Information Links
Related Conferences
Previous Issues Volume 8, Issue 5 - 2023
How In Situ Simulation can Facilitate Implementation Science Interventions for Formalisation of an Emergency Neonatal Obstetric Code (ENOC)
Fatimah Lateef1,2,3,*
1Senior Consultant, Department of Emergency Medicine, Singapore General Hospital, Singapore
2Professor, Duke NUS Graduate Medical School, Yong Loo Lin School of Medicine, National University of Singapore and Lee Kong Chian Medical School, Nanyang Technological University, Singapore
3Director, Sing Health Duke NUS Institute of Medical Simulation (SIMS), Singapore
*Corresponding author: Fatimah Lateef, FRCS (A&E), MBBS, FAMS, Department of Emergency Medicine, Singapore General Hospital, Outram Road, 1 Hospital Drive, Singapore 169608, Singapore, Tel: +65 632 149 72/3558; Fax: 65 632 148 73; E-mail: [email protected].
Received Date: October 07, 2023
Published Date: November 20, 2023
Citation: Lateef F. (2023). How In Situ Simulation can Facilitate Implementation Science Interventions for Formalisation of an Emergency Neonatal Obstetric Code (ENOC). Mathews J Emergency Med. 8(5):66.
Copyrights: Lateef F. © (2023).
ABSTRACT
Implementation science (IS) refers to the understanding and addressing of both the barriers and enablers to the incorporation and uptake of evidence-based practices and interventions. IS has evolved as a means to close the research to practice gap. At the same time, it can also help enhance the return on research investments. IS should provide guidance on themes, tools, resources, strategies as well as research design in the implementation of a program, a new pathway or a practice guideline. It must also focus on the implementation context, how to measure outcomes and how to report the implementation findings.
Simulation can help in the identification of barriers and latent threats as well as assist with familiarization with the enablers. Simulation is also useful for implementation mapping and the planning of implementation strategies. This paper discusses how a new emergency activation pathway, The Emergency-Neonatology-Obstetric Code (ENOC), will be implemented, in the context of an inter-professional team working together, at Singapore General Hospital (SGH). In situ simulation was used on several occasions to test out the proposed workflow, which was planned and conceptualized using the Updated Consolidated Framework for Implementation Research.
Keywords: Implementation Science, In Situ Simulation, Emergency- Neonatal-Obstetric Code, Implementation Framework.
ABBREVIATIONS
IS: Implementation Science; ENOC: Emergency-Neonatology-Obstetric Code; SGH: Singapore General Hospital; ED: Emergency Department; NIV: Non-Invasive Ventilation; ICU: Intensive Care Unit; CFIR: Consolidated Framework for Implementation Research; OG: Obstetrics and Gynaecology; EOT: Emergency Operating Theatre.
INTRODUCTION
Implementation science (IS) refers to the understanding and addressing of both the barriers and enablers to the incorporation and uptake of evidence-based practices and interventions. IS will involve determinants of adoption, implementation and sustainable maintenance. IS therefore includes both research and practice. In most academic institutions and departments, many would have been involved in some degree of implementation or changing practices and processes. When doing this, it is best to ensure appropriateness alignment with accepted framework or guidelines [1-6].
IS has evolved as a means to close the research to practice gap. At the same time, it can also help enhance the return on research investments. IS should provide guidance on themes, tools, resources, strategies as well as research design in the implementation of a program, a new pathway or a practice guideline. It must also focus on the implementation context, how to measure outcomes and how to report the implementation findings. The implementation process itself is important. Studies have shown that when programmes are properly implemented, the success rate, buy-in and results are better. Today, for institutions and department to not consider comprehensive and strategic implementation processes can be a costly error [5,7-8].
Simulation is the technique to replace or amplify real experiences with guided ones. It is powerful in evoking or replicating a substantial portion or aspects of real world practice, as it is immersive and experiential. Simulation-based education is applicable to many specialties and disciplines across various industries. It is an active learning process and in general, feedback from learners has been positive. It serves to demonstrate how carefully crafted experiential learning scenarios can impact both learners and eventually, patient care [9-12].
What Can Simulation Offer in the Process of Implementation?
Simulation can help in the identification of barriers and latent threats as well as assist in familiarization with the enablers. Simulation is also useful for implementation mapping and the planning of implementation strategies. Some examples would include using simulation to test out new workflow processes for infectious cases during the Covid-19 pandemic, charting a major trauma patient’s journey from the pre hospital setting into the Emergency Department (ED) and to the Emergency Operating Theatre, or even the simulated journey of a patient with respiratory distress and started on non-invasive ventilation (NIV) from the ED up to the Intensive Care Unit (ICU). There are many examples of such scenarios which are utilised on a day to day basis, in healthcare organizations [13-17].
Observations and results from laboratory studies, clinics and the community can be tested via simulation and pilot studies before finalization to incorporate into implementation techniques and methodologies which can improve the health of individuals and the population [9,17]. Simulation allows the testing out of some proposed implementation, innovation or change. However, between conducting the simulation, to understand behaviours and practices, to implementation, there are often time lag and gaps. To avoid this, it becomes important to chart timelines of activities to be accomplished, from the very beginning [18,19]. From the point where the concept of change is realized to the fact finding portion, research, simulation trials and a realistic timeline of workflow should be created [20-23]. Some degree of allowances for expected delays can be incorporated as well. Delays and gaps can lead to loss of opportunities, effectiveness and impact. Awareness and interest of staff may also dwindle. Sometimes, whilst waiting for adoption and implementation, the evidence may have evolved or changed, especially if the period of delay is prolonged [5,24-26] (Figure 1).
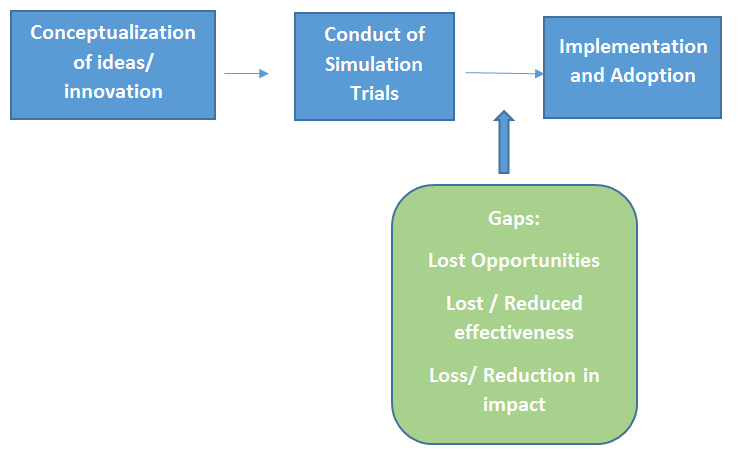
Figure 1. From Conceptualization to Implementation.
Simulation can be used in some of the following applications and ways [9,11,13,24,27,28]:
- To measure and predict the functioning of an existing system or a newly proposed system. Results may be affected by alteration in individual components and these may be tested through simulations
- To identify “bottlenecks” or points of overload and congestion in a system or workflow
- To test the “what if” effects, especially if there are various ideas for the innovation, and to select the most efficient and practical ones.
- To verify certain observations and expectations. In healthcare systems, many complex processes are involved and the use of simulation can give a better insight to the issues encountered.
- In testing out potentially implementable steps, simulation can help in the process of making decisions on the most efficient and cost effective models of work. Thus it contributes towards cost-savings.
- Simulation modelling can be a qualitative method to address underlying assumptions of a system wide process implementation, whilst at the same time, can facilitate the identification of barriers and enablers. This step can be crucial to decision making before the confirmed, finalised implementation. Barriers are challenges which can be encountered when planning and implementing transitional research findings, thus knowing and discovering them (especially latent ones) during simulation is very helpful.. Enablers and facilitators refer to persons, events, circumstances or experiences which assist or value add to the implementation.
- Simulation enables the creation of ‘visual prototyping’ of a system thus contributing towards validating systems behaviour and performance.
Translational simulation can be applied in skills translation, systems testing and systems integration. In other contexts, simulation exercises help in improvement of service delivery. Simulation is different from an experiment, which is fixed as a time-based evolution of a process but, it can be integrated into mathematical models to predict real-time performance and behaviour [22,27-29].
Call To Action: The Implementation Framework
In planning implementation, having a formal framework is beneficial. It should be reviewed from the beginning and customised to the appropriate local setting. Checklists can be utilised to translate the constructs and domains into actionable steps which can be easily executed. Otherwise, with the multitude of processes involved, it is not uncommon for shortcuts to be taken or for important elements to be overlooked. More often, after a smooth initiation, the implementation tend to drift into delays and uncertainties as the process unfolds [3,24]. This is where having champions and persons designated to look into and take ownership of certain domains play a crucial role to ensure non-regression of the implementation process. Assessing the effectiveness of the implementation is also important in order to ensure a sustainable programme, pathway or process [6,25,26,30].
One commonly used framework in Implementation science is The Consolidated Framework for Implementation Research (CFIR). CFIR helps to predict barriers and facilitators for implementation effectiveness. It can be customized to address contextual determinants, across implementation settings and locality. Since its original proposal, the CFIR has been through a few iterations and is known as the Updated CFIR [5,6].
The CFIR framework was recently used to implement an Emergency-Neonatal-Obstetric Code (ENOC) at Singapore General Hospital, which represents the clinical entity within the Academic Medical Centre (AMC of Sing health Duke NUS AMC. The ENOC will be activated for [31]:
- Any imminent delivery outside of the labour and obstetric wards
- Birth before arrival to the ED (emergency department)
- Maternal collapse
- Eclamptic seizures
- Cord Prolapse and
- Massive obstetric haemorrhage
It requires an inter-professional team response. Why the ENOC idea was conceived is due to the following reasons [29-31].
When there are maternal emergencies in the Emergency Department (ED), frontline emergency physicians will manage them and will contact the Obstetrics and Gynaecology (OG) on-call doctor. These maternal emergencies would include maternal cardiac arrest, eclamptic seizures, antenatal and postnatal (post-partum haemorrhage) and obstetric haemorrhage. At times, coupled with the maternal emergencies are also obstetric emergencies; such as shoulder dystocia, breech delivery, premature baby delivery and cord prolapse. For these, the Neonatology registrar and the anaesthetist on call would have to be contacted as well in view of the imminent high risk delivery of the baby and the potential need to use the emergency operating theatre (EOT) for surgical interventions. To call each of these doctors, it takes time. This also means the ED doctor would have to repeat the history several times [31].
The time taken for these personnel to arrive at the ED resuscitation room also varies due to a variety of factors, including how fast they can be activated by the ED staff. There have been challenges in the micro-system described. These could be related to time delays, human factors, equipment issues and lack of clear workflow processes. These delays can be linked to poor patient (maternal and baby) outcomes, low staff morale and inability to meet key performance indicators (KPIs). Feedback gathering from the ground staff was also conducted to see what inputs were of concern and also to get their ideas on how to better manage these issues [31-33].
As a result of this, it was decided that a review of the work flow processes was needed. This was conducted with an inter-professional team, from all the relevant disciplines (Emergency Medicine, Neonatology, Obstetrics and Gynaecology, Call Centre Operations). A simple, clear and effective workflow would be desirable. Every discipline must be clear about their roles, responsibilities and commitment as members of the team. From this review, a consolidated algorithm was generated based on the agreement and inputs from all disciplines. A simultaneous activation code makes more practical sense than the current sequential mode of calling each discipline. This flow was finalised after several rounds of brainstorming to ensure the needs and requests are met [31,34](Figure 2).
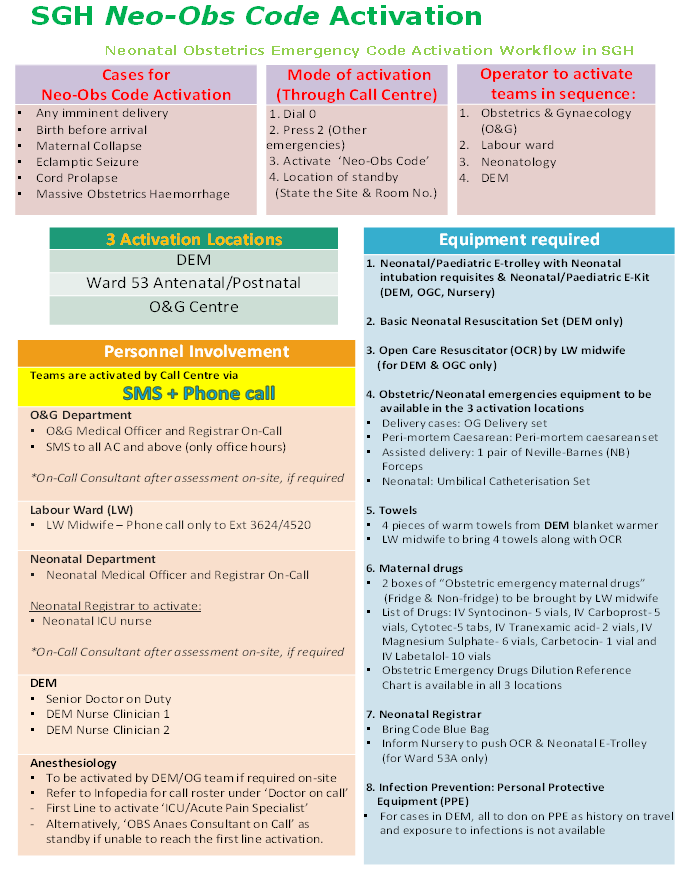
Figure 2. Neonatal obstetrics Emergency code Activation Work Flow in SGH.
The CFIR framework was very helpful in the planning stages of the implementation of ENOC. It helped us keep pace with our proposed steps and timeline and ensured no blind spots were overlooked in the build-up to implement the Code. It helped us realise that most implementation efforts actually tend to focus on staff training and less on building the implementation capacity, the implementation context and other important factors that can influence the programme success. Thus, we decided to focus on these and also planned in using in situ simulation to help achieve maximum impact, once implemented.
Table 1 provides the summary of the considerations given to the various constructs of the CFIR framework. Besides having this framework, the PDSA (Plan-Do-Study-Act) cycles were also very useful in our implementation of ENOC. In the process of implementation, in situ simulation was used on multiple occasions to test out the proposed flow, to study challenges, to pick up latent threats, to familiarise staff across the three departments with the pathway and to reinforce good practices. In situ simulation was repeatedly utilised during the one year of planning for the ENOC. It has certainly helped the team maximise the impact of their implementation process.
Table 1. Using the Updated Consolidated Framework for Implementation Research for The Emergency Neonatal Obstetric Code (ENOC) implementation.
|
|
CONSTRUCT |
DESCRIPTION |
|
1 |
Intervention |
|
|
a |
Intervention Source |
A new consolidated inter-professional algorithm developed internally and agreed upon by all the stakeholders/ disciplines (Emergency Medicine, Neonatology, Obstetrics and Gynaecology and Call Centre). Various rounds of fine-tuning, brain-storming and simulation-based testing was also conducted before final confirmation |
|
b |
Strength/ Quality of Evidence |
All disciplines involved agreed a change was needed and also a single code activation would serve the purpose and meet the objectives, instead of the current sequential activations which had to be carried out by the Emergency medicine staff. Literature search was also conducted to sort out the best evidence and similar studies from other centres. These corroborated our objectives and desired outcome for having our Emergency Neonatology-Obstetric Code (ENOC) |
|
c |
Relative advantage |
Before agreement, various ideas and methodologies were discussed. The mode of activation using a single Code through the call centre, “To Activate ENOC” was chosen over others such as using an institution wide announcement call or sequential, distributed calls. These other methods would increase time delays as well. |
|
d |
Adaptability |
Issues such as : i.Criteria for activation ii. Use of the Call Centre Code iii. Standardization of equipment across the Emergency Department, Neonatology and Labour Ward, were discussed. Site visits were conducted to understand equipment arrangements, layout and location, better. Staff across all the disciplines participated actively to ensure their level of comfort was met |
|
e |
Trialability |
This was conducted with the use of planned in situ simulation sessions to ensure all segments of the flow was seamless. This kind of testing is known as sequential simulation. Latent threats and hitches in the flow were corrected and changes incorporated into the final algorithm |
|
f |
Complexity |
As this pathway and workflow involves inter-professional staff across several departments (cross-departments), its scope and coverage is broader than just within one department. It also serves to align with all the domains of IPCP (inter-professional collaborative practice). The approval process within each department, right up to the institution level of The Medical Board’s approval must be obtained. One other initiative is the coordination with the existing Code Blue Response for the institution which responds to all cardiac arrest. For the ENOC, one of our focuses is on maternal cardiac arrest. Thus, how to coordinate between the two codes had to be clarified so staffs are clear about the activation. |
|
g |
Design Quality and Packaging |
From the criteria for activation, the work flow, the personnel involved, the evidence-based actions at each step, (which was trialled via simulation) to the evaluation and monitoring after implementation: all these have to be planned and packaged appropriately. The comprehensive package helps in the standardization during the sharing with the staff within each department and getting their concurrence and buy-in. Also the publicity that needs to be done in order to ensure all practitioners in the Academic Medical Centre (AMC) is aware of the pathway and will activate appropriately , must be given adequate time. |
|
h |
Cost |
The cost for starting up the ENOC flow is very reasonable. It does not involve entirely new equipment but more of the realignment and re-organization of flow. The call centre operators also saves in terms of having less calls to make with just one Code that activates all the relevant staff |
|
2 |
Outer Setting |
|
|
a |
Patient Needs and Resources |
Patients’ needs are crucial and central. In planning pathways and care delivery, they must be patient-centric and appropriately positioned in order to make the flow as seamless as possible for patients and their relatives/ families. Any barriers to these must be addressed. In fact, aligning with this, it becomes easier for the departments to also meet their key performance indicators (KPI) such as waiting time to care deliver, mortality and morbidity rates and other outcomes measures. Thus, there is value in this alignment. |
|
b |
Cosmopolitanism |
Our academic medical centre is world renown. This means all KPIs and outcomes indicators are shared and contribute towards both national and international data collation, such as the World Health Organization (WHO) ranking for maternal mortality and perinatal mortality rates(relevant to our implementation of ENOC) etc. |
|
c |
Peer Pressure |
Peer competition can be a healthy thing. However even without this we are always looking at our dynamic flow processes to see how change can be implemented and improvements can be integrated. This is the only way forward, inculcating a growth mindset amongst staff and at the same time, ensuring the organization progresses. |
|
d. |
External Policy and Incentives |
The ENOC is an internal pathway for our institution. However, through conference presentations and publications, we are happy to share with others, regionally and internationally. Within the institution itself, good programmes are highlighted and shared for collaborative best practice ideas and innovations. |
|
3 |
Inner Setting |
|
|
a |
Structural Characteristics |
The Sing Health Duke NUS AMC, where the clinical departments are under Singapore General Hospital (a healthcare institution providing clinical services for over 200 years), meets the criteria for age, maturity and size of organization |
|
b |
Networks and Communications |
As a large healthcare institution and cluster, there are formal and informal networks of communications established and in use. This makes it easier for proper dissemination and sharing as needed. Sharing through email blasts, information technology formal channels, intranet, departmental newsletters, peer review sessions and others, are all in place. |
|
c |
Culture |
The mission of the organization is
Our values and norms are summarised by SPREE (safety, professionalism, respect, experience and efficiency). Thus in all our work and outreach, these values are to be aligned with. |
|
d |
Implementation Climate |
|
|
|
Tension for Change |
As described in the text, flow processes are dynamic and staff champions recognise the need to change and upgrade from the current micro-system of function to a better and more seamless one ie to undertake the ENOC activation pathway |
|
|
Compatibility |
The objective of ENOC aligns with that of the institution, in terms of values, norms and goals. |
|
|
Relative Priority |
Individuals involved across the ED, OG, Neonatology departments recognise the importance and need for ENOC |
|
|
Organizational Incentives and Rewards |
These are not the primary drivers of instituting the implementation. However, if it does gain recognition or any award it is a bonus which should be viewed as a positive step in helping to create strategic publicity and knowledge of the implementation |
|
|
Goals and Feedback |
This is shared very closely with all staff of the respective departments involved. Even after implementation, every time the ENOC is activated, a form is completed for evaluative feedback and issues raised are ironed out. If changes are needed, these will be discussed for proper implementation. All these are done with the objective of wanting to continually improve performance |
|
|
Learning Climate |
In the implementation of ENOC, heads of department, champions, and staff, all work together and in the process, learning from each other is inevitable. Maintenance of psychological safety across all levels of staff is also a conscious effort on everyone’s part. The staffs are given leeway to implement new initiatives, which are evidence-based in order to improve processes. They are also given sufficient time for reflection, feedback and even site visits to familiarise themselves with equipment, flow and personnel involved. Tests and trials are conducted as deemed necessary to enhance the level of comfort |
|
e |
Readiness for Implementation |
The team in charge looked all aspects of the pathway before final implementation. Different options and ideas were discussed. Trials were done via in situ simulation in order to depict the actual state as to how the Code would run. Changes at every step were also added and shared appropriately. The finalised protocol was presented across all the 3 departments involved, before forwarding to the Medical Board of the institution, where the final approval for execution and implementation was obtained from the Chairman, Medical Board. Following this ENOC was also discussed with the Code Blue cardiac arrest response team of the institution in view that one category of overlap may occur, i.e. the group in cardiac arrest, whereby a maternal cardiac arrest may not be recognised as an ENOC activation but rather as a generic Code Blue activation. In the event this occurs, a parallel workflow for coordination between the two pathways was also planned and implemented. |
|
|
Leadership Engagement |
Leadership at all levels were involved as can be seen from the Readiness for Implementation section/ domain |
|
|
Access to Knowledge and Information |
The pathway was simplified and thus very easy to follow. It was uploaded on the departments website and institution intranet as resource and reference materials. |
|
4 |
Characteristics of Individuals |
|
|
a |
Knowledge/ belief on Interventions |
Individual knowledge is important but collaborative learning and sharing with colleagues and staff in the department is also very relevant. The peer sharing and explanation is very helpful to ensure common alignment and understanding by all staff that will be using / executing the pathway. |
|
b |
Self-efficacy |
With the peer review and sharing, individuals are able to assess their understanding and clear their doubts if any. Their buy-in is important as they will be the users of the ENOC. |
|
c |
Individual state of Change |
As above, all the relevant staff that is likely to be involved in the activation will be updated. This way they can assess their own capabilities and readiness to participate in the implementation. They are also invited to participate in the in situ simulation trainings. |
|
d |
Individual identification with organization |
All the staffs involved in ENOC are within different departments within the larger academic medical centre of Sing Health Duke NUS. Thus, values and norms are easier to align. |
|
e |
Personal Attributes |
The committee as well as the champions must bear in mind factors such as motivation levels of staff, capabilities, and their understanding, competence and learning styles. |
|
5 |
Process |
|
|
a |
Planning |
The ENOC was planned in a step by step organised fashion: from the conceptualization stage to the trials via in situ simulation, the final execution and implementation. Each step should be given adequate time to be developed and practised. |
|
b |
Engaging |
The importance of engaging all stakeholders cannot be over-emphasized. All the relevant individuals must be engaged with a common strategy, with education, and role modelling of their own roles as appropriate. |
|
|
Opinion leaders |
These persons who are leaders and in positions of influence are engaged. They can also be the champions or ambassadors of the initiative. For ENOC, all the heads of the various departments were involved. So were the Director of Quality and simulation champions of the departments |
|
|
Internal Implementation Leaders |
As above, the Opinion Leaders can also play the role of the implementation leaders. |
|
|
Champions |
These are the individual who are dedicated to support and help in the implementation of the initiatives. They will also usually help with answering any queries, sorting out challenges and overcoming any differences which may exist. |
|
|
External Change Agents |
Each of the departments here, (i.e. ED, OG and neonatology) contributed representatives to work collaboratively. They were the ambassadors or the external change agents. |
|
c |
Executing |
The role of executing is done by the appointed committee/persons and they are responsible to see the ENOC implemented to completion; to the stage when it becomes embedded into day to day use and is activated appropriately. |
|
d |
Reflecting and Evaluating |
In fact, after implementation, monitoring continues. Each time the ENOC is activated, feedback on any challenges and issues are gathered and evaluated. From here, any necessary changes are then evaluated for implementation. If new steps are introduced, then all stakeholders will have to be updated once more to ensure everyone is on the same page and alignment is most crucial here |
Hospitals represent complex systems, with macro- and micro-systems. It is important to ensure well-coordinated services as well as continuity of essential services as patients move from one area to the next within the institution. There must be swift adaptation to the changing needs. This is especially with critically ill patients, with time-dependent issues. Planning this simultaneous activation code took a year. All these steps are important to ensure proper activation, and quality improvement in the implemented intervention.
ENOC represents a major paradigm shift but a necessary one. Inter-professional team responses such as this must proceed in a coordinated and choreographed fashion to ensure efficiency and effectiveness in execution. IS supports innovative approaches as we identify, understand and overcome barriers to the adoption and integration of evidence-based interventions. In situ simulation has played a critical role in testing and trialling many of the steps in ENOC, before final implementation. The CFIR has been a useful framework to guide the work of planning, implementation and change adaptation.
REFERENCES
- Bernstein SL, Stony CM, Rothman RE. (2015). Dissemination and implementation research in emergency medicine. Acad Emerg Med. 22(2):229-236.
- Bauer MS, Damschroder L, Hagedorn H et al. (2015). An introduction to implementation science for the non-specialists. BMC Psychol. 391:32.
- Century J, Cassata A. (2016). Implementation research: finding common ground on what, how, why, where, who. Rev Res Educ. 40(1):169-215.
- Eccles MP, Mittman BS. (2006). Welcome to implementation science. Implement Sci. 1(1):1.
- Damschroder LJ, Aron DC, Keith RE et al. (2009). Fostering implementation of health sciences research fndings into practice: a consolidated framework for advancing implementation science. Implemnt Sci. 4(10):1-5.
- Damschroder LJ, Reardon CM, Marilla A, et al. (2022). The updated Consolidated Framework for Implementation Research based on feedback. Implement Sci. 17(1):75.
- Nilsen P. (2015). Making sense of implementation theories, models and frameworks. Implement Sci. 10(1):53.
- Lengnick-Hall R, Gerke DR, Proctor EK et al. (2022). 6 practical recommendations for improved implementation outcomes reporting. Implement Sci. 17(1):16.
- Fatimah L. (2010). Simulation-based learning: Just Like the Real Thing. J Emerg Trauma Shock. 3(4):348-352.
- Rosen KR. (2008). The history of medical simulation. J Crit Care. 23(2):157-166.
- Shapiro MJ, Morey JC, Small JD et al. (2004). Simulation-based teamwork training for ED staff: Does it improve clinical team performance when added to an existing didactic teamwork curriculum. Qual Saf Healthcare. 13(6):417-421.
- McGaghie WC, Issenberg SB, Petrosa ER et al. (2016). Revisiting a comprehensive review of simulation-based education research 2003-2009. Med Edu. 50(10):986-991.
- Durlak J, DuPr E. (2008). Implementation matters: a review of results on the influence of implementation on program outcomes and the factors affecting implementation. Am J Community Psychol. 41(3-4):327-350.
- Dubrowski R, Dubrowski A. (2018). Why should implementation science matter in simulation-based health professions education. Cureus. 10(12):e3754.
- Al-Azri NH. (2020). How to think like an emergency care provider: a conceptual mental model for decision making in emergency care. Edu Adv in Emerg Med. Int J of Emerg Med. 13(1):17.
- Bender GJ, Maryman JA. (2018). Clinical macrosystems simulation translates between organizations. Simul Healthc. 13(2):96-106.
- Brazil V, Purdy EI, Bajaj K. (2019). Connecting simulation and quality improvement: How can healthcare simulation really improve patient care? BMJ Qual Saf. 28(11):862-865.
- Lateef F. (2018). Inter-professional education, inter-professional practice and team science: learning together, working together. Edu Med Journal. 10(4): 81-91.
- Lateef F. (2018). Clinical reasoning: the core of medical education and practice. Int J Intern and Emerg Med. 1(2):1015.
- Moir T. (2018). Why is implementation science important for interventional design and evaluation within educational settings? Front Edu. 3: 61.
- Kilborne AM, Glasgow RE, Chambers DA. (2020). What can implementation science do for you? Key success stories from the field. J Gen Intern Med. 35:783-787.
- Fort DG, Herr TM, Shaw PL et al. (2017). Mappng the evolving definition of translational research. J Clin and Translational SCi. 1(1):60-66.
- Lamé G, Dixon-Woods M. (2020). Using clinical simulation to study how to improve quality and safety in healthcare. BMJ Simul Technol Enhanc Learn. 6(2):87-94.
- Baumann AA, Cabassa LJ. (2020). Reframing implementation science to address inequities in healthcare delivery. BMC Health Serv Res. 20(1):190.
- Wensing M. (2021). Reflection in the measurement of implementation constructs. Impement Res Pract. 2:263348952110201.
- Dy SM, Ashok M, Wines RL et al. (2015). A framework to guide implementation research for core transition intervention. J Healthcare Qual. 37(1):41-54.
- Brazil V. (2017). Translational simulation: Not where but why? A functional view of insitu simulation. Adv in Sim. 2(1):1-5.
- Chan SL, Lee JW, Ong EHM et al. (2022). Implementation of prediction models in the emergency department from an implementation science perspective: determinants, outcomes and real world impact: a scoping review protocol. PLoS One. 17(5):e0267965
- Murphy M, Curtis K, McCloughen A. (2019). Facilitators and barriers to the clinical application of teamwork skills taught in a multidisciplinary simulated trauma teams training. Injury. 50(5):147-152
- Kristensen N, Nymann C, Konradsen H. (2016). Implementing research results in clinical practice: the experience of healthcare professionals. BMC health Services Res. 16(10):1-11.
- Lateef F. (2020). It Just takes One Phone call: Simultaneous activations to reduce referral times. Clinical Orthopaedic and Trauma Care. 2(2):029.
- Jeejeebhoy FM, Zelop CM, Lipman S, Carvalho B, Joglar J, Mhyre J et al. (2015). Cardiac arrest in pregnancy. A scientific statement from the American Heart Association. Circulation. 132(18):1747-1773.
- Winters B, Pham J, Pronovost P. (2006). Rapid response teams walk. Don’t run. JAMA. 296(13):1645-1647.
- King E, Wowath R, Shulken DJ. (2006). Establishing a rapid response team in an academic hospital: One years experience. J Hosp Med. 1(50):296-305.