia (Y-TZP) after microblasting with silicic acid-modified aluminum oxide (SMAO). In this figure, increased irregularities were also observed following treatment with SMAO, differently from that observed in figures 1 and 2 for the two surfaces.
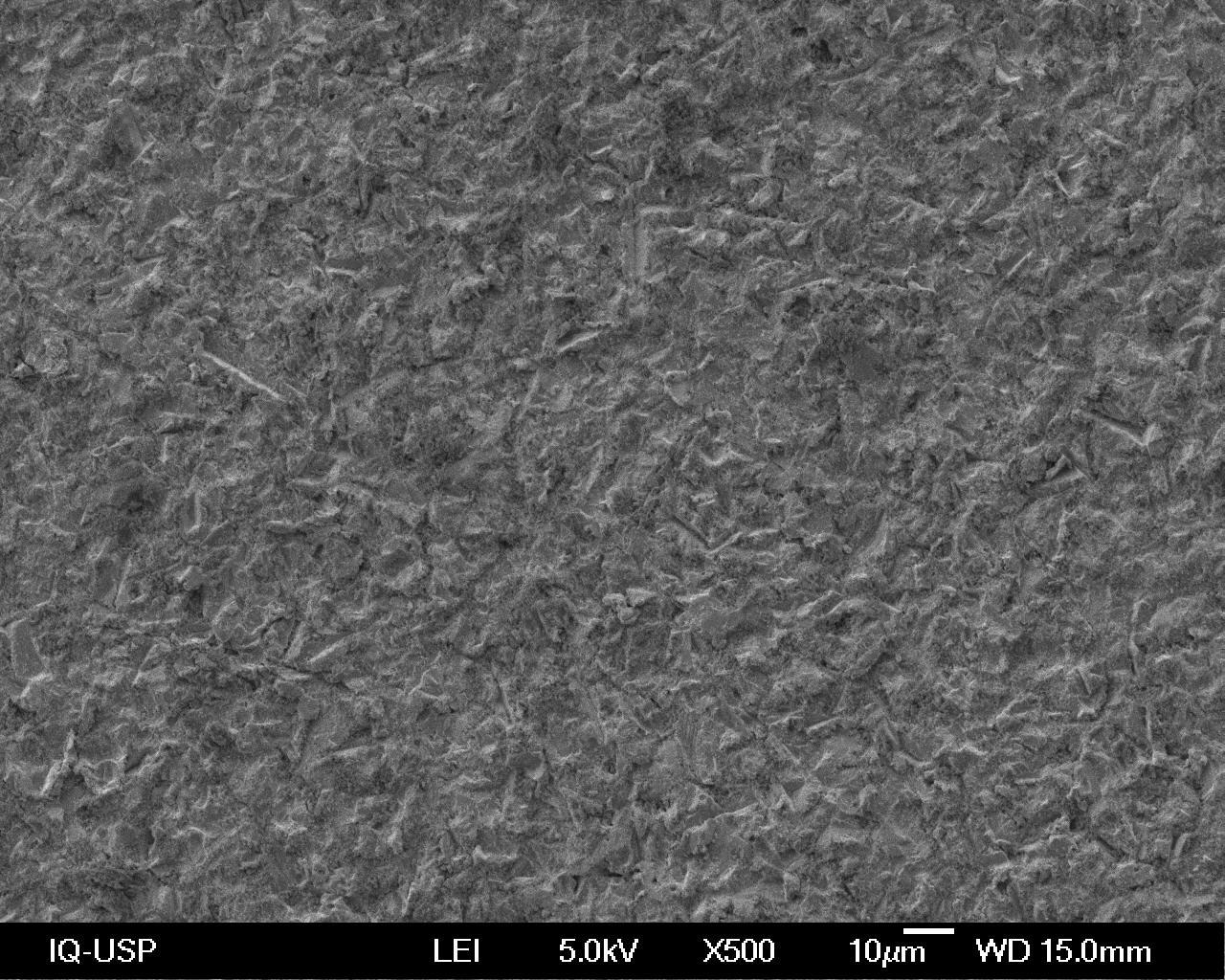
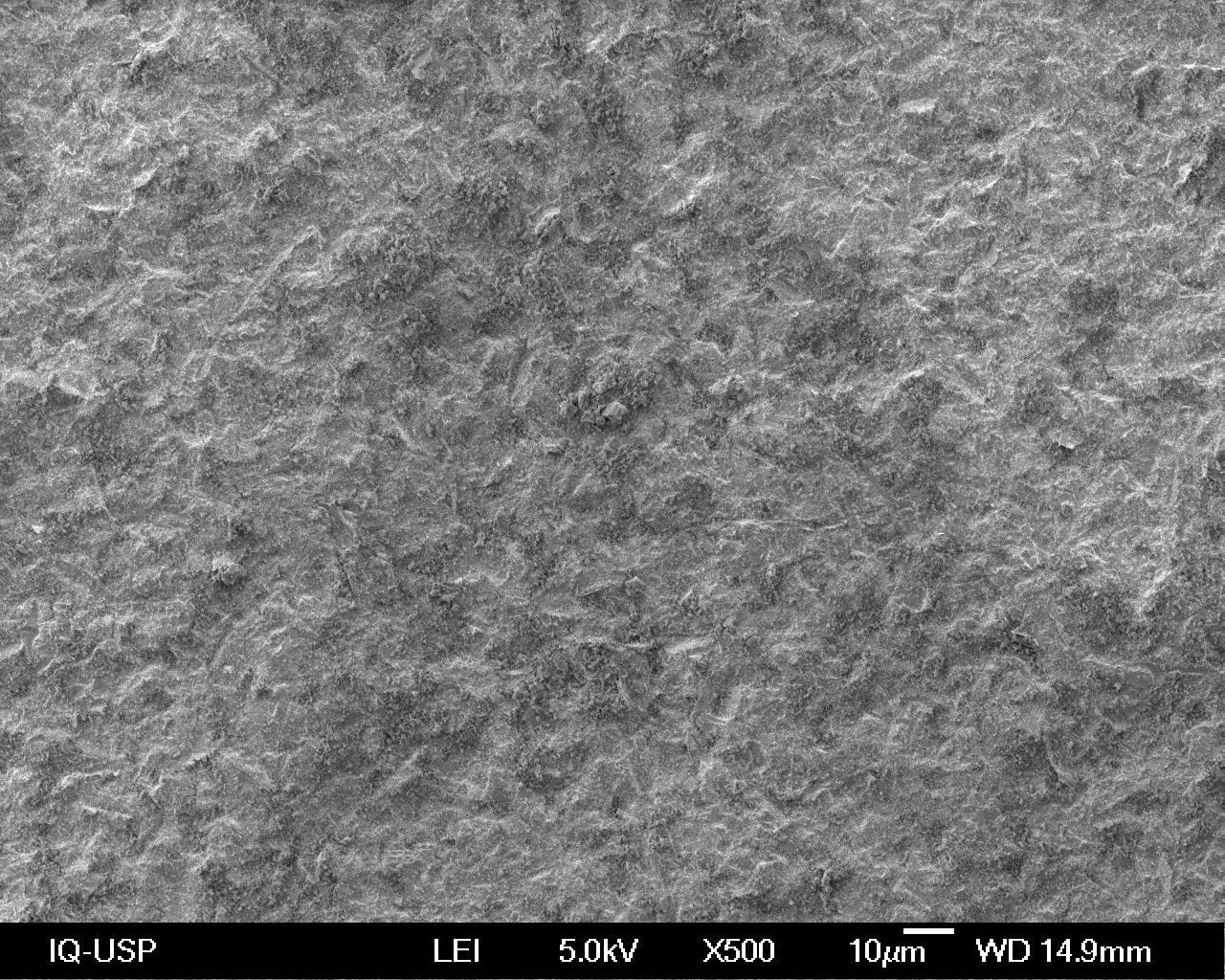
Figure 3: In A and B surfaces of Titanium and Zirconia (Y-TZP), respectively, after microblasting with silicic acid-modified aluminum oxide (SMAO).
The surface treatment with silica for implants presented in the literature usually requires an expensive and complicated methodology (Pelaez-Vargas, 2011; Martínez-Ibáñez et al., 2016) [47,48]. Thus, a simple and rapid method that promotes deposition of silica on the surface of materials was adopted in this study (SMAO group). The method proposes microblasting of the surface with 30-μm aluminum oxide powder treated with silica, which can provide a concentration of up to 76% silica on the treated surface (Della Bona et al., 2015) [49]. In Figures 3A and 3B (SMAO), a rough surface with irregular topography and a slightly less rough appearance can be observed when compared to Figures 2A and 2B (AO). The grain of the Cojet Sand abrasive powder is lesser (30 μm) than that for aluminum oxide (50 μm), which may be the reason behind the difference in irregularity and topography, since pressure, time and the distance between the microblasting source and the object remained constant (Coelho et al., 2009). When further analyzing figures 3A and 3B (SMAO) in relation to Figures 2A and 2B (AO), a more “milky” or “opaque” topography was observed on the former, which is most likely to be the result of covering granules or particles of fused silica onto the surface (Sarmento et al., 2011) [25].
Surface features such as macro and microtopography as well as chemical composition affect short-term cellular responses such as migration and cell adhesion, proliferation as well as differentiation and expression of mineralized matrix (Teixeira et al., 2009; Hempel et al., 2010) [45,50]. This may affect the process of osseointegration, as it has been shown to be an important factor in the process of osseointegration.
CELL PROLIFERATION
The pre-osteoblastic cell line selected for this study was that derived from rat calvaria (MC3T3-E1) as per previous studies (Yamashita et al., 2009; Watanabe et al., 2012; Ito et al., 2013; Umeazawa (1998)) [20,31,40,51,52] although other different cell lines have also been reported (Josset et al., 1999, Bächle et al. Aboushelib et al., 2013, Altmann et al., 2013, Herath et al., 2015, Mesquita et al., 2015) [41,42,53-56]. Such methodological difference may lead to different conclusions when comparing results.
The analysis of the data at different time periods has shown that the results are both material and treatment dependent (Table 1, graph 1). At 24 hours, two-way ANOVA (p = 0.05) followed by Tukey’s tests showed that, for titanium, surface treatment with SMAO promoted a significantly higher proliferation of osteoblastic cells than the group treated with AO and the group with no treatment (MA). No significant difference was observed between the latter two groups. On zirconia, the different surface topographies did not affect cell proliferation. Furthermore, no significant difference in osteoblast proliferation was found between titanium and zirconia when the surface remained untreated (MA) or when it was treated with AO. When samples were treated with SMAO, osteoblast proliferation on titanium was significantly higher than that on zirconia (Table 1, Graph 1).
Table 1: Mean and standard deviation of cell proliferation (cells/mm2) according to biomaterial, surface treatment and time.
|
Time |
Surface treatment |
Biomaterial |
Overall Mean |
|
|
Titanium |
Zirconia |
|||
|
24 hours |
MA |
0.44x104 Ba (0.08x104) |
0.45x104 Aa (0.03x104) |
¾ |
|
AO |
0.48x104 Ba (0.05x104) |
0.42x104 Aa (0.09x104) |
¾ |
|
|
SMAO |
0.64x104 Aa (0.03x104) |
0.39x104 Ab (0.05x104) |
¾ |
|
|
48 hours |
MA |
0.83x104Aa (0.17x104) |
0.73x104 Bb (0.01x104) |
¾ |
|
AO |
0.73x104 Bb (0.08x104) |
0.92x104 Aa (0.10x104) |
¾ |
|
|
SMAO |
0.76x104 Abb (0.06x104) |
0.75x104 Bb (0.07x104) |
¾ |
|
|
72 hours |
MA |
1.81x104 (0.18x104) |
2.22x104 (0.15x104) |
2.01x104a (0.27x104) |
|
AO |
1.69x104 (0.15x104) |
2.13x104 (0.09x104) |
1.91x104a (0.26x104) |
|
|
SMAO |
1.85x104 (0.06x104) |
2.34x104 (0.15x104) |
2.09x104a (0.29x104) |
|
|
Overall mean |
1.78x104B (0.14x104) |
2.23x104A (0.15x104) |
¾ |
|
Graph 1: Bar chart of osteoblast proliferation on titanium and zirconia, according to surface treatment and time.
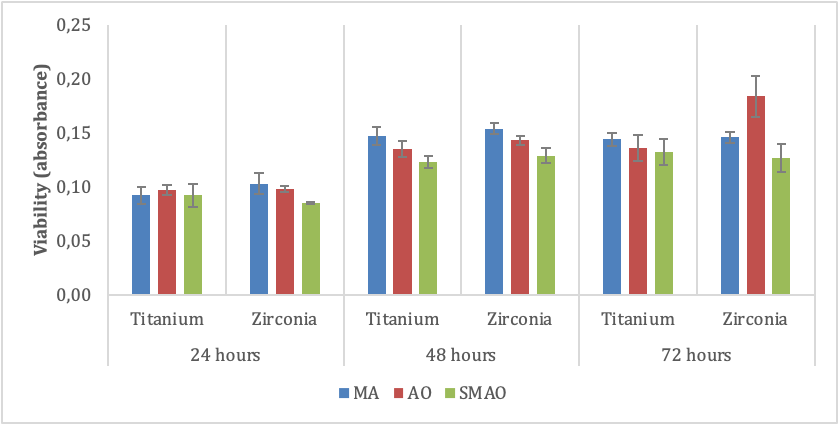
Legend: MA – machined surface – no microblasting; AO – aluminum oxide microblasting; SMAO – silicic acid-modified aluminum oxide microblasting
At 48 hours of culture, the two-way ANOVA (p = 0.055) and Tukey tests identified that, for titanium, the absence of treatment (MA) revealed a significantly higher cell proliferation than AO alone, while in the SMAO group, cell proliferation was intermediate. For Zirconia, the AO-treated surface showed significantly higher cell proliferation than MA and SMAO, and these two groups did not differ significantly between each other. When comparing the materials within each treatment, it was verified that in the MA group, cell proliferation was significantly higher on titanium, while AO reduced cell proliferation on the titanium surface. Finally, SMAO resulted in no significant difference between titanium and zirconia in terms of cell proliferation.
It was observed, therefore, that all the surfaces, smooth or treated, regardless of the material, allowed cell proliferation, be it higher or lower (table 1), which is in agreement with the reports found in the literature (Santiago et al., 2005; Bächle et al.,) [33,54].
There is no consensus among authors regarding the optimum surface preparation for adequate cell proliferation. In other words, while some studies show greater proliferation on smooth surfaces obtained from machining, abrasive grinding or polishing (Kubies et al., 2011; Herath et al., 2011) [40,55], others show that the creation of textures (roughness) using coating, mechanical, chemical treatments or combinations thereof may stimulate cell proliferation (Deppich et al., 2008; Kohal et al.,2009; Hempel et al.,2010; Aboushelib et al., 2013; Ito et al.,2013) [30,41,45,51,57]. Notwithstading that, some authors have reported no improvement in cell proliferation regardless of the roughness created (Santiago et al., 2005, Bächle et al., 2007, Yamashita et al., 2009, Mesquita et al., 2015) [31,33,54,56]. This variety of findings are also observed over time, namely 24h and 48h, between treatments and surfaces in terms of cell proliferation.
At 72 hours, a significantly higher cell proliferation was observed on the zirconia group, regardless of the treatment performed, in relation to the titanium group, which is according to Depprich et al. 2008 and Hempel et al.; 2010 [45,58], what may suggest a preference for this type of surface (chemical affinity) in terms of cell proliferation (Figure 1).
CELL VIABILITY ASSAY (MTT)
The two-way analysis of variance was applied to data collected at 24 hours and showed that the interaction between material and treatment was not significant (p = 0.134). It was also found that osteoblast proliferation was not significantly affected by the material (p = 0.653) nor treatment (p = 0.065; table 2, chart 2)
Table 2: Mean values and standard deviation of cell viability, as evaluated by absorbance, according to biomaterial, surface treatment and time.
|
Time |
Surface treatment |
Biomaterial |
Overall mean |
|
|
Titanium |
Zirconia |
|||
|
24 hours |
MA |
0.092 (0.008) |
0.103 (0.010) |
0.098a (0.010) |
|
AO |
0.097 (0.005) |
0.098 (0.003) |
0.098a (0.004) |
|
|
SMAO |
0.092 (0.011) |
0.085 (0.001) |
0.088a (0.008) |
|
|
Overall mean |
0.094A (0.008) |
0.095A (0.008) |
¾ |
|
|
48 hours |
MA |
0.147 (0.008) |
0.154 (0.005) |
0.151a (0.007) |
|
AO |
0.135 (0.007) |
0.143 (0.004) |
0.139b (0.007) |
|
|
SMAO |
0.123 (0.006) |
0.129 (0.007) |
0.126c (0.007) |
|
|
Overall mean |
0.135B (0.012) |
0.142A (0.012) |
¾ |
|
|
72 hours |
MA |
0.144 Aa (0.006) |
0.146 Ba (0.005) |
¾ |
|
AO |
0.136 Aa (0.012) |
0.184Ab (0.019) |
¾ |
|
|
SMAO |
0.132 Aa (0.012) |
0.127 Ca (0.013) |
¾ |
|
Legend: Standard deviation in brackets. Means followed by different capital letters indicate significant difference between materials, regardless of surface treatment. Overall means followed by different lowercase letters indicate significant difference between surface treatments, regardless of the biomaterial.
Means followed by different capital letters indicate significant difference within each column for each time period. Means followed by different lowercase letters indicate a significant difference within each row for each time period.
Graph 2: Bar diagram of cell viability on titanium and zirconia surfaces according to surface treatment and time.
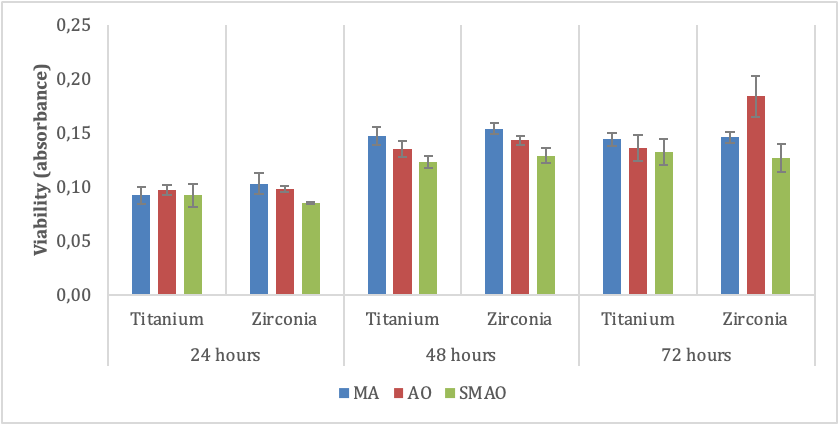
Legend: MA – machined surface – no microblasting; AO – aluminum oxide microblasting; SMAO – silicic acid-modified aluminum oxide microblasting
At 48 hours, two-way ANOVA demonstrated that the viability of osteoblastic cells was significantly higher on zirconia than on titanium (p = 0.046), regardless of surface treatment. The two-way analysis of variance (p <0.001) and the Tukey tests indicated that, either on titanium or zirconia, when SMAO was performed, cell viability was significantly lower than that verified when only AO was performed, which in turn, showed less cell viability than on the MA surface.
At 72 hours, two-way ANOVA (p = 0.005) and Tukey tests showed that cell viability was not significantly influenced by the microblasting, be it AO or SMAO. However, on the zirconia surface, the highest cell viability was verified on the AO-treated surface, which was significantly different from the values observed on the MA and SMAO surfaces, where the former was significantly higher (Table 2 graphic 2). No significant difference in osteoblast viability was observed between titanium and zirconia for MA or SMAO. In terms of AO, cell viability was significantly higher on the zirconia surface.
Increased cell viability at 24h and 48h suggests a proliferation increase in the same time periods, which was indeed the fact, as seen in table 1. Regardless of the surface treatment performed and the material used, the first 24 hours showed similarities without treatment or surface preference. At 48 hours, there was a predilection for the zirconia surface and this was statistically superior to that of the titanium. In relation to surface treatments, MA provided greater and significantly different cellular viability between AO and SMAO. At 72 hours, however, differences were observed. For, cell viability was not significantly different between the treatments, suggesting that the surface type did not influence cell viability in this period of time, although the viability values were not increased. On zirconia, the AO group presented the highest values of cell viability, which were significantly different from the others (chart 2). A numerical increase in cell viability may suggest a decrease in cell proliferation to initiate differentiation and secretion of specific markers of osteoblastic activity, such as osteopontin, a protein involved in the early stages of the mineralization process (Anselme, 2000; Tuan, 2011) [59,60].
Overall, cell viability increased, suggesting similar biocompatibility throughout the surfaces evaluated, especially at 72h, except for AO, which showed close similarity between surfaces, regardless of treatment (Herbergues et al., 2009; Herath et al., 2006) [55,61].
Wu et al. (2015) [62] demonstrated that cell viability could be better on rough surfaces than on smooth surfaces, a fact not observed in the present study. At 72 hours, cell viability was similar in most of the groups evaluated, with the exception of AO. Perhaps the fact that the authors reported using a titanium alloy, as opposed to grade 4 titanium, and a different methodological approach might have led to different outcomes.
Metal cytotoxicity depends on their position in the periodic table. Thus, the chemical elements present in this study, such as Ti, Zr, Al, and Si, belong to a group that does not cause cytotoxic reactions to living tissues (Kawahara, 1983) [63] and still allow cell proliferation, though with varied cellular activity (Zhang et al., 2016) [64], which could explain the differences observed in cell viability at 72 hours.
The mechanical treatment of microblasting to create textures and roughness may leave abrasive powder residue on the surface, such as Aluminum and Silica, and may negatively influence bone formation or contribute to different cellular and tissue responses (Santiago et al., 2005; Coelho et al., 2009; Zinelis et al., 2010; Martínez-Ibáñez et al., 2016) [33,37.48,65], although some studies that used this type of treatment showed the opposite, i.e., that there was no loss in cellular activity or bone formation (Coelho et al., 2009; Zinelis et al., 2010; Martínez-Ibáñez et al., 2016) [37,48,65] and the surfaces were biocompatible (Kohler et al., 2004; Bächle et al., 2007, Yamashita et al., 2009, Hempel et al., 2010; Martínez-Ibáñez et al., 2016) [33,54,31,45,48,66]. Aluminum, even if detected on the surface, seems to cause no harm to osseointegration (Zinelis et al. 2010) [65] and could explain the higher cell viability at 72h on the AO-treated zirconia group combined with its surface roughness feature.
The silica used in some studies aims to improve the bioactivity of a given material or induce bone growth (Kawahara, 1983; Pelaez-Vargas, 2011; Martínez-Ibáñez et al., 2016) [47,48,63]. However, its presence on the surface of titanium and zirconia showed different viability outcomes. While titanium did not negatively affect cellular viability, a decrease in viability was observed on zirconia, which was not similar to that observed on the smooth zirconia and the smooth titanium (control), although similar to the SMAO-treated titanium at 72h
Enzyme immunoassay for quantification of osteopontin (ELISA)
For osteopontin secretion (table 3, graph 3), two-way ANOVA (p = 0.041) and the Tukey’s test identified that, at 24 hours, osteopontin secretion on the SMAO-treated titanium surface was significantly superior to AO; however, when comparing the osteopontin data obtained on these surfaces with that of titanium (MA), no significant difference was identified. On the zirconia surface, the highest secretion of osteopontin was detected in the condition MA, followed by SMAO and AO, which proved to be the treatment with the lowest osteopontin secretion. The Tukey test further indicated that in MA, osteopontin secretion was significantly higher on zirconia. On the other hand, when AO was applied, osteopontin secretion was significantly higher on the titanium surface. Finally, for SMAO, no significant difference was observed between the titanium and zirconia surfaces in terms of osteopontin secretion.
Table 3: Mean values and standard deviation of osteopontin quantification (pg/ml), according to material, surface treatment and time.
|
Time |
Surface treatment |
Material |
Overall mean |
|
|
Titanium |
Zirconia |
|||
|
24 hours |
MA |
1.150Aab (0.149) |
1.348Aa (0.230) |
¾ |
|
AO |
1.032Ba (0.020) |
0.724Bb (0.104) |
¾ |
|
|
SMAO |
1.272Aa (0.083) |
1.089Ba (0.235) |
¾ |
|
|
48 hours |
MA |
1.259 (0.165) |
1.375 (0.117) |
1.375b (0.143) |
|
AO |
1.481 (0.100) |
1.475 (0.324) |
1.478 ab (0.214) |
|
|
SMAO |
1.427 (0.097) |
1.917 (0.067) |
1.672 a (0.279) |
|
|
Overall mean |
1.389 B (0.147) |
1.589 A (0.305) |
¾ |
|
|
72 hours |
MA |
1.860 (0.125) |
1.818 (0.035) |
1.839 a (0.085) |
|
AO |
2.020 (0.050) |
1.853 (0.231) |
1.936 a (0.175) |
|
|
SMAO |
1.540 (0.127) |
1.649 (0.107) |
1.595b (0.121) |
|
|
Overall mean |
1.806 A (0.231) |
1.773 A (0.160) |
¾ |
|
Legend: Standard deviation in brackets. Means followed by different capital letters indicate significant difference within each column, individually considering each time. Means followed by different lowercase letters indicate significant difference within each row, individually considering each time. Overall means followed by different capital letters indicate significant difference between materials, regardless of surface treatment. Overall means followed by different lowercase letters indicate significant difference between surface treatments, regardless of the material.
Graph 3: Bar chart of osteopontin expression by osteoblasts on titanium or zirconia, according to surface treatment and time.
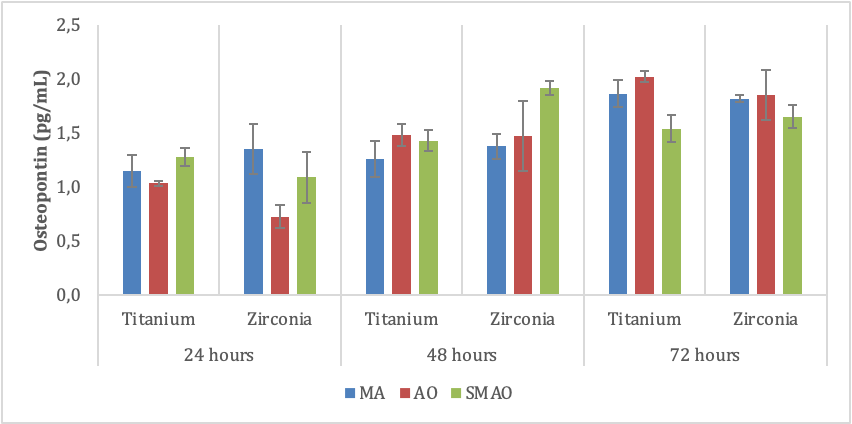
Legend: MA – machined surface – no microblasting; AO – aluminum oxide microblasting; SMAO – silicic acid-modified aluminum oxide microblasting.
At 48 hours of culture, two-way ANOVA identified that osteopontin secretion was higher on the zirconia surface (p = 0.027), regardless of AO or SMAO. It was also found that, on titanium or zirconia, surface treatments significantly affected osteopontin secretion (p = 0.011). Specifically, on the AO and SMAO-treated surfaces, the secretion of osteopontin was significantly superior to the MA surface, whereas when AO only was used, osteopontin secretion was intermediate, since no significant difference was identified when comparing this condition to the others.
At the 72 hours, the interaction material-treatment was not significantly different (p = 0.221, with 68.4% test power). Two-way analysis of variance showed no significant difference between the titanium and zirconia surfaces for osteopontin secretion (p = 0.600). On the other hand, surface treatment significantly affected the secretion of this protein (p = 0.002). The Tukey test showed that the surface secretion with AO only, or with MA, whose values did not differ significantly between each other, was higher than that observed on the SMAO surface. When analyzing table 2, at 72 hours, a decrease in cell viability was noticed for SMAO, which may suggest a less attractive surface for cellular interaction (silica). While the surface treatments (MA – OA) were not significantly different from each other, nor were they different from the control itself (titanium MA), SMAO both on titanium and zirconia showed a decrease in osteopontin secretion, which is a marker of bone mineralization (Stein, 1990; Bodine, 1996; Schenk, 1996) [67-69], when compared to the other groups. Another interesting aspect is that within each group, osteopontin increased over time, while within the group of titanium and zirconia treated with SMAO, the amount of osteopontin secretion hardly changed between 48h and 72h. The probable factor in the stabilization of the values in this group of zirconia with SMAO may have been the layer of silica adhered to the surface, inhibiting the osteoblasts to a certain extent from secreting this protein, as a response to the residual particles of silica (Setzerat et al.,2009ç Ecarot-Charrier et al., 1988) [70,71].
Cell morphology analysis
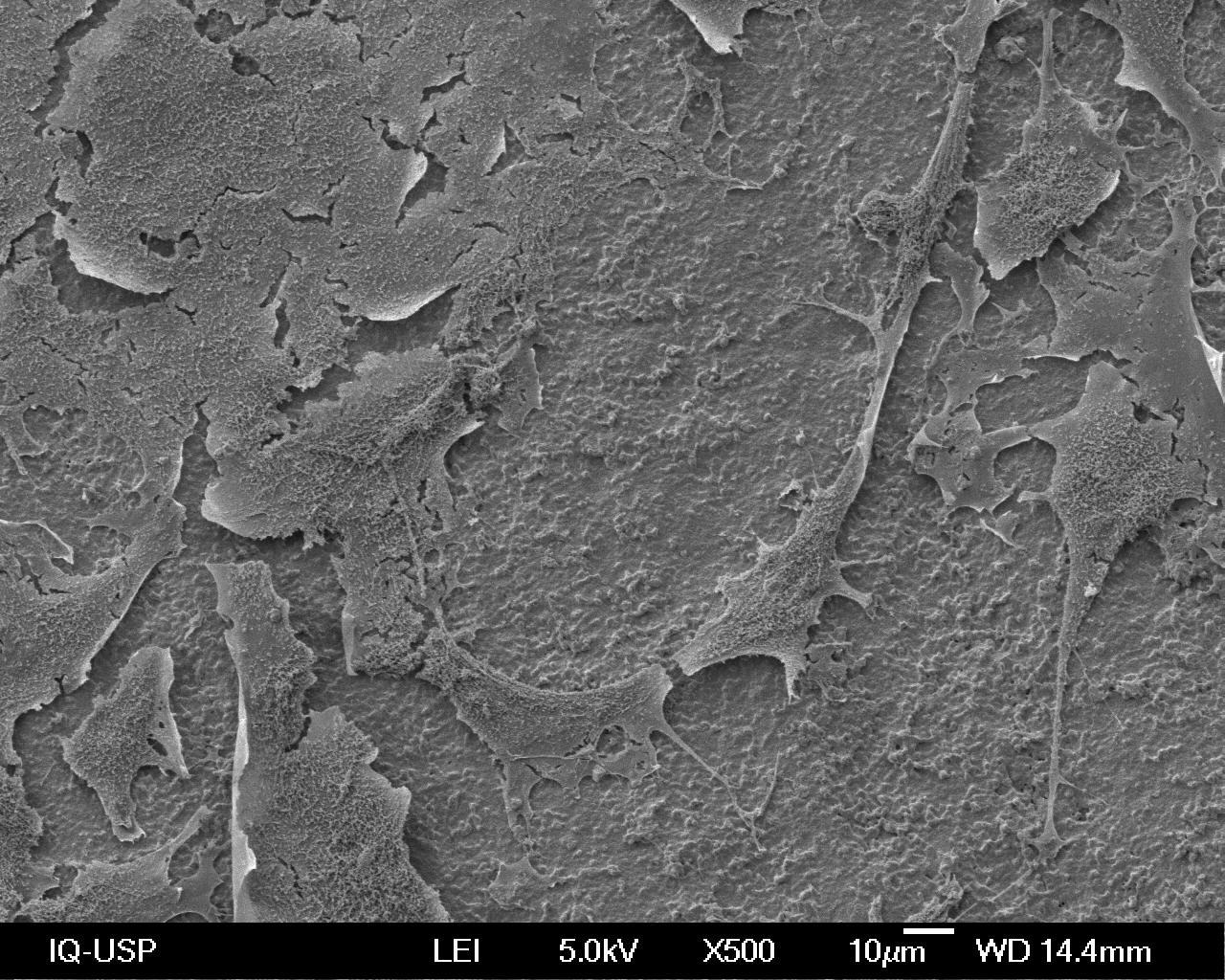
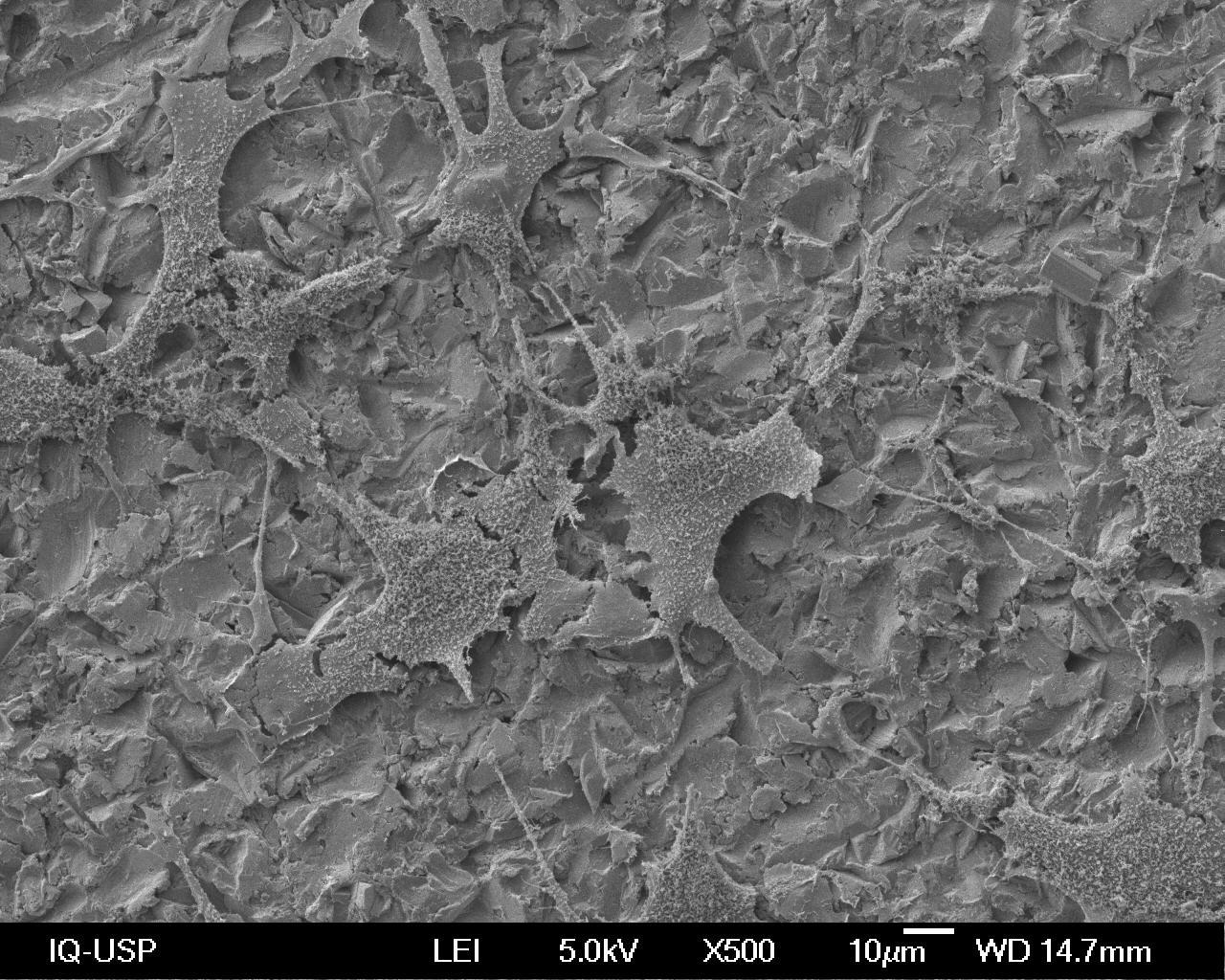
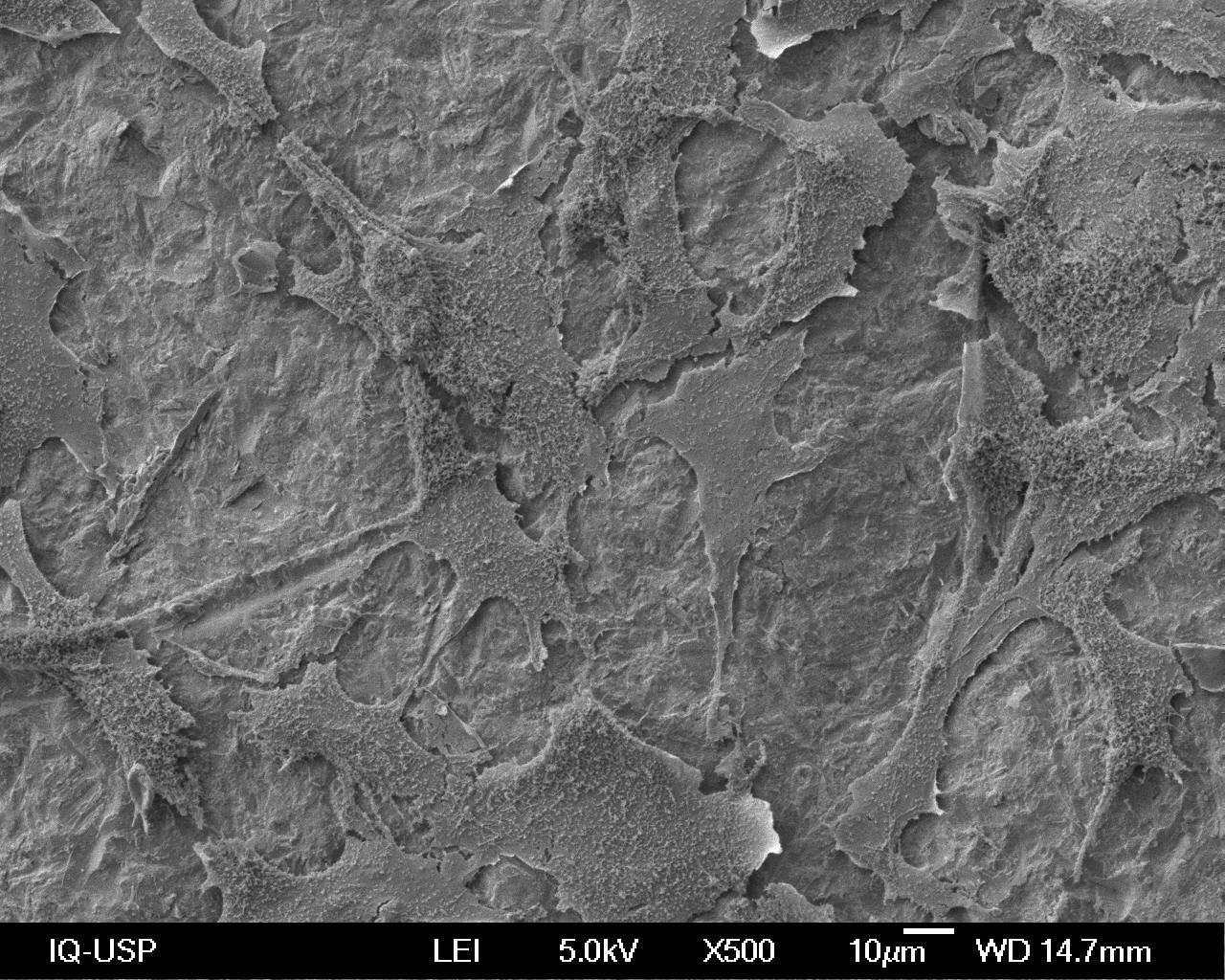
The different morphological aspects of the osteoblast cultures at 72h are illustrated in chart 1, which were assessed using SEM at 500 times magnification (X500) on the Titanium and Zirconia for dental prostheses (Y-TZP) surfaces after the treatments.
Chart 1: Osteoblast morphology according to the surface treatment performed.
|
|
Ti |
Zr |
|
MA |
|
|
|
AO |
|
|
|
SMAO |
|
|
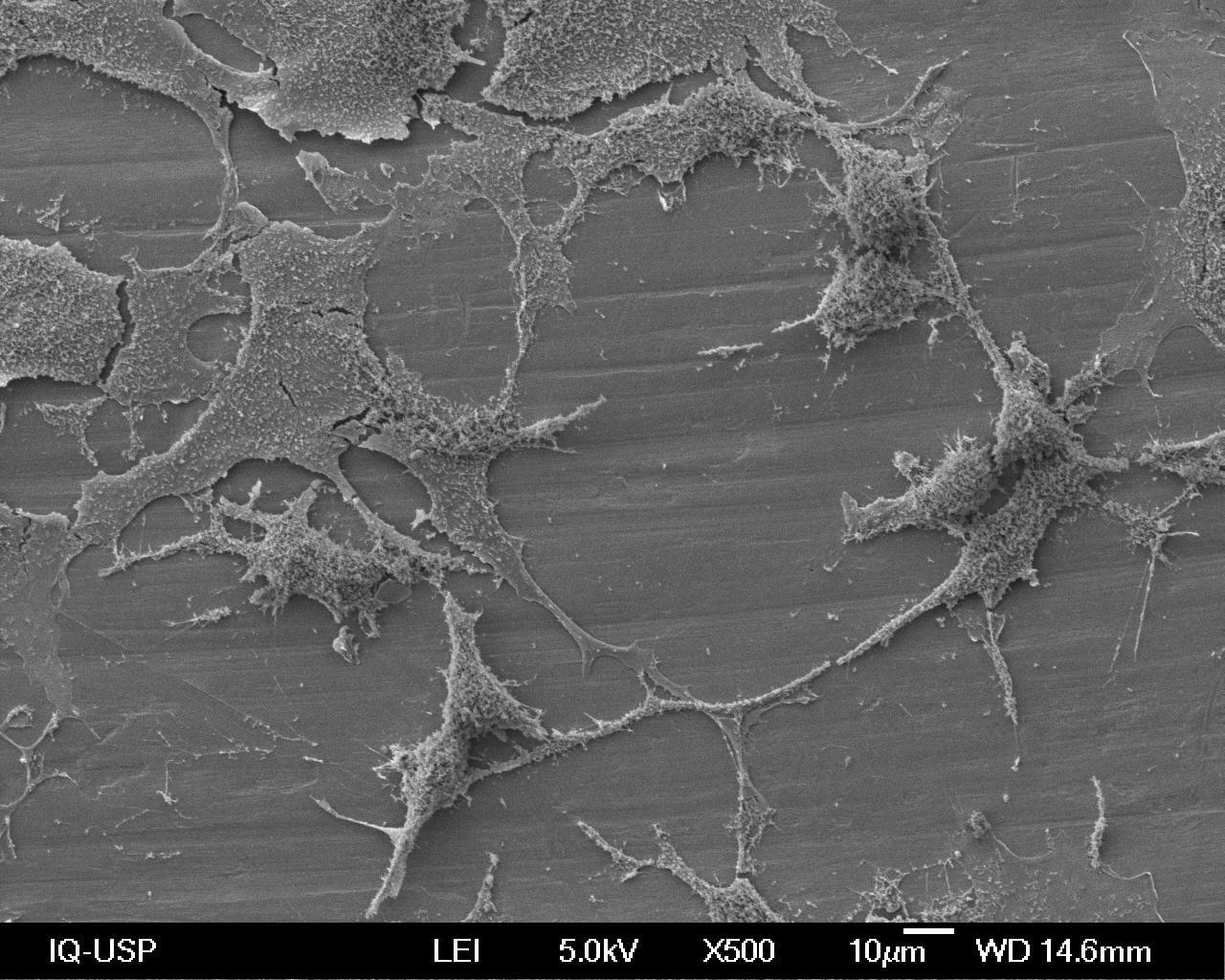
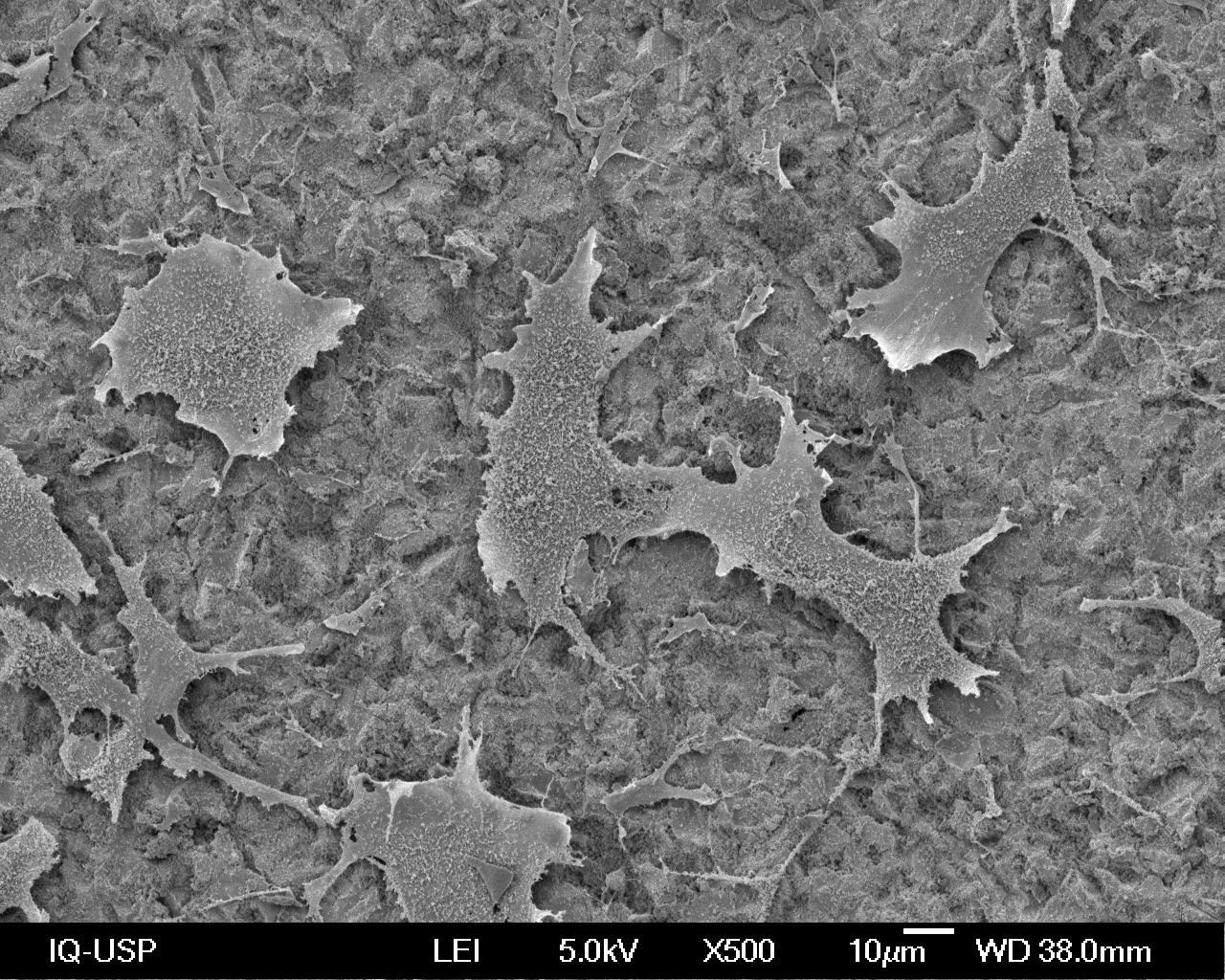
Bone growth on biomaterial is accompanied by surface features, be they topographic, chemical and surface energy, all of which play an important role on cell adhesion to such biomaterials. Therefore, bonding, adhesion and spreading correspond to the first phase of cell-biomaterial interaction and the quality of this phase (adhesion) may influence the morphology of osteoblast and their ability to proliferate and differentiate onto a dental implant (Anselme, 2000; Coppini et al., 2006; Teixeira et al., 2009; Hempel et al., 2010) [45,50,59,71].
As seen in Tables 1, 2 and 3, cell proliferation, viability and osteopontin expression over time suggest active and secretory osteoblasts on all surfaces evaluated, although when using SMAO, stabilization in values was observed. The presence of titanium and zirconia and the different types of treatment may influence cell morphology (Josset et al., 1999; Gard et al., 2014, Wu et al., 2015) [36,53,62]. On the smooth surface of Ti (MA), osteoblasts with many long and thin cytoplasmic projections connected to each other could be seen spreading along the grooves left by the machining process (Alves and Wassal, 2009) [72] in variable sizes and mostly with a flattened cell aspect (Wu et al., 2015) [62].
On the smooth zirconia surface (MA), flattened cells were also seen with some cytoplasmic projections trying to connect to each other though more scattered than on the titanium surface (Aboushelib et al., 2013) [41]. Overall, there was considerable similarity between these two phenotypes, independent of the surface, be it Ti or Zr (Depprich et al., 2008; Kohal et al., 2009) [58,66], although on the titanium surface, the dendritic projections were thinner and longer, while on zirconia, they appear shorter (Araujo, 2013) [73].
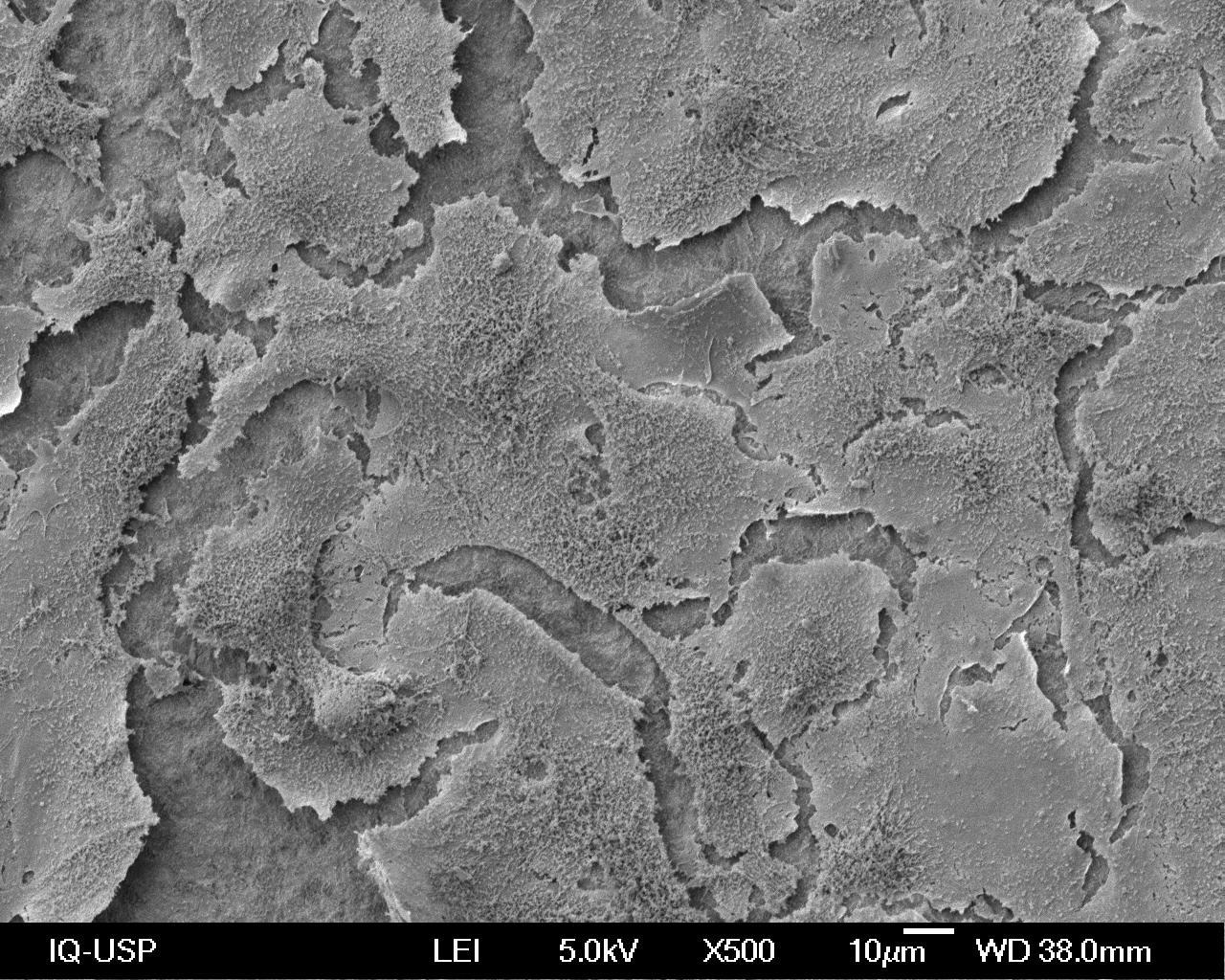
When the photomicrographs of titanium and Zirconia treated with AO are compared, a difference is observed mainly in relation to the size of the cells. Both show a generally flat appearance and the cells on the AO Zr surface are larger and show fewer dendritic projections than on the AO Ti surface. Furthermore, they do not appear to be confined to the grooves or retentions and with few lateral ramifications (Wu et al., 2015) [62]. They also present a polygonal shape and appear to grow throughout the surface (Alves and Wassal, 2009) [72].
When analyzing the images from the SMAO-treated surfaces, the osteoblasts showed the greatest difference in morphology between the two biomaterials. On titanium, the cells show a polygonal shape with dendritic projections and smaller sizes, these resemble the cells on the AO Ti surface. On the Zirconia surface, the cells appear larger, flatter and with no dendritic projections, hindering the visualization of cell outline and the surface below (Pelaez-Vargas, 2011; Herath et al., 2015) [47,55]. On Zirconia, morphological differences were found, according to the treatments used, which is not corroborated by a similar study (Yamashita et al., 2009) [12].
It was observed that surface topography and biomaterial can influence the morphology of osteoblastic cells (Anselme, 2000; Depprich et al., 2008; Aboushelib et al., 2013); Altmann et al., 2013, Gardin et al., 2014; Herath et al., 2015; Mesquita et al., 2015; Wu et al., 2015) [36,41,42,55,56,58,59,62]. Ecarot-Charrier et al. (1988) [71] reported that osteoblasts in a less active state become flattened and lose their ultrastructural characteristics of protein-producing cells, and this morphology can be observed in most of the photomicrographs in Table 1 for zirconia treated with AO and SMAO, though such flattened appearance did not prevent cell viability nor osteopontin secretion, although the values stabilized when the surfaces were treated with SMAO.
Regardless of the morphological differences presented by the osteoblasts on the different surface treatment conditions and the materials used, cell proliferation capacity, viability and osteopontin secretion were preserved.
Clinical manipulation of zirconia for dental prosthesis in the manufacturing process of dental implants may, in the not too distant future, be another possibility for dental surgeons in the rehabilitation of their patients. Nevertheless, surface treatments should be further investigated, since they may affect the viability and secretion of cells involved in bone formation.
CONCLUSIONS
The different surface treatments, both titanium and zirconia for dental prosthesis, promoted different cell/substrate interactions in the early cellular adaptation events.
In conclusion
Cell proliferation at the end of the evaluated period was higher and significantly different on zirconia for dental prostheses compared to titanium, but no significant differences between the treatments were found. Cell viability, however, was verified on all treated surfaces for both materials, though microblasting with aluminum oxide (AO) on zirconia for dental prosthesis showed the highest values of cell viability.
Osteoblastic secretion occurred on all surfaces and treatments at different time points. At 72 h, no statistical difference was observed between titanium and zirconia for dental prosthesis. However, the least favorable condition was that in which the surfaces were treated with silicic acid-modified aluminum oxide (SMAO) microblasting.
Visual evaluation of the ultrastructural topographic features of the treated surfaces showed a difference between smooth titanium and zirconia for dental prosthesis (MA), suggesting greater smoothness on the titanium surface. However, the treatments with aluminum oxide (AO) silicic acid-modified aluminum oxide (SMAO) microblasting on titanium and zirconia produced textures that are potentially rougher than those observed on titanium and zirconia for dental prosthesis with no microblasting (MA).
Osteoblast morphology differed according to surface treatment as well as to material, namely titanium or zirconia.
REFERENCES
- Zarb GA. (1983). Proceedings of the Toronto Conference on Osseintegration in Clinical Dentistry. St Louis: The CV Mosby Co.
- Azevedo VVC, Chaves AS, Bezerra DC, Costa CFM. (2008). Materiais cerâmicos utilizados para implantes. Rev Eletron Mat Process (REMAP): 3(1):31-39.
- Andreluolo R, Gonçalves AS, Dias KRHC. (2011). A zircônia na Odontologia Restauradora. Rer Bras Odontol. 68(1): 49-5311.
- Tschernitschek H, Borchers L, Geurtsen IW. (2005). Nonalloyed titanium as a bioinert metal – a review. Quintess Int. 36(7):523-530.
- Möller B, Terheyden H, Açil Y, Purcz NM, Hertrampf K, Tabakov A, et al. (2012). A comparison of biocompatibility and osseointegration of ceramic and titanium implants: an in vivo and In Vitro study. Int J Oral Maxillofac Surg. 41:638-645.
- Della Bona A. (2009). Adesão às cerâmicas. Evidências para o uso clínico. Cap 2,p.20-42.Artes Médicas: São Paulo, 2009.
- Wenz HJ, Bartsch J, Wolfart S, Kern M. (2008). Osseintegration and clinical success of zirconia dental implants: a systematic review. Int J Prosthod. 21(1):27-36.
- Özkurt Z, Iseri U, Kazazoglu E. (2010). Zirconia ceramic post systems: a literature review and a case report. Dent Mat J. 29(3).
- Moraes MCCSB. (2004). Microestrutura e propriedades mecânicas de compósitos alumina-zircônia para próteses dentárias. [tese]. Rio de janeiro: Instituto Militar de Engenharia.
- Hoffmann O, Angelov N, Gallez F, Jung RE, Weber FE. (2006). The treatment implant-bone interface: a preliminar histologic evaluation in rabbits. Int J of Oral Maxillofacial Implants. 23(4): 691-695.
- Andreiotelli M, Wenz Hj, Kohal R. (2009). Are ceramic implants a viable alternative to titanium implants? A systematic literature review. Clin Oral Impl Res. 20(Suppl.4):32-47.
- Yamashita A, Yamani T. (1982). How to make an adhesive bridge and apply it clinically. DE J Dent Eng. 60:1-11.
- Renk VA, Hartmann D. (1982). Untersuchengen über die haftfestigkeit von Palliag M-Komposite-Ätzbrücken nach vorbehandlung der metalloberfläche. Dtsch Zahnärztl Z. 37(12):957-960.
- Kühl VW, Renk A. (1982). Untersuchungen übe die haffestigkeit von isopast and palliag im zugversuch nach unterchiedlicher vorbehandlung der metalloberfläche. Dtsch Zahnärztl Z. 37(12): 961-963.
- Swift Jr EJ. (1989). New adhesive resins. A status report for the American Journal of Dentistry. Am J Dent. 2(6):358-360.
- Lin T, Chang H, Chung K. (1990). Interfacial strengths of various alloy surface treatments for resin-bonded fixed partial dentures. J Prosthet Dent. 64(2):158-162.
- Isidor F, Hassna N M, Josephsen K, Kaaber S. (1991) Tensile bond strength of resin-bonded non-precious alloys with chemically and mechanically roughened surfaces. Dent Mater. 7(4):225-229.
- McCaughey AD. (1993). Sandblasting and tin-plating- surface treatments to improve bonding with resin cements. Dent Update. 20(4):153-159.
- Latta MA, Barkmeier WW. (2000). Approches for intraoral repair of ceramic restorations. Comp Contin Educ Dent. 21(8):635-645.
- Watanabe H,Saito, K, Kokubun K, sasaki H, Yoshinari M. (2012). Change in surface properties of zirconia and initial attachment of osteoblast- like cells with hydrophilic treatment. Dent Mater J. 31(5):806-814.
- Frankenberger R, Krämer N, Sindel J. (2000). Repair strength of etched vs silica coated metal-ceramic and all-ceramic restorations. Oper Dent. 25(3):209-215.
- Herrmann W, Nergiz I, Özcan M, Schmage P, Platzer U. (2000a). Influence of conditioning methods on bond strengths between brackets and ceramic surfaces. J Dent Res. Chicago 79:435.
- Herrmann W, Nergiz I, Özcan M, Schmage P, Platzer U. (2000b). Influence of conditioning methods on bond strengths between brackets and ceramic surfaces. J Dent Res. Chicago 79:435.
- Castro HL. (2010). Avaliação de três cimentos resinosos na resistência de união entre dentina e uma cerâmica de zircônia estabilizada por ítria. [tese]. São José dos Campos: UNESP.
- Sarmento HR, Campos F, Sousa RS, Alves MLL, Machado JPB, Souza ROA. (2011). Influência de protocolos de jateamento na rugosidade da superfície de uma cerâmica de zircônia tetragonal parcialmente estabilizada por ítria. PesqBrasOdontopClinIntegr. 11(2):231-238.
- Baldissara P, Querzè M, Monaco C, Scotti R, Fonseca RG. (2013). Efficacy of surface treatments on the bond strength of resin cements to two brands of zirconia ceramic.J Adhes Dent. 15(3):259-267.
- Matsuzaka K, Walboomers XF, Yoshinari M,Inoue T, Jansen JÁ. (2003). The attachment and growth behavior of osteoblast-like cells on microtextured surfaces.Biomaterials. 24:2711-2719.
- Gapski R, Wang HL, Mascareñas P, Lang NP. (2003). Critical review of immediate implant loading. Clin Oral Implant Res. 14: 515-27.
- Wieland M, Textor M, Chehroudi B, Brinette DM. (2005). Synergistic interaction of topographic features in the production of bone-like nodules on Ti surfaces by rat osteoblasts. Biomaterials. 26:1119-1130.
- Kohal RJ, Wolkewitz M, Hinze M, Han JS, Bächle M, Butz F. (2009). Biomechanical and histological behavior of zirconia implants: an experiment in the rat. Clin Oral Impl Res. 20:333-339.
- Yamashita D, Machigashira M, Miyamoto M, Takeuchi H, Noguchi K, Izumi Y, et al. (2009). Effect of surface roughness on initial responses of osteoblast-like cells on two types of zirconia. Dent Mat J. 28(4):461-470.
- Matsuzaka K, Wallboomers XF, Yoshinar M, Inouet T, Jansen JA. (2003). The attachment and growth behavior of osteoblast-like cells on microtextured surfaces. Biomaterials. 24:2711-2719.
- Santiago AS, Dos Santos EA, Sader MS, Santiago MF, Soares GA. (2005). Response of osteoblastic cells to titanium submitted to three diferente surfasse treatments. Bras Oral Res. 19(3):203-208.
- Zhu X, Chen J, Scheideler L, Reichl R, Geis-Gerstorfer J. (2004). Effects of topography and composition of titanium surface oxides on osteoblast responses. Biomaterials. 25:4087-4103.
- Dos Santos AR. (2008.). Efeito da oxidação anódica de titânio comercialmente puro revestido ou não com fibronectina na interface osteoblastos humanos-superfície de titânio. (Tese de Doutorado). Universidade Federal do rio de Janeiro. Rio de Janeiro, RJ – Brasil.
- Gardin C, Ferroni L, Bressan E, Calvo-Guirado JL, Degidi M, Piattelli A, Zavan B. (2014). Adult stem cells properties in terms of commitment , aging and biological safety of grit-blasted and acid-etched Ti dental implant surfaces. Int J Mol Cell Med. 3(4):225-236.
- Coelho PG, Granjeiro JM, Romanos GE, Suzuki M, Silva NR, Cardaropoli G et al. (2009). Basic research methods and current trends of dental implant surfaces. J Biomed Mater Res Part B. 88(2):579-596.
- Hofstetter W, Sehr H, Wild M, Portenier J, Gobrecht J, Hunziker EB. (2013). Modulation of human osteoblasts by metal surface chemistry. J Biomed Mat Res. 101(A):2355-2364.
- Belo YD, Souza QN, Borba M, Bona AD. (2013). Zircônia tetragonal estabilizada por ítria: comportamento mecânico, adesão e longevidade clínica. Cerâmica. 59:633-639.
- Kubies D, Himmlova L, Riedel T, Chanova E, Balik K, Douderova M, et al. (2011). The interactions of osteoblastos with bone -implant materials: 1 the effect of physicochemical surface properties of implants materials. Physiol. Res. 60: 95-111.
- Aboushelib MN, Osman E, Jansen I, Everts V, Feilzer AJ. (2013). Influence of a Nanopouros zirconia implant surface of on cell viability of human osteoblasts. J Prosthodont. 22:190-195.
- Altmann B, Kohal RJ, Steinberg T, Tomakidi P, Bächle-Hass M, Wennerberg A, Att W. (2013). Distinct cell functions of osteoblasts on UV-functionalized titanium and zirconia based implant materials are modulated by surface topography. Tissue Eng Part C Methods. 19(11):850-863.
- Tomsia AP, Launey ME, Lee JS, Mankani MH, Wegst UG, Saiz E. (2011). Nanotechnology approaches to improve dental implants. Int J of Oral Maxillo Fac Implants. 26 Suppl:25-44; discussion 45-49.
- Özkurt Z, Kazazoglu E. (2011). Zirconia dental implants: a literature review. J Oral Implantol. 37(3):367-376.
- Hempel U, Hefti T, Kalbacova M, Wolf-Brandstetter C, Dieter P, Schlottig F. (2010) . Response of osteoblast~like SAOS-2 cells to zirconia ceramics with different surface topographies. Clin Oral Impl Res. 21:174-181.
- Della Bona A, Borba M, Benetti P, Cecchetti D. (2007). Effect os surface treatments on the bond strength of a zirconia-reinforced ceramic to composite resin. Bras Oral Res. 21(1):10-15.
- Pelaez-Vargas A, Gallego-Perez D, Magallanes-Perdomo M, Fernandes MH, Hansford DJ, De Aza AH, et al. (2011). Isotorpic micropatterned reatm coatings on zirconia induce guided cell growth for dental implants. Den Mat. 27:581-589.
- Martínez-Ibáñez M, Juan-Díaz MJ, Lara-Saez I, Coso A, Franco J, Gurruchaga m, et al. (2016). Biological characterization of a new silicone based coating developed for dental implants. J Mater Sci: Mater Med. 27:80.
- Della Bona A, Pecho OE, Alessandretti R. (2015). Zirconia as a Dental Biomaterial. Materials. 8:4978-4991.
- Teixeira LJC, Dos Anjos CM, Soares MM, Vidigal Jr GM, Conz MB. (2009). Cultura de células na implantologia oral: revisão de Literatura. Rev implant. 6(5):479-483.
- Ito H, Sasaki H, Saito K, Honma S, Yajima Y, Yoshinar M. (2013). Response of osteoblast-like cells to zirconia with different surface topography. Dent Mat. 32(1):122-129
- Umezawa T, Chen P, Tsutsumi Y, Doi H, Ashida M, Suzuki S, et al. (2015). Calcification of MCV3T3-C1 cels on titanium and zirconium. Dent Mater J. 34(5):713-7118.
- Josset Y, Oum´Hamed Z, Zarrinpour A, Lorenzato M, Adnet JJ, Laurent-Maquin D. (1999) .In Vitro reactions of human osteoblasts in culture with zirconia and alumina ceramics. Jbiomed Mater Res. 47(4):481-493.
- Bächle M, Butz F, Hübner U, Bakalinis E, Kohal R. (2007). Behavior of CAL72ostoeblast-like cells cultured on zirconia ceramics with different surface topographies. Cin Oral Impl Res. 18:53-59.
- Herath HMTU, Di Silvio L, Evans JRG. (2015). Osteoblast response to zirconia surfaces with different topographies. Mater Sc Enginn C. 57:363-370
- Mesquita P, Felino A, Raposo H, Afonso A. (2015). Avaliação “in vitro” do comportamento de osteoblastos sobre implantes com diferentes tratamentos de superfície. Rev Port Estomatol Med Dent Cir Maxilofac. 56(2):95-102.
- Depprich R, Ommerborn M, Zipprich H, Naujoks C, Handschel J, Wiesmann HP, et al. (2008). Behavior of osteoblastic cells cultured on titanium and structures zirconia surfaces. Head Face Med. 4:29.
- Anselme K. (2000). Osteoblast adhesion on biomaterials. Biomaterials. 21:667-681
- Tuan RS. (2011). Role of adult stem/progenitor cells in osseointegration and implant loosening. Int J Oral Maxxillofac Implants. 26:50-62.
- Hisbergues M, Vendeville S, Vendeville P. (2009). Zirconia: established facts and pespectives for a biomaterial in dental implantology. J Biomed Mat Res. Part B: Appl Biomater. 88B:519-529.
- Wu C, Chen M, Zheng T, Yang X. (2015). Effect of surface roughness on the initial response of MC3T3-E1 cells cultured on polished titanium alloy. Bio-Med Mater and Engineering. 26:S155-S164.
- Kawahara H. (1983). Cellular responses to implant materials: biological, physical and chemical factors. Int Dent J. 33(4):350-375.
- Zhang D,Wong CS, Wen C, Li Y. (2016). Cellular responses of osteoblast-like cells to seventeen elemental metals. J Biomed Mater Res A. 105(1):148-158.
- Zinelis S, Thomas A, Syres K, Silikas N, Eliades G. (2010). Surface characterization of zirconia dental implants. Dent Mat. 26:295-305.
- Kohal RJ, Weng D, Bächle M, Strub JR. (2004). Loaded Custom-made zirconia and titanium implants show similar osseointegration: an animal experiment. J Periodontol. 75:1262-1268.
- Stein GS, Lian JB, Owen TA. (1990). Relationship of cell growth to the regulation of tissue – specific gene expression during osteoblast differentiation.FASEB J. 4:3111-3123.
- Bodine P, Trailsmith M, Komm B. (1996). Development and characterization of a conditionally transformed adult human osteoblastic cells line. J Bone Miner Res. 11(6):1-19.
- Schenk RK. (1996). Regeneração óssea: bases biológicas. In: Buser D, Dahlin C, Schenk RK. Regeneração Óssea: bases biológicas. São Paulo: Quintessence.
- Setzer B, Bächle M, Metzger MC, Kohal RJ. (2009). The gene expression and phenotypic response of Hfob 1.19 osteoblasts to surface-modified titanium and zirconia. Biomaterials. 30:979-990.
- Ecarot-Charrier B, Shepard N, Charrete n, Grynpas M, Glorieux FH. (1988). Mineralization in osteoblast cultures: a light and electron microscopic study. Bone. 9:147-154.
- Coppini LP, Duarte MAT, Lucchesi C, Duek EAR. (2006). Cultura de osteoblastos sobre blendas de pldla / pcltriol. 17º CBECIMat – Congresso Brasileiro de Engenharia e Ciência dos Materiais, 15 a 19 de Novembro de 2006, Foz do Iguaçu, PR, Brasil.
- Alves SF, Wassal T. (2009). In Vitro evaluation of osteoblastic cell adhesion on machined osseointegrated implants. Braz Oral Res. 23(2):131-136.
- Araújo LDE. (2013). Avaliação “in vitro” da adesão e proliferação de osteoblastos na superfície de implantes de zircônia. [tese de mestrado]. Campinas. São Leopoldo Mandic.