Previous Issues Volume 1, Issue 2 - 2016
Fever and its Association with Infection in Severely Injured Polytrauma Patients
Sylvain Steinmetz1, Ilker Uçkay1,2, Corinne Cohen3, Sophie Abrassart1
1Orthopedic Surgery Service, Switzerland.
2Service of Infectious Diseases, Geneva University Hospitals & Medical School, University of Geneva, Geneva, Switzerland.
3Emergency Medicine Service, Sion Hospital, Sion, Switzerland.
Corresponding Author: Ilker Uçkay, University Hospitals of Geneva and Faculty of Medicine, 4rue Gabrielle Perret-Gentil, 1211 Geneva 14 / Switzerland, Tel: ++41 22 372 9828; E-Mail: [email protected]
Received Date: 26 Oct 2016 Accepted Date: 01 Dec 2016 Published Date: 05 Dec 2016
Copyright © 2016 Uçkay I
Citation: Steinmetz S, Uçkay I, Cohen C and Abrassart S. (2016). Fever and its Association with Infection in Severely Injured Polytrauma Patients. Mathews J Orthop. 1(2): 011.
ABSTRACT
Background
Polytrauma patients often receive antibiotic therapy because of the high risk of infection and long-lasting posttraumatic fever.
Material and Methods:
Prospectively maintained database of patients hospitalized for severe polytrauma in our intensive care unit. We investigated the overall and daily occurrence of fever (any temperature ≥38°C or 104°F) during the first 15 days of hospitalization and its association with various categorical (Pearson--χ2 -tests) or continuous variables (Wilcoxonranksum-tests).
Results
Among 155 patients with severe polytrauma (median age 38 years), fewer occurred in 80 (55%) despite the prescription of anti-inflammatory drugs in all cases and corticosteroids in 15 cases. Among 90 patients (58%) who were receiving antibiotic treatment (median 2 days) during the two-week window, infection was proven microbiologically and clinically in 18 patients (12%). Fever was noted in 16 patients, or 89% (16/18) among those who were infected. (χ2 -test; p=0.002). Using daily stratified analyses with categorical and continuous temperature variables we confirmed the statistical association of fever with infection for each day (all pvalues <0.01). By multivariate analysis, fever was significantly associated with infection (odds ratio 3.3, 95% CI 1.2-9.4); while surgery, open fractures, and abdominal trauma did not.
Conclusions
For severe polytrauma patients in the intensive care unit fewer is frequent and significantly associated with infection both overall and stratified upon individual days, with no apparent time threshold.
KEYWORDS
Fever; Polytrauma; Infection; Intensive Care; Epidemiology.
INTRODUCTION
Fever is very frequent among patients with severe polytrauma, especially among young patients in the Intensive Care Unit (ICU) [1]. The reasons are multiple, ranging from central nervous thermoregulation following injury, iterative surgeries, atelectasis, or due true infections such as open fractures, ventilator-associated pneumonia, peritonitis, urinary tract infections, surgical site infections, catheter-related sepsis and many more. Recent research also advocates that fever might be influenced by the genetic background of the patients [2- 10]. Persistent fever leads to a costly search for the site of an (occult) infection and very often is the clinical "variable number one" for the suspicion of underlying infection. Unsurprisingly, facing multiple sites of possible infections, the trauma-related immune-suppression of a fragile patient and the difficulty to distinguish between microbiological contamination and true infection, clinicians prefer to cover their patients with antibiotics. Moreover, these patients have freshly implanted osteosynthesis material. Implant-related infections are one of the most feared and clinically devastating complications of orthopaedic trauma surgery, and might seed from distant remote infections [1, 4, 11]. No wonder surgeons, even if they are not directly in charge of the patients, support the choice of broadspectrum agents because of the persistence of fever despite narrow-spectrum prophylaxis administered for prior surgical prophylaxis. On the other hand, it is known that fever per se is not associated with infection in elective orthopedic surgery up to seven days postoperatively, but corresponding data for polytrauma ICU patients are almost absent [3]. In this prospective study, we assess the epidemiological profile of fever and its association with infection during the ICU stay of polytrauma patients.
MATERIAL AND METHODS
We prospectively followed all adult polytrauma patients hospitalized in the ICU and followed by the Orthopaedic Surgery Service of Geneva University Hospitals 2011-2012; with a minimal follow-up of 15 days. Patient's daily clinical parameters, medication, medical and nursing notes, and laboratory results were noted in various electronic files and multiple local Ethical Committee's approbations allowed us to follow these patients. No intervention was performed for this study outside of the usual clinical management of the patients, who were equally followed by attending consultants of the Service of Infectious Diseases (ID). Of note, our ICU do not regularly use cooling methods; besides of antipyretic medication. The patient was considered febrile if there was an axillary or ear temperature ≥38°C or 104°F), at any time of the day and independent of antipyretic medication. The different definitions of nosocomial infections based on the Center of Disease Control criteria, and the judgment of the clinicians and Infectious Diseases physicians that followed the patients [12]. In addition, for this study, data concerning infections and antibiotic treatment were cross-checked by surgeons (SS) not involved in the treatment and an Infectious Diseases physician experienced in surgical infections and antibiotic stewardship (IU) [13].
STATISTICAL ANALYSIS
The primary outcome parameter was the occurrence of infection. For group comparisons, we used the Pearson-χ², Fisherexact or the Wilcoxon-ranksum-tests, as appropriate. A multivariate logistic regression analysis adjusted for case-mix. P values =0.05 (all two-tailed) were significant. STATA™ software (9.0, STATA Corp, College Station, USA) was used.
RESULTS
Overall, 155 patients (124 males; median age 38 years; median BMI 23 kg/m2 ) were enrolled in our study. The median follow-up was 34 days (range, 15-92 days). The median Injury Severity Score (ISS) was 25 (range, 16-75 points) and the American Anesthesiology Associations' Score (ASA) was 2 (range, 1-5 pts). The anatomical regions of the trauma were liver (n=2), kidney (n=4), lower urogenital tract (n=13), pelvis (n=30), face (n=55), central nervous system (n=113), thorax (n=84), peripheral arteries (n=26) and open extremity fractures (n=30). One single patient could have a mix of all these sites. The median duration of intubation was 0 days (range, 0-40 d) and 118 patients (76%) had a urinary tract catheter for more than 24 hours. Almost all had a central venous line. Fiftyeight percent (90/155) were under 18 different regimens of systemic antibiotic treatment or prolonged prophylaxis during their ICU stay; for a median duration of 2 days (range, 1-15 d). In total, 18 patients (12%) were infected, of which three were in sepsis, and three in severe sepsis. All infections were bacterial. Those infections were 8 pneumonia, 2 combined respiratory and surgical site infections, 5 surgical site infections, 2 primary catheter-related bloodstream infections and 1 symptomatic urinary tract infection. In crude group comparison, the severity of the injury, the duration of intubation/ventilation and the occurrence of fewer were the only parameters associated with infection (Table 1).
Table 1: Characteristics of patients with and without documented infection.
| Infection | p-values° | No Infection | |
| n = 155 | n = 18 | n = 137 | |
| Median age | 34 years | 0.76 | 39 years |
| Diabetes mellitus | 2 (11%) | 0.31 | 7 (5%) |
| Median body mass index | 24 kg/m2 | 0.15 | 23 kg/m2 |
| Median serum lactate level (admission) | 35 mmol/l | 0.01 | 23 mmol/l |
| Median ASA Score | 3 points | 0.08 | 2 points |
| Median ISS Score | 35 points | 0.01 | 25 points |
| Median Glasgow Score (admission) | 13 points | 0.08 | 14 points |
| Median duration of intubation | 6 days | 0.01 | 0 days |
| Steroid use | 3 (17%) | 0.29 | 12 (9%) |
| Fever ≥ 38°C (104°F) | 16 (89%) | 0.01 | 64 (47%) |
Pearson χ2-test, Fisher-exact-test or Wilcoxon-ranksum-tests, as appropiate °Significant results are displayed bold and in italic FEVER AND MULTIVARIATE ANALYSES
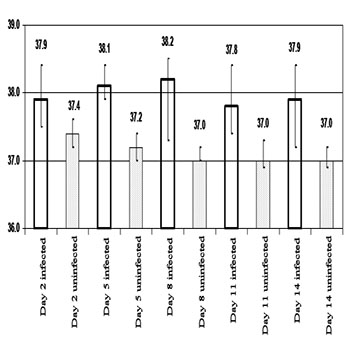
Fever at any time was noted in 80 patients (55%), or 89% (16/18) among those who were infected. Statistically, 89% of all infected patients had fever in contrast to 47% of noninfected patients. Among febrile patients, 80% (64/80) were infected compared to 3% (2/68) of the afebrile counterparts. These differences were significant (χ2 -test; p=0.002)(Table 1). Formally, in predicting infection, fever had a sensitivity of 89%, specificity of 57%, positive predictive values of 28% and negative predictive values of 96%. At the same time, we were unable to define a minimal duration threshold above which the presence of fever would determine underlying infection. The maximum temperature of each of the fifteen first days significantly differed between infected and uninfected patients (Wilcoxon-ranksum-tests, p<0.05) (Figure 1). The exception was the admission day. Within the first 24 hours, the proportion of future uninfected versus infected patients did not statistically differ upon the presence of fever (21/139 vs. 6/18; χ2 -test; p=0.08).
Due to considerable case-mix in the study population and among the infections, we performed a multivariate analysis to estimate the influence of the variable 'infection' regarding the outcome variable 'fever' (Table 2). In this analysis, as in the group comparison, the duration of intubation (odds ratio 1.3; 95% confidence interval 1.1-2.3) and occurrence of fever (OR 3.3, 95% CI 1.2-9.4) were significantly associated with infection. Overall, the odds ratio for fever and infection was 3.3, but this differed according to the day. When we performed the multivariate analysis with the presence of fever only on Day 1, the odds ratio was 3.1, but increased with subsequent days. The odds ratio for infection upon presence of fever was 3.3 at Day 2, and 5.0, 16.3, 20.4, ad 28.7 on Days 4, 8, 12 and 14, respectively. This suggests a higher association with infection as the duration of ICU stay continues. Of note, the goodness-of-fit test was not significant and the Receiver Operating Curve (ROC) value was 0.83, highlighting a more than acceptable accuracy of our final model.
Table 2: Logistic regression with outcome "Infection"
| Univariate analysis | Multivariate analysis | |
| Associations | Odds ratio with 95% confidence intervals | Odds ratio with 95% confidence intervals |
| PATIENT CHARACTERISTICS | ||
| Age (continuous variable) | 1.0, 1.0-1.0 | n.a. |
| Glycemia at admission (continuous variable) | 1.0, 1.0-1.0 | n.a. |
| ASA Score (continuous variable) | 1.0, 1.0-1.1 | n.a. |
| Glasgow Score at admission | 0.9, 0.8-1.0 | n.a. |
| ISS Score at admission | 1.0, 1.0-1.1 | n.a. |
| Abdominal lesions | 1.4, 0.5-3.9 | n.a. |
| Pelvic lesions | 1.7, 0.6-5.3 | n.a. |
| Open extremity fractures | 1.7, 0.6-5.3 | n.a. |
| Thoracic lesions | 2.4, 0.8-7.1 | n.a. |
| Body mass index (continuous variable) | 1.1, 0.9-1.3 | n.a. |
| Blood transfusions | 1.1, 0.8-1.3 | n.a. |
| Fever ≥ 38°C (104°F) | 3.2, 1.1-9.2 | 3.3, 1.2-9.4 |
| Steroid use | 2.1, 0.5-8.2 | 1.6, 0.4-6.9 |
| Duration of intubation (continuous variable) | 1.2, 1.1-1.4 | 1.3, 1.1-2.3 |
+n.a. = analysis not performed due to interaction only results in bold and italic are statistically significant (two-tailed p value =0.05).
DISCUSSION
We evaluated 155 severe polytrauma patients hospitalized in the ICU and operated by the orthopaedic team. As witnessed in other studies, persisting fever was very common involving 55% of all patients [1, 14]. In contrast to the population of elective surgery, the occurrence of fever was significantly associated with infection; overall and stratified upon each single day from admission up to the Day 15 [3]. The odds ratio of association of fewer with infection increased however for the time being hospitalized in the ICU, starting from an odds ratio of 3.2 on Day 2 and ending with an odds ratio of 28 after two weeks. Eighty-nine percent of all infected patients had fever in contrast to 47% of non-infected patients. Among febrile patients, 80% (64/80) were infected compared to 3% (2/68) of the non-febrile counterparts. Of note, the diagnosis of infection was supported by ID Consultants and also retrospectively cross-checked by an ID physician with experience in surgical infections [13]. Moreover, the definition of infection fitted with internationally accepted recommendations. The literature of polytrauma and body core temperature is sparse and complex. Available studies rather wonder if fever is friend or foe [14]. Large national multicenter polytrauma databases suggest that rather hypothermia, not fever, might be associated with an increase of mortality risk, whereas the presence of fever up to Day 4 would not increase mortality [14-17]. Indeed, a large retrospective analysis of 38,550 trauma patients in the USA noted a more than twofold increase in infectious complications, renal failure, adult respiratory distress syndrome, and cardiac arrest in hypothermic patients compared to normothermic patients. The authors are convinced that hypothermia itself could have independent, detrimental effects on trauma patients and is not simply a marker for injury severity [15]. This association is congruent with articles advocating less surgical site infection by avoiding hypothermia during surgery, but stands in contrast to widespread practice of the protective effects of iatrogenic hypothermia during cardiac, transplant, and neurosurgery and has been shown to improve outcomes after cardiac arrest [8, 15]. We cannot solve this contradiction and can only note that the outcome parameters in all these studies were mixed and not forcefully congruent with each other. Whatever the causative link of hypothermia and infection and other complications might be, the potentially adverse effect of hypothermia does not grant a protective effect of fever. To the best of our knowledge, there is no single study advocating a benefit of elevated core temperature beyond normothermia. Our small single-center was equally too small to pronounce on the outcome of febrile patients in terms of mortality and long term sequelae. However, fever in polytrauma patients remains associated with a higher incidence of overall infection. Our findings are confirmed by Mizushima et al. among 253 consecutive polytraumatic ICU patients. The authors identi-fied fever and age as the most important associations with infection [14].
CONCLUSION
We conclude that persistent fever despite anti-inflammatory and antalgic medication needs to be taken seriously and justifies a work-up for underlying infection.
ACKNOWLEDGMENTS
We are indebted to the teams of the Orthopaedic Service, the Intensive Care Units and the Microbiological Laboratory for their invaluable help. The Ethical standard and Conflict of interest i. This is a retrospective study involving severe polytrauma patients directly hospitalized in the Intensive Care Unit and unable to give formal consent for notification of fever. ii. All data sampling involving our own patients were in accordance with the 1964 Helsinki declaration and its later amendments and were clinically oriented. No additional tests, samplings or questionnaires were performed, or have been sent, for study purposes. iii. The study was in line with several ongoing studies approved by local Ethics Committee.
REFERENCES
- Large TM, Alton TB, Patton DJ and Beingessner D. (2013). Does perioperative systemic infection or fever increase surgical infection risks after internal fixation of femur and tibia fractures in an intensive care polytrauma unit? J Trauma Acute Care Surg. 75(4), 664-668.
- Little RA. (1985). Heat production after injury. Br Med Bull. 41(3), 226-231.
- Uckay I, Agostinho A, Stern R, Bernard L, et al. (2011). Occurrence of fever in the first postoperative week does not help to diagnose infection in clean orthopedic surgery. Int Orthop. 35(8), 1257-1260.
- Dunkel N, Pittet D, Tovmirzaeva L, Suva D, et al. (2012). Short duration of antibiotic prophylaxis in open fractures does not enhance risk of subsequent infection. J Bone Joint Surg Br. 95-B(6), 831-837.
- Uckay I, Ahmed QA, Sax H and Pittet D. (2008). Ventilatorassociated pneumonia as a quality indicator for patient safety? Clin Infect Dis. 46(4), 557-563.
- Harbarth S and Uckay I. (2004). Are there patients with peritonitis who require empiric therapy for enterococcus? Eur J Clin Microbiol Infect Dis. 23(2), 73-77.
- Uckay I, Sax H, Gayet-Ageron A, Ruef C, et al. (2013). High proportion of healthcare-associated urinary tract infection in the absence of prior exposure to urinary catheter: a cross-sectional study. Antimicrob Resist Infect Control. 2(1), 5.
- Uckay I, Harbarth S, Peter R, Lew D, et al. (2010). Preventing surgical site infections. Expert Rev Anti Infect Ther. 8(6), 657-670.
- Sax H, Uckay I, Balmelli C, Bernasconi E, et al. (2011). Overall Burden of Healthcare-Associated Infections among Surgical Patients: Results of a National Study. Ann Surg. 253(2), 365- 370.
- Ferguson JF, Meyer NJ, Qu L, Xue C, et al. (2015). Integrative genomics identifies 7p11.2 as a novel locus for fever and clinical stress response in humans. Hum Mol Genet. 24(6), 1801-1812.
- Al-Mayahi M, Betz M, Muller DA, Stern R, et al. (2013). Remission rate of implant-related infections following revision surgery after fractures. Int Orthop. 37(11), 2253-2258.
- Garner JS, Jarvis WR, Emori TG, Horan TC, et al. (1988). CDC definitions for nosocomial infections. Am J Infect Control. 16(3), 128-140.
- Uckay I, Vernaz-Hegi N, Harbarth S, Stern R, et al. (2009). Activity and impact on antibiotic use and costs of a dedicated infectious diseases consultant on a septic orthopaedic unit. J Infect. 58(3), 205-212.
- Mizushima Y, Ueno M, Idoguchi K, Ishikawa K, et al. (2009). Fever in trauma patients: friend or foe? J Trauma. 67(5), 1062- 1065.
- Shafi S, Eliott AC and Gentinello L. (2005). Is hypothermia simply a marker of shock and injury severity or an independent risk factor for mortality in trauma patients? Analysis of a large national trauma registry. J Trauma. 59(5), 1081-1085.
- Martin RS, Kilgo PD, Miller PR, Hoth JJ, et al. (2005). Injury-associated hypothermia: an analysis of the 2004 national trauma data bank. Shock. 24(2), 114-118.
- Shiozaki T, Kishikawa M, Hiraide A, Shimazu T, et al. (1993). Recovery from postoperative hypothermia predicts survival in extensively burned patients. Am J Surg. 165(3), 326-330.