Previous Issues Volume 1, Issue 1 - 2018
Fulminant Hypoxic Hepatitis During Endurance Sport
Salem Bouomrani*,1,2, Nesrine Belgacem1, Maher Béji1,3
1Department of Internal medicine, Military Hospital of Gabes, Gabes 6000, Tunisia . 2Sfax Faculty of Medicine, University of Sfax, Sfax 3029, Tunisia. 3Tunis Faculty of Medicine, Tunis El Manar University, Tunis 1007, Tunisia.
Corresponding Author: Salem Bouomrani, Department of Internal medicine, Military Hospital of Gabes. Gabes 6000. Tunisia, Tel: +00216 98977555; Email: [email protected]
ABSTRACT
Introduction: Digestive complications are seen in 30% of endurance sports practitioners. They are dominated by gastric and intestinal lesions. Liver manifestations are much rarer and often unknown. Severe acute hepatitis complicating malignant hyperthermia of effort is the most serious form: fatal in 10% of cases. We report an observation. Case report: A 40-year-old patient, without pathological medical history, was hospitalized for a sudden loss of consciousness, confusion, and agitation with abundant liquid diarrhea and bilious vomiting, occurring at 19km from a race of a halfmarathon. The initial physical examination noted a fever at 38°C, systolic blood pressure at 90mmHg, and right hemiparesis. Biology showed leukocytosis at 11300/mm³, thrombocytopenia at 74000/mm³ and prothrombin time at 56%. An adapted resuscitation allowed the stabilization of the blood pressure and the regression of the neurological signs. On the second day, mucocutaneous jaundice with hepatic cytolysis at 10N for AST and 6N for ALT and a collapse of PT at 10%, as well as rhabdomyolysis (CPK at 46N and LDH at 8N) without renal failure.
The infectious, immunological, and morphological investigations of this hepatitis were negative. The diagnosis was that of fulminant hepatitis and subclinical rhabdomyolysis caused by exertional heatstroke. The subsequent course was progressively favorable after adequate resuscitation, infusion of fresh frozen plasma and vitamin K injection. The PT normalized on day 20 and cytolysis on day 40 and the patient had no physical sequelae. Conclusion: As rare as it is, the acute hepatitis of effort must be known and systematically evoked in front of any severe clinical presentation in high-athlete in order to ensure adequate and fast management making it possible to improve the prognosis of this affection.
KEYWORDS: Hypoxic Hepatitis; Exertional Heatstroke; Fulminant Hepatitis; Endurance Sport; Semi-Marathon.
INTRODUCTION The half-marathon (road running event of 21,097 kilometers) is a very popular sport for both athletes and amateurs for two reasons: 1) It does not require, in comparison with the marathon, a serious and advanced preparation, 2) The complications and the impact are less compared to the marathon: the half-marathon runs very much below the maximum aerobic speed and below the anaerobic threshold. Thus, there will be no shortness of breath or muscle fatigue; and muscle accumulation of lactates is lower. Pathophysiologically this is explained by the fact that the “30-kilometer wall” caused by the depletion of the glycogen stock does not occur in the halfmarathon [1-4]. This sport has become very popular because of its health benefits with mainly a reduction in cardiovascular events and general mortality [5]. Despite their health benefits, endurance sports can, on the other hand, have a negative and sometimes serious impact that can lead to severe functional and/or organic failures (heart, liver, kidneys ...) [1, 2, 6-8]. The digestive tract is one of the key systems that controls and regulates adaptation and regeneration of the athlete [9] explaining the frequency of digestive manifestations during endurance sports; it is estimated that 20 to 50% of athletes are having gastrointestinal symptoms [9-11]. These symptoms are one and a half time to three times more common among elite athletes than among occasional practitioners [10]. Unlike the digestive tract, the liver, located downstream of the splanchnic circulation, is considered a relatively “protected” organ during physical exertion [1, 2, 6, 8]. Its afferent vascularization is ensured by a double systemic and portal network; whose basal rest rate is estimated to be between 1.5 and 1.8L per minute. During exercise, the decrease in splanchnic flow causes a decrease in hepatic flow. The decrease in hepatic blood volume thus varied from 14 to 18% [2]; which made it the most vascularized organ of the abdominal cavity [1, 2, 6]. Thus, the liver remains an organ much more rarely affected than the rest of the digestive tract [1, 2, 6], and hepatic biological disturbances induced by endurance sports are still little known and little considered by clinicians: most often a rough clinical expression and biochemical translation often delayed from a few hours to a few days [1, 2, 6, 12]. Severe hepatic complications remain exceptional and unusual. Despite its potential severity and its possible fatal outcome, the isolated hepatic involvement during endurance sports, is little known, extremely reported as sporadic cases, poorly studied, and little characterized in current medical practice. We are reporting an original observation of an isolated fulminant hypoxic hepatitis complicating a half marathon in healthy adult. CASE REPORT
A 40-year-old man, with no pathological medical history, an active military, with a regular physical activity deemed average (regular training of 4 to 6 hours per week), participated in a programmed half-marathon. His clinical examination and basic biological tests before the race were without any abnormalities. He was well acclimatized since he was from and resides in the city where the race took place. After 19 km of running, he presented brutally a liquid diarrhea with fever at 38°C, systolic blood pressure at 90 mmHg, and right hemiparesis. Biology showed leukocytosis at 11300/mm³ with 70% neutrophils, thrombocytopenia at 74000/mm³, hepatic cytolysis at 10N for AST and 6N for ALT, and PT at 56%. His electrocardiogram, chest X-ray, and brain CT showed no abnormalities. Appropriate resuscitation had allowed the stabilization of blood pressure and the regression of neurological signs. On the second day a mucocutaneous jaundice was established with a worsening of hepatic cytolysis at 39N for AST and 65N for ALT, a cholestasis with total Bilirubin at 180μmol/l and direct Bilirubin at 98μmol/l, and a collapse of PT at 10%, as well as rhabdomyolysis (CPK at 46N and LDH at 8N) without renal failure. The patient was transferred to the intensive care unit. A progressive and adapted rehydration with hydroelectrolitic equilibration, transfusion of ten fresh frozen plasma bags, injection of vitamin K, and monitoring of vital parameters. Subsequent investigations aimed for the etiological diagnosis of this acute hepatopathy had not revealed any abnormalities: abdominal ultrasound and CT-scan, Doppler examination of intra-abdominal vessels, gastrointestinal fibroscopy, cerebral CT-scan and lumbar puncture, blood cultures, cardiac ultrasonography and viral serologies (hepatitis B, C, A and E, HIV, CMV, EBV and leptospirosis). There was no mention of medication, doping or potentially toxic substances or alcohol consumption. The evolution was progressively favorable with normalization of PT and blood count at day 20 and transaminases level at day 40. The patient had no physical sequelae. Table 1 summarizes the chronological evolution of the different biological parameters of our patient.
Table 1: Chronological evolution of the different biological parameters of our patient.
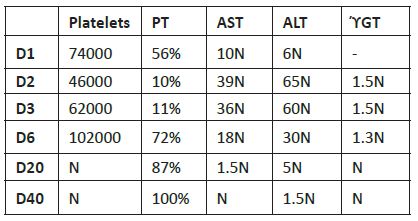
D: Day, AST: aspartate aminotransferase, ALT: alanine aminotransferase, PT: prothrombin time, ϓGT: gamma-glutamyltransferase.
DISCUSSION
It is known that intense and long physical exercise, especially marathon and half-marathon races, leads to a significant increase in all liver bioassays (AST, ALT, direct Bilirubin, total Bilirubin, ϓGT, and alkaline phosphatase) without exceeding the upper limits of normal rates [1,2,6,12,13]. The increase in transaminases is due essentially to muscle lysis, whereas hepatic damage is usually only secondary and minimal [14]. The predominance of ALT elevation and the association of hypertransaminasemia with even minimal cholestasis or hepatocellular insufficiency confirms the hepatic origin of these enzymatic abnormalities [7,15-18]. Apart from any underlying liver injury, bilirubin can be increased due to the continuous hemolysis typical of intense and prolonged exercise [7]. This cytolysis predominates on AST in the series of De Paz JA. and Nuviala RJ.; this is mainly related to rhabdomyolysis given the severity of the physical exercise (marathon and a 100 km run) [16,17]. Liver injury itself is constant in exercise hyperthermia or “ exertional heatstroke “ [19-21]. This involvement is reflected in 90% of cases by moderate, transient and subclinical cytolysis; [1,2,6]. In 10% of cases it is severe resulting in acute liver failure, fatal in half of the cases [1,19,20]. This hepatitis can sometimes be fulminant and require urgent liver transplantation [1,15,19,22,23]. Histologically; hepatocyte destruction is observed in the form of necrosis with intracytoplasmic vacuolization, the centrilobular localization of which supported an ischemic mechanism [2]. In mild forms, hepatic bioassays are elevated immediately after stroke and remain so for the next 24 hours except for ϓGT, which begins to decrease from the sixth hour after the end of exercise [12]. A return to normal is generally observed after two days [13]. The pathophysiology of liver injury in endurance sports involves hypoxia/relative tissue ischemia secondary to reduced splanchnic flow, excess production of free radicals and oxidative stress, and mitochondrial dysfunction induced by effort [24-26]. All of these factors lead to damage and lysis of hepatocytes more or less pronounced depending on the nature and duration of the effort, which can in extreme cases lead to shock liver or classic “hypoxic hepatitis” that remains exceptional [24,26-29]. Hepato-digestive disorders caused by endurance sports are mainly conditioned by the nature, duration and intensity of physical exercise [1,2,6,23]; many other factors influence the onset and degree of these disorders such as: age, sex, state of hydration, level of training and acclimation, drug and food intake and possible underlying diseases: these disorders appear to be more frequent in young, female athletes, poorly hydrated, poorly trained, badly acclimated, and those with pre-existing liver disease and/or taking potentially toxic substances for the liver and the gastrointestinal tract (anti-inflammatory drugs, anabolic steroids,...) [1,3,29]. Inherited determinants, particularly muscular enzymatic equipment, are also incriminated [7,30]. All of these findings mean that clinical signs and variations in liver bioassays must be taken into consideration when selecting and preparing candidates for high level competitions [12,13]; and by analogy when selecting military soldiers for special missions requiring intense and/or prolonged physical effort. The recommendations for avoiding or minimizing the hepatic and gastrointestinal repercussions of endurance sports are regular training, changes in lifestyle, adapted diet composition, adequate hydration and the eviction of any doping product [1,6,10,31,32]. Subsequent large-scale studies, systematically analyzing clinical manifestations and biological abnormalities, are thus useful for better understanding and characterizing hepatic complications during endurance sports.
CONCLUSION
As rare as it is, the acute hepatitis caused by exertional heatstroke must be known and systematically evoked in front of any severe clinical presentation in athletes. A better knowledge of this exceptional, but potentially fatal, complication of the intense sport activity makes it possible to establish the diagnosis without delay and to ensure an adequate and fast care, thus making it possible to improve its prognosis. Certain recommendations are to be respected as well by the candidates participating in endurance sports activities as by the sports doctors taking care of these candidates to avoid or minimize the liver injury. Good physical preparation with regular training and good acclimation, a balanced diet, good continuous hydration during the race, as well as the eviction of alcohol, hepatotoxic drugs, and any doping substance are recommended. CONFLICTS OF INTEREST
None
ABBREVIATIONS
AST: aspartate aminotransferase, ALT: alanine aminotransferase, CMV: cytomegalovirus, CT: computed tomography, CPK: creatine phosphokinase, EBV: Epstein-Barr virus, ϓGT: gamma-glutamyltransferase, HIV: human immunodeficiency virus, LDH: Lactate dehydrogenase, PT: prothrombin time. REFERENCES 1. Watelet J and Bigard MA. (2005). Troubles hépato-digestifs du sportif. Gastroenterol Clin Biol. 29(5): 522-532. 2. Watelet J. (2008). Foie et sport. Gastroenterol Clin Biol. 32(11): 960-972. 3. Villiger B, Egger K and Lerch R. (1992). Endurance, theory and practice. Masson, Paris. 1-259. 4. Lopez AA, JP Preziosi, Chateau PH, Auguste PH, et al. (1994). Digestive disorders in competition among endurance athletes: epidemiological survey on a triathlon sports season. Gastroenterol Clin Biol. 18 (4): 317-322. 5. Grosclaude M and Ziltener JL. (2010). Les avantages de l’activité physique (et / ou les effets néfastes d’un mode de vie sédentaire). Rev Med Suisse. 6: 1495-1498. 6. Watelet J and Bronowicki JP. (2005). Hepatogastroenterological pathology of the sportsman. EMC - Hepato-Gastroenterology. 2 (1): 1-11. 7. Banfi G, Colombini A, Lombardi G and Lubkowska A. (2012). Metabolic markers in sports medicine. Adv Clin Chem. 56: 1-54. 8. Bouomrani S, Baïli H, Allani R and Béji M. (2015). Manifestations hépato-digestives et sport d’endurance chez les militaires. J Afr Hépatol Gastroentérol. 9(4): 170-178. 9. Berg A, Müller HM, Rathmann S and Deibert P. (1999). The gastrointestinal system--an essential target organ of the athlete’s health and physical performance. Exerc Immunol Rev. 5: 78-95. 10. De Oliveira EP and Burini RC. (2009). The impact of physical exercise on the gastrointestinal tract. Curr Opin Clin Nutr Metab Care. 12(5): 533-538. 11. Peters HP, De Vries WR, Vanberge-Henegouwen GP and Akkermans LM. (2001). Potential benefits and hazards of physical activity and exercise on the gastrointestinal tract. Gut. 48(3): 435-439. 12. Lippi G, Schena F, Montagnana M, Salvagno GL, et al. (2011). Significant variation of traditional markers of liver injury after a half marathon run. Eur J Intern Med. 22(5): e36-e38. 13. Wu HJ, Chen KT, Shee BW, Chang HC, et al. (2004). Effects of 24 h ultra-marathon on biochemical and hematological parameters. World J Gastroenterol. 10(18): 2711-2714. 14. Bessa A, Nissenbaum M, Monteiro A, Gandra PG, et al. (2008). High-intensity ultraendurance promotes early release of muscle injury markers. Br J Sports. Med 42(11): 889-893. 15. Barjonet G, Lenz AB and Gatfosse M. (1992). Foie hypoxique d’effort : une entité à ne pas méconnaitre. Cinésiologie. 32: 235-237. 16. De Paz JA, Villa JG, Lopez P and Gonzalez-Gallego J. (1995). Effects of long-distance running on serum bilirubin. Med Sci Sports Exerc. 27(12): 1590-1594. 17. Nuviala RJ, Roda L, Lapieza MG, Boned B, et al. (1992). Serum enzymes activities at rest and after a marathon race. J Sports Med Phys Fitness. 32(2): 180-186. 18. Priest JB, Oei TO and Moorehead WR. (1982). Exercise-induced changes in common laboratory tests. Am J Clin Pathol. 77(3): 285-289. 19. Tortosa JC, Mahe V and Ichai P. (1999). Exercise heat stroke and acute liver failure. Urgent Rescue. 8 (5): 363- 367. 20. Valla DC. (2003). Acute hepatic hypoxia, congestive heart liver. Gastroenterol Clin Biol 27 (Suppl 5): B33-B40. 21. Hassanein T, Razack A, Gavaler JS, Van Thiel DH, et al. (1992). Heatstroke: its clinical and pathological presentation, with particular attention to the liver. Am J Gastroenterol. 87 (10): 1382-1389. 22. Saïssy JM, Almanza L, Samuel D and Pats B. (1996). Hepatic transplantation after exercise heat stroke with fulminant liver failure. Press Med. 25 (21): 977-979. 23. Saïssy JM. (2000). Heat stroke. Urgent Rescue. 9 (7): 498- 507. 24. Bing Y and Zhaobao W. (2010). Effects of Ginkgo biloba extract on free radical metabolism of liver in mice during endurance exercise. Afr J Tradit Complement Altern Med. 7(4): 291-295. 25. Benderitter M, Hadj-Saad F, Lhuissier M, Maupoil V, et al. (1996). Effects of exhaustive exercise and vitamin b6 deficiency on free radical oxidative process in male trained rats. Free Radical Biol Med. 21(4): 541-549. 26. Sun L, Shen W, Liu Z, Guan S, et al. (2010). Endurance exercise causes mitochondrial and oxidative stress in rat liver: effects of a combination of mitochondrial targeting nutrients. Life Sci. 86(1-2): 39-44. 27. Voces J, Alvarez AI, Vila L, Ferrando A, et al. (1999). Effects of administration of the standardized Panax ginseng extract G115 on hepatic antioxidant function after exhaustive exercise. Comp Biochem Physiol Part C: Pharmacol, Toxicol Endocrinol. 123(2): 175-184. 28. Gul M, Demircan B, Taysi S, Oztasan N, et al. (2006). Effects of endurance training and acute exhaustive exercise on antioxidant defense mechanisms in rat heart. Comp Biochem Physiol - Part A: Mol & Integrative Physiol. 143(2): 239-245. 29. Hartgens F and Kuipers H. (2004). Effects of androgenicanabolic steroids in athletes. Sports Med. 34(8): 513-554. 30. Costa AM, Breitenfeld L, Silva AJ, Pereira A, et al. (2012). Genetic inheritance effects on endurance and muscle strength: an update. Sports Med. 42(6): 449-458. 31. Saris WH, Brouns F, Beckers EJ and Rehrer NJ. (1992). The effect of beverage composition and gastrointestinal function on fluid and nutrient availability during physical exertion: e review. Schweiz Z Sportmed. 40(4): 149-160. 32. Maughan RJ and Shirreffs SM. (2012). Nutrition for sports performance: issues and opportunities. Proc Nutr Soc. 71(1): 112-119.