Information Links
Related Conferences
Previous Issues Volume 7, Issue 1 - 2022
Healthcare Documents: How Readable? A Study of Simple Strategies to Decrease Reading Grade Level and Increase Reading Ease of Healthcare Documents
James Espinosa*, Alan Lucerna, Henry Schuitema
Department of Emergency Medicine, Rowan University, USA
Received Date: June 19, 2022
Published Date: July 15, 2022
*Corresponding author: James Espinosa Department of Emergency Medicine, Rowan University SOM/Jefferson - Stratford, NJ, USA, 18 East Laurel Road, Stratford, NJ 08084, Tel: 8563045101 E-mail: [email protected]
Citation: Espinosa J, Lucerna A, Schuitema H. (2022). Healthcare Documents: How Readable? A Study of Simple Strategies to Decrease Reading Grade Level and Increase Reading Ease of Healthcare Documents. Mathews J Emergency Med. 7(1):44.
Copyright: Espinosa J, et al. © (2022).
ABSTRACT
Background: The field of healthcare is becoming more aware of the need for patients to be able understand the consent forms we provide. Health literacy is often defined as the ability to read, understand, and act correctly on health information. Health literacy surveys have consistently shown that about 24% of the population cannot read at the 5th grade level. About 66% of the population can read at the 6th grade level. It is for this reason that the target grade level for most newspapers and lay periodicals is set at a goal of a 6th grade reading level. [1-2] How can one study the reading level and reading ease of a document? A well-known formula for determining the reading grade level of a document is the Flesch-Kincaid Grade Score (FKGS). The Flesch Reading Ease Score (FRES) is a well-known formula for determining reading ease. One advantage of these two tests is that they are both available on a widely-available word processing platform. Methods: The purpose of this project was to identify a random sample of consent forms, open source, from the internet. The Flesch-Kincaid Grade Level and Flesch Reading Ease tests were applied to the random sample. Then two simple strategies were tested—reduction in sentence length and reduction of multi-syllable words. Sentence length was tested in isolation as well as in tandem with reduction of multi-syllable words. Results: All of the documents in the sample frame were at or above the FKGS of 8th grade reading level. The minimum FKGS grade level was 8. The maximum FKGS grade level was 21. The median FKGS was 11. The mean FKGS was 12.05. The overall paragraph sample Flesch Reading Ease Score (FRES) was 40.6% (Minimum 15, maximum 60, median 40). The sentence length intervention and sentence/syllable intervention both showed the effect of decreasing the reading grade level as expressed in the FKGS and of increasing reading ease as expressed in the FRES. These effects were highly statistically significant. The effects were incremental stepwise—sentence length intervention with word length reduction was statistically significantly lower in grade level and higher in reading ease than sentence length reduction alone. Conclusions: The sentence length intervention and sentence/syllable intervention both showed the effect of decreasing the reading grade level as expressed in the FKGS and of increasing reading ease as expressed in the FRES. These effects were highly statistically significant. Future directions could include a study of other literacy indicators. Hospital-based documents could be assessed for possible literacy intervention. Comparisons of reductions in FKGS and FRES could be compared to outcomes in other reading scores. Lastly, outcomes of patient comprehension pre and post literacy interventions, such as reductions in FKGS and increases in FRES, could be made.
Keywords: Healthcare Literacy, Consent Forms in Healthcare, Readability of Consent Forms
INTRODUCTION
The field of healthcare is becoming more aware of the need for patients to be able understand the written forms we provide in order to make informed decisions. Health literacy is often defined as the ability to read, understand, and act correctly on health information. 54% of adults have a literacy below 6th grade level. The average American reads at the 7th- to 8th-grade level. It is for this reason that the target grade level for most newspapers and lay periodicals is set at a goal of a 6th grade reading level. Medical information is ideally set at no greater than the 8th grade level. [1-12]
How can one study the reading level and reading ease of a document? There are hundreds of readability formulas. A well-known formula for determining the reading grade level of a document is the Flesch-Kincaid Grade Score (FKGS). An associated and related formula is the Flesch Reading Ease Score. (FRES). One advantage of these two tests is that they are available on Microsoft Word. [1 Microsoft Way, Redmond, WA 98052]
The purpose of this project was to identify a random sample of consent forms, open source, from the internet. The Flesch-Kincaid Grade Level and Flesch Reading Ease tests were applied to the sample frame. Then two simple strategies were tested—reduction in sentence length and reduction of multi-syllable words. Sentence length was tested in isolation as well as in tandem with reduction of multi-syllable words. These strategies were selected because they are integral to the Grade Level and Reading Ease analysis process. The FKGS is driven mathematically by average sentence length and the average number of syllables per word, and is based on research in readability. Flesch Reading Ease rates text on a 100-point scale. A higher score is related to higher readability. FKGL is driven by average sentence length as well as the average number of syllables per word and is based on research in readability.
MATERIALS AND METHODS
Objective 1: to identify a sample frame of 10 randomly selected consent forms from a frame of 30 consent forms identified on an internet search for healthcare consent forms. Thus, the analysis was performed on Internet-available, open-access documents.
Objective 2: To apply the Flesch-Kincaid Grade Level and Flesch Reading Ease tests to the sample frame
Phase1: A sample frame of 10 Internet-available, open-access documents was randomly selected from a frame of 30 internet-available open access documents. These documents were healthcare related, informed consent documents.
Phase 2: Flesch-Kincaid Grade Level and Flesch Reading Ease tests were applied to the sample frame.
Phase 3: Using a random number generator, a set of 10 paragraphs for testing was pulled from the sample frame. (one paragraph per document).
Phase 4: The effect on grade level and reading ease using two simple strategies was tested (reduction of sentence length versus reduction of sentence length and reduction of multi-syllable words)
Paired T-tests were used to study the relationship of the sample paragraphs to the entire source document, and to study the effect of sentence length reduction and sentence length with multi-syllable word reduction on the sample paragraphs.
RESULTS
The 10 complete documents in the internet-search frame showed a mean Flesch Reading Grade Score (FKGS) of 13.6. The 10 sample paragraphs showed a mean FKGS of 12.05.
The difference between the total consent documents and the samples from the consent documents was not statistically significant. All of the documents in the sample frame were at or above the FKGS of 8th grade reading level. The minimum FKGS grade level was 8. The maximum FKGS grade level was 21. The median FKGS was 11.
The overall paragraph sample Flesch Reading Ease Score (FRES) was 40.6%. (Minimum 15, maximum 60, median 40) The mean FRES from the entire consents was 42. The difference between the FRES from the full consents and the sample paragraphs was not statistically different. All of the documents in the pretreatment sample frame showed a reading ease (FRES) of 60 or below.
Effect of Sentence length intervention alone:
Sentence length intervention alone reduced the FKGS Grade level from a sample pre-intervention mean of 12.05 to a sentence length intervention mean of 8.86. (p<0.006, paired T-test) Sentence length intervention alone increased the FRES (reading ease score) from a sample pre-intervention mean of 40 to a sentence length intervention mean of 52.2 (p<0.002, paired T-test)
Effect of Sentence length intervention and word syllable reduction:
Sentence length intervention with syllable reduction reduced the FKGS Grade level from a sample pre-intervention mean of 12.05 to a sentence length/syllable reduction intervention mean of 8.13. (p<0.004, paired T-test) Sentence length intervention with syllable reduction increased the FRES (reading ease score) from a sample pre-intervention mean of 40 to a sentence length/syllable reduction intervention mean of 55 (p<0.001, paired T-test)
The difference between sentence length intervention alone and sentence length word syllable reduction on FKGS:
The difference between sentence length (mean 8.86) and sentence length/word syllable reduction (8.130) on the FKGS was statistically significant. (p<0.006, paired T-test)
The difference between sentence length intervention alone and sentence length/word syllable reduction on FRES:
The difference between sentence length (52.2) and sentence length/word syllable reduction (55.3) on the FRES was statistically significant. (p-0.006, paired T-test)
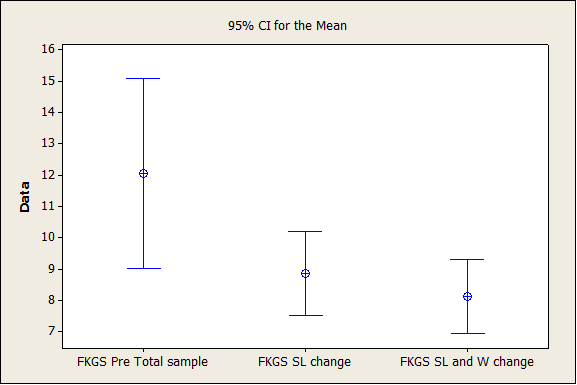
Figure 1: Interval Plot Grade Level (FKGS): pretreatment, sentence length change (SL) and sentence length/word complexity change (SL and W).
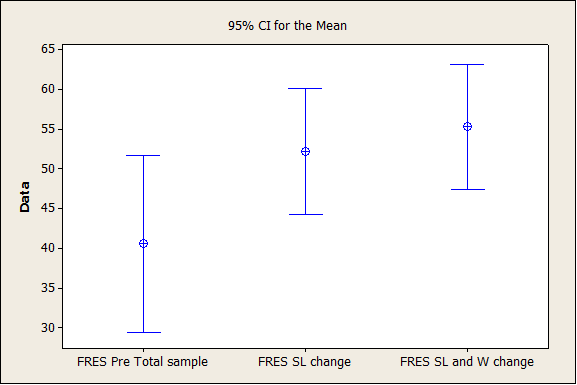
Figure 2: Interval Plot Reading Ease (FRES): pretreatment, sentence length change (SL) and sentence length/word complexity change (SL and W).
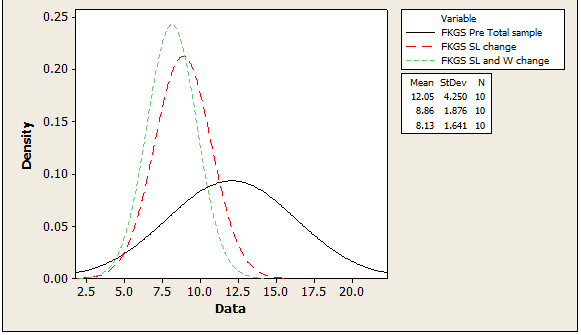
Figure 3: Histogram. Flesh-Kincaid Grade Score total sample, then after sentence length change alone, then after sentence length and word complexity (SL and W) reduction change.
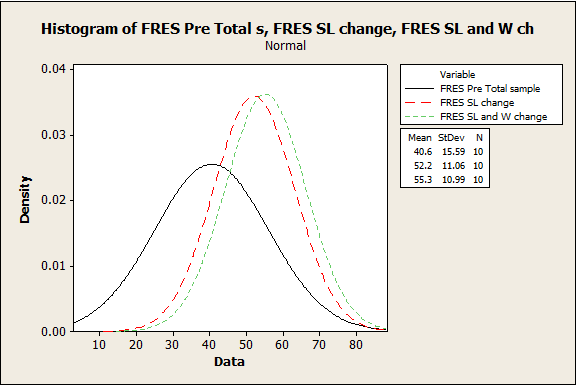
Figure 4: Histogram. Flesch Reading Ease Score: total sample, then after sentence length change alone, then after sentence length and word complexity (SL and W) reduction change.
DISCUSSION
The growing demand on healthcare professionals is vast and the population that care is provided for is always highly variable. Health literacy is one such variable that is pivotal and is often forgotten. Lack of healthcare literacy not only affects patient autonomy but it has also been directly correlated to higher healthcare costs. This pilot study uses the FKGS and FRES scoring systems to analyze the average grade level and average reading ease of open source medical consent forms. Reducing sentence length and the number of syllable used were that two interventions performed to improve readability of the sample documents.
All of the documents in the sample frame were at or above the FKGS of 8th grade reading level. The minimum FKGS grade level was 8. The maximum FKGS grade level was 21. The median FKGS was 11. The mean FKGS was 12.05.
The overall paragraph sample Flesch Reading Ease Score (FRES) was 40.6%. (Minimum 15, maximum 60, median 40)
The FKGS and the FRES suggest that improvement would be desirable on the sample frame in order to decrease the average grade level and to improve the average reading ease.
The sentence length intervention and sentence/syllable intervention both showed the effect of decreasing the reading Grade level as expressed in the FKGS and of increasing reading ease as expressed in the FRES. These effects were highly statistically significant. The effects were incremental stepwise—sentence length intervention with word length reduction was statistically significantly lower in grade level and higher in reading ease than sentence length reduction alone.
Future directions could include a study of other literacy indicators. Hospital based documents could be assessed for possible literacy intervention.
Comparisons of reductions in FKGS and FRES could be compared to outcomes in other reading scores. Lastly, outcomes of patient comprehension pre and post literacy interventions, such as reductions in FKGS and increases in FRES, could be made.
CONCLUSIONS
The sample frame did not differ from the total consent frame, which suggests that the sampling method was valid. All of the documents in the sample frame were at or above the FKGS of 8th grade reading level. The minimum FKGS grade level was 8. The maximum FKGS grade level was 21. The median FKGS was 11. The mean FKGS was 12.05.The overall paragraph sample Flesch Reading Ease Score (FRES) was 40.6%. (Minimum 15, maximum 60, median 40) The FKGS and the FRES suggest that improvement would be desirable on the sample frame in order to decrease the average grade level and to improve the average reading ease. The sentence length intervention and sentence/syllable intervention both showed the effect of decreasing the reading Grade level as expressed in the FKGS and of increasing reading ease as expressed in the FRES. These effects were highly statistically significant. The effects were incremental stepwise—sentence length intervention with word length reduction was statistically significantly lower in grade level and higher in reading ease than sentence length reduction alone. Future directions could include a study of other literacy indicators. Hospital based documents could be assessed for possible literacy intervention. Comparisons of reductions in FKGS and FRES could be compared to outcomes in other reading scores. Lastly, outcomes of patient comprehension pre and post literacy interventions, such as reductions in FKGS and increases in FRES, could be made.
REFERENCES
- Adult Literacy Facts. ProLiteracy. http://www.proliteracy.org/the-crisis/adult-literacy-facts
- The U.S. Illiteracy Rate Hasn't Changed In 10 Years. (2013). HUFFPOST. http://www.huffingtonpost.com/2013/09/06/illiteracy-rate_n_3880355.html
- Williams MV, Parker RM, Baker DW, Parikh NS, Pitkin K, et al. (1995). Inadequate functional health literacy among patients at two public hospitals. JAMA. 274(21):1677-1682.
- US Department of Health and Human Services. (2010). National Institutes of Health Clear communication: an NIH health literacy initiative. Bethesda, MD: National Institutes of Health.
- Brown MT and JK Bussell. Medication Adherence: WHO Cares?” Mayo Clinic Proceedings. (2011). 86(4):304-314.
- Szabó P, Bíró É, Kósa K. (2021) Readability and Comprehension of Printed Patient Education Materials. Front Public Health. 9:725840.
- van Ballegooie C, Hoang P. (2021). Assessment of the Readability of Online Patient Education Material from Major Geriatric Associations. J Am Geriatr Soc. 69(4):1051-1056.
- Kapoor K, George P, Evans MC, Miller WJ and Liu SS. (2017) Health Literacy: Readability of ACC/AHA Online Patient Education Material. Cardiology. 138(1):36-40.
- Adult Literacy in the United States. (2019). National Center for Education Statistics. https://nces.ed.gov/pubs2019/2019179/index.asp
- Adult Literacy in the United States. (2019). Data Point: Adult Literacy in the United States. https://nces.ed.gov/pubs2019/2019179.pdf
- Palumbo R. (2017). Examining the impacts of health literacy on healthcare costs. An evidence synthesis. Health Serv Manage Res. 30(4):197-212.
- Wolf MS, Wilson EA, Rapp DN, Waite KR, Bocchini MV, et al. (2009). Literacy and learning in health care. Pediatrics. 124(0-3):S275–S281.