Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2023
Female Masturbation Practices amongst Different Populations and Age Groups
Markus van Niekerk*
Department of Obstetrics and Gynaecology, Riga Stradins University, Riga, Latvia
*Corresponding author: Markus van Niekerk, MD, Department of Obstetrics and Gynaecology, Riga Stradins University, Riga, Latvia, Phone: +(27)825448775; E-mail: [email protected].
Received Date: June 04, 2023
Published Date: July 04, 2023
Citation: Niekerk MV. (2023). Female Masturbation Practices amongst Different Populations and Age Groups. Mathews J Gynecol Obstet. 7(2):28.
Copyrights: Niekerk MV. © (2023).
ABSTRACT
Aim: This study was to assess efficacy of sexual education in schools, the inclusion of female masturbation in such and its sufficiency regarding the preparation of adolescents for safe and consensual sexual activities. Effects of religious, cultural, and parental factors on women’s views on masturbation as well as the nature of women’s emotions during masturbation were assessed. The frequencies of female orgasm during masturbation to sexual intercourse with a partner were compared. Methods: Cross-sectional anonymous online questionnaire with 24 questions both multiple choice and open ended. Inclusion criteria was female/identify as female, 18 years and older. Approval of the study by Riga Stradins Research Ethics Committee. The questionnaire was promoted on various social media platforms and by word of mouth for a period of 3 months. Analyzation of data was conducted via SPSS system. Results: A sample size of 1068 participants, aged ≥ 18years, mainly European (46%) and North American (43%), was obtained. 64.6% reported insufficient sexual education, with 43.3-55.8% stating insufficient preparation for safe, consensual sex. 84.4-85.2% stated that female masturbation was not covered, 59% of participants indicated that female masturbation needs a place in sexual education. Amongst 39.2% of participants, parents didn't discuss any sexual education with them with 29.8% of participants forbidden to engage in pre-marital sexual activity. Amongst those prohibited 38% still masturbated. A total of 1.3% of participants underwent genital mutilation. Assessing frequency of masturbation majority (40.3%) reported to masturbate more than once weekly with the most popular mode of masturbation being sex toys(44%) followed by hands(42%). Comparing the frequency of orgasm while masturbating versus during sexual intercourse with a partner, 59% always report having an orgasm while masturbating solo; compared to 15% when with a partner. Emotions experienced by women during masturbation were mostly positive with the majority feeling relieved (68.7%). Conclusions: Sexual education programs in schools are insufficient in teaching about female masturbation and preparing students for safe, consensual sexual intercourse; they require reassessment by UNESCO and WHO for more efficient implementation. Female masturbation should be considered a right to female sexual health, this needs to be ensured and included as a normal topic of discussion, no longer considered a taboo in society.
Keywords: Sexual Health, Female Masturbation, Female, Masturbation.
ABBREVIATIONS
WHO: World Health Organization; CSE: Comprehensive Sexuality Education; UN: United Nations; UNESCO: United Nations Educational, Scientific and Cultural Organization; IPPF: International Planned Parenthood Federation; MS: Member States; TPPP: Teen pregnancy Prevention Program; EU: European Union.
INTRODUCTION
The beginning of the 21st century sparked a new generation of modernization and inclusion of everyone in society and with these steps forward new topics need to be discussed and changes need to be made to ensure there are equal rights and opportunities for our society. One of these topics that require serious reconsideration and alterations is sexual health. According to WHO sexual health is defined as “a state of physical, emotional, mental, and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination, and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected, and fulfilled” [1].
The following novelty cross-sectional study about female sexual masturbation was conducted with the aim to determine the significance in the shortcomings of the education systems responsible for sexual education, since previous studies have looked at the efficacy of Sexual Education in its delivery to adolescents in the school setting [2], but no studies were found to include whether this prepared students enough for safe, consensual sexual activities or whether it included female masturbation as a topic of discussion. The role that familial traditions, cultural and religious beliefs play in a woman’s view about masturbation and her own sexual health was also studied due to the lack of studies regarding this topic, with one study found regarding guilt feelings toward masturbation and its effect on physiological and psychological effects of masturbation taking the past regarding society and religions view of masturbation into account [3].
With a poor research foundation to assess the frequency of the female orgasm when she is engaging in solo masturbation in comparison to engaging in sexual intercourse with a partner and whether it is also age dependent was studied, since there was only one previous study found regarding the relationship between Masturbation and partnered sexual activity in women-being very specific [4]. Lastly the aim was to determine what mode of masturbation proves most efficient in ensuring an orgasm and what emotions women experience whilst masturbating be it more positive or negative. It is thus of vital importance that more in depth research is conducted in these poorly researched fields to obtain a more well-rounded description of what is lacking in society and medicine when speaking about female sexual health and how these needs can be met.
A BRIEF HISTORY OF FEMALE MASTURBATION, TABOOS OF THE PAST AND OUR CURRENT SOCIETY’S PERCEPTION
According to Britannica Academic Masturbation is ‘manipulation of the genital organs for pleasure, usually to orgasm. The term masturbation generally connotes self-manipulation, but it can also be used to describe manipulation of or by a sexual partner, exclusive of sexual intercourse’ [5].
Female masturbation can be traced back many millennia, with the earliest records dating back to 5000BC Mesopotamia present day Iraq [6]. Masturbation was documented by the Sumerians who had many sexual rituals; their culture was made up of a sexual nature and they believed that masturbation improved their sexual potencies [6]. From 1712-1920 masturbation was classified as a disease that if practiced could lead to amongst others insanity and blindness [7]. The basis of this was Christianity and this change took place shortly after the release of a book titled” Onania; or The Heinius Sin of Self Pollution” in the early 1700s. The author most probably the English surgeon, John Martyn affected the trajectory of modern sexuality by his “discovery” of a disease which he also happened to have a cure for [8]. He based this disease on a biblical character Onan who refused to impregnate his dead brother’s widow [9].
In Catholicism “Onanianism” means coitus interruptus and relevant since their purpose of marriage is procreation. Therefore knowingly not procreating they would violate their marriage and purpose on Earth. This is most probably what was meant in the story of Onan in Gen. 38:8-10 of the Bible, NIV where Judah ordered Onan to marry and impregnate his dead brother’s wife, but Onan hated his brother and did not want to create an heir for his brother so instead he did not ejaculate in his new wife. This was sinful and he was killed, not because he masturbated, but because he hated his brother so much that he didn’t want to procreate in his name [10].
Another book titled: “Plain facts for old and young” by John Harvey Kellogg first published in 1877, masturbation is referred to as: “the most dangerous of all sexual abuses because the most extensively practised.” Kellogg refers to masturbation as “self-pollution, self-abuse,” “solitary or secret vice”[11]. Rosario also refers to female masturbation as”polluting” in his book titled “Phantastical Pollutions: The Public Threat of Private Vice in France” [12].
During the Victorian era doctors would refer female masturbators to mental institutions for treatment where vibrators were often put in use to treat the so called hysteria [13]. Kellogg also mentions a patient who was bedridden with psychological changes after masturbating 10-14 times per day for several weeks [11]. For which he offered treatment options from prevention by abstinence [11] to curative treatment based on duration of the disease and patient’s attitude; from scolding young children, bandaging hands, applying a cage around the genitals in older patients and if unsuccessful circumcision [11]. The Greeks depictions of masturbation were often seen on pottery focusing on two figures [8]. The first being of Satyrs, who were deformed goat-headed beasts with larger stature than a human who were supposedly taught to masturbate by the gods to relieve themselves of their sexual frustrations [14]. These very beasts were seen of lower status, uneducated in comparison to the Greeks [8]. Therefore those who masturbated were also seen as having lower status. Female masturbation is rarely portrayed, [8,15] it can be found in Greek and Latin literature, but women were of low importance and when they masturbated said to only do so since they couldn’t find anyone to help them reach satisfaction [8]. The term masturbator originates from the Romans between 85-103 C.E [8].
It wasn’t until the 20th century that doctors no longer believed masturbation to be a disease, but the remnants of it stayed well into the 1900s with children still being told of the negative consequences of masturbating. Many diseases now had specific causes among others Tuberculosis is caused by a bacteria and not masturbation [8]. Masturbation became the source of sexual pleasure for years to come. People were no longer threatened with consequences and there was a goal to implement sexual education and a thought process that it is normal to masturbate, but this was flawed. People still felt the decades of guilt and societal inappropriateness to be present. Between the 1950s-70s massive progression was made concerning female sexuality after Kinsey, Pomeroy, Martin, Gebbhard, Masters, Johnson, Hite conducted different studies on female sexuality and masturbation. Where a mere 20% of study participants used vaginal penetration during masturbation, proving the myth that a penis/object of similar shape was not vital for sexual satisfaction. Further study questions also showed that when women did not orgasm it could be connected to penis-vaginal penetration [16].
It wasn’t until the 1960s that masturbation became a platform for self-expression, autonomy over one’s body, self-pleasure for the sake of self-satisfaction, the sex toy industry exploded, and sex parties became popular [8]. Hite further explored the topic even making a questionnaire for females in which he challenged societal norms about female masturbation by promoting female masturbation, that it is a form of self-expression and getting to know oneself [16].
EFFECT OF RELIGION, PARENTING VIEWS AND CULTURE ON FEMALE PERCEPTION OF MASTURBATION
Research about masturbation is difficult to find and still seems to be a taboo topic of discussion and in the past most research has been regarding sexual intercourse between two people and things must change. An article written by Nantje Fischer regarding the ‘Prevalence of Masturbation and Associated Factors Among Older Adults in Four European Countries’ addresses this issue. A cross-sectional study with a sample size of 3816 people aged between 60-75 taking socioeconomic factors into account when analysing the participants’ overall health, sexual activities including their masturbation practices. The contributing factors to participants masturbating included unsatisfactory sex and absence of love [17]. It showed that people who were sex-positive probably masturbated, in contrast to those who had a pessimistic view were less likely to masturbate or indicate that they masturbate in the questionnaire. In order to move forward from previous falsities regarding masturbation and the effect aging has on adults sexual behaviour more research and awareness programs need to be implemented [17].
Impact of Religion on Female Perception of Masturbation
In chapter one the Christianic views on Masturbation have been discussed [9,10] and one more diverse religious group that needs discussion is the Islamic Faith. According to the Quran 23:5-7 “And they who guard their private parts except from their wives or those their right hand possess, for indeed, they will not be blamed but whoever seeks beyond that, then those are the transgressors” [18]. When questioned about these verses Imam Ja’Far as-Sadiq who was a spiritual leader after the Prophet Muhammad commented that masturbation was included as a transgression [19]. Some ways to not succumb to temptations of this kind are by getting married [20,21], if that is not an option fasting can be used since it will decrease one’s sexual temptations [19,22] amongst others one is also recommended to take a cold shower to decrease the sexual needs, praying to God for help, exercise and even being more social [19].
Impact of parenting view on masturbation
In an article written by Klukas with regards to how parents’ views around masturbation and how it can affect their children a study was conducted among 279 university students. The results showed that those who did not talk about masturbation with their parents showed largely negative views towards masturbation than those who discussed it with their parents [23]. When comparing the male and female participants the females reported a less negative view on masturbation. Parenting style thus had a large influence on the susceptible adolescent view later in life [23]. Another study of students both gendered aged 15-18 advocated for the stance that those who had honest open relationships with their parents regarding sexual acts were likelier to admit they masturbate [24].
Impact of Culture and Female Genital Mutilation
The main source of a female orgasm is the clitoris which is innervated by a large amount of nerve endings which can be stimulated by touch. Other contributing structures include the vaginal introitus, vestibule and labia minora together with bodily touch from a partner, arousal of levator ring muscles, pelvic ring muscles, and breasts [25,26]. The mind is also powerful enough to induce orgasm simply by thoughts and no physical stimulation [25]. The main reason that circumcision is done is to decrease sexual urges and to protect the woman’s virginity and once surgical work is done around the genitalia which are very sensitive it increases the risk of psycho-physical trauma [25,26]. Adverse results include traits such as anxiety, panic attacks, feeling of humiliation and abandonment by the parents who raised the child seem to be predominant. Peer pressure in certain cultures make some girls believe that circumcision is necessary due to them being unclean and susceptible to temptations of sexual desire and that this cleansing will make them whole [26]. This can result in anxiety and feelings of guilt when not done as she will not find a partner who wants someone not circumcised [25,26]. Female genital mutilation is still prevalent in parts of Asia, the Middle East and most common in Northern Africa, with WHO’s prediction standing at more than 100 million people worldwide living with the mutilation, of which approximately 90 million are from Africa [26]. In women who underwent mutilation effects include foremost pain, bleeding and puts patient at risk of infections such as tetanus, HIV, [26,27] with late complications such as problems to void and incontinence, [26,27] a decreased response to sexual stimulation, anorgasmia, those with vaginal closure can lead to penetration per vagina not being possible where partners then use anal penetration or even the urethral orifice [25,26]. There can be various side effects including a psychosocial impact due to possible infertility resulting in some women being abandoned by their partners [27]. This being said many circumcised women don’t experience those complaints, but it does increase the likelihood of anorgasmia [25,27]. Although this cruel, inhumane process has been banned in many countries, and considered as a “violation of human rights” since 1993 according to the Vienna World Conference [26], many communities still perform these rituals unsafely and this unfortunately still gives rise to many health complications [25].
SOURCES OF SEXUAL EDUCATION AND ITS EFFICACY
Since the 1900s sex education was a very controversial topic in the USA. Education associations suggested the need for programs, but they were only implemented in the 1950s together with the medical association in releasing the “sex education series” [28]. Disagreements exist between the liberals and conservatives. Between the 60s and 80s the John Birch Society called it a ‘Filthy Communist plot’ and their view was that it sparked higher numbers of sex among adolescents [28]. Evidence-based research indicated that it did the complete opposite by delaying the age of sexual onset and teenage pregnancies [28].
Initially the programs in the 80s included human growth and development courses. This included also teaching students the responsibility as well as the right to their personal decision making by also teaching skills of parenting and the financial responsibilities of supporting a family [28]. By the end of the 80s the HIV epidemic emerged and it was suggested to include prevention methods in teachings including the first call to include homosexual relationships in the programs. Controversial opinions resulted in conservatives implementing a sex education that is based on fear and abstinence [28]. Jocelyn Elders the Surgeon General of USA from 1993-1994 was asked to step down after publicly stating that masturbation be included in sexual education curricula, an indication to our societal norms 30 years ago [29].
According to UNESCO “Comprehensive sexuality education (CSE) is a curriculum-based process of teaching and learning about the cognitive, emotional, physical and social aspects of sexuality. It aims to equip children and young people with knowledge, skills, attitudes and values that will empower them to: realize their health, well-being and dignity; develop respectful social and sexual relationships; consider how their choices affect their own well-being and that of others; and, understand and ensure the protection of their rights throughout their lives” [30].
Sexual Education in the USA
When looking at the current situation of Sexual Education in the USA we can refer to an article written by the Guttmacher Institute about the negative effect of the purely Abstinence programs. It is active in certain U.S. states and receives government funding of 75 million dollars per year [31]. Their research showed these areas had increased pregnancy rates and births and similar incidence of sex before marriage, STIs, anal and oral sex as those who didn’t. Promote these programs [31]. It showed that adolescents (57%) have had sexual relations by the end of high school.
The abstinence programs on the other hand instead of being informative cause adolescents to develop feelings of guilt, fear, and even shame with regards to sex before marriage [31]. The curricula are also not inclusive to the LGBTQ community as they are mostly heteronormative and thus putting this community at higher risk. They don’t include information with regards to domestic and sexual abuse and thus often allow victims to not feel heard and able to voice their concern with experienced events [31]. The American Medical Association, American College of Obstetricians and Gynaecologists and Society for Adolescent Health and Medicine are all against this program [31].
A fact sheet published by the Guttmacher Institute on “Federally Funded Sex Education” claim that it is of necessity that the youth have access to “ comprehensive sexual and reproductive health information that is medically accurate, LGBTQ inclusive, and culturally and age appropriate so that they can make informed decisions about their sexual behaviour, relationships and reproductive choices” [32].
There are two active programs the first being the “Teen pregnancy Prevention Program (TPPP)” who aim to decrease the frequency of teen pregnancies and it is evidence-based [32]. Government funded since 2014 for NGOs, government organisations, hospitals, clinics, schools, universities [32].
The second program ‘Personal Responsibility Education Program (PREP)’ is government funded since 2010, with a goal to decrease pregnancy and STIs among teenagers by marking the importance of abstinence and contraception. It deals with youth-19 that are in the orphanage system, HIV positive, human trafficking survivors and those that live in regions with increased incidence of teenage births [32]. The curriculum is composed of: healthy relationships, life skills and lastly adolescent development [32].
Guttmacher institute emphasize the need for sexual education to include:” Human development, relationships, communication, decision making skills, sexual behaviour, sexual health, and cultural representations of sexuality and gender. These curricula frame sexuality as a normal part of life and are medically accurate, LGBTQ inclusive, and culturally and age appropriate” [32]. Isabella Caruso’s article also points out contributing factors include funding budgets, inadequate updating of the curriculum per specific community and systemic barriers to the delivery of sexual education to adolescents especially to the previously marginalized Latino, Black, African American and LGBTQ+ communities [33].
Reviewed curricula in 2018 by United Nations showed that comprehensive sex education programs contribute increase age of onset and frequency of sexual activity among adolescents, decrease in partners, increased use of preventative methods like condoms and other contraceptive methods [32]. Homophobia amongst peers decreased by broadening their understanding of gender, and communicatory competencies [32].
Sexual Education within the European Union
Organisations such as the World Health Organisation (WHO), United Nations (UN), and UNESCO set forward guidelines for the European Countries with regards to sexual education.
Refer to Figure 1 for a timeline showing the progression of sexual education across the decades until now. Regulation of such is difficult programs since every country differs in opinion on the how and if this information should be delivered to students, parents’ involvement, age of education, depth at which it is delivered [34].
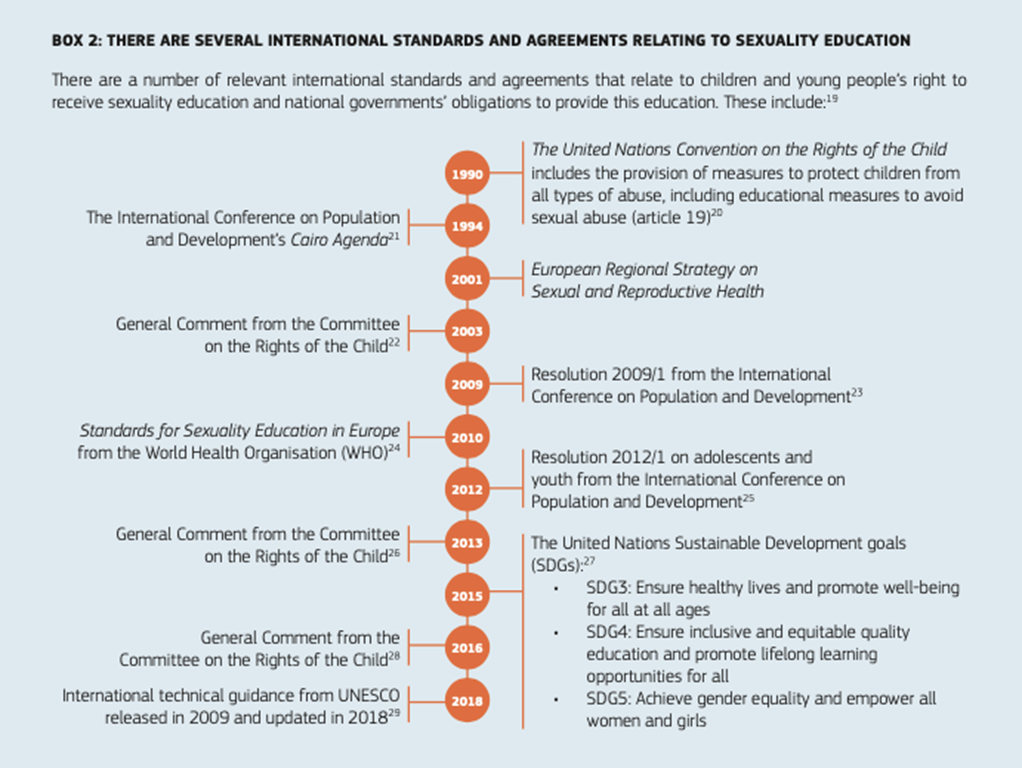
Figure 1. Timeline showing the progression of sexual education as described in “sexuality education across the European union: an overview” [34].
The guidelines clearly indicate that evidence-based studies suggest sexual education has positive outcomes on the sexual health of adolescents. It showed older age of sexual onset, increased use of contraceptive and barrier methods, a decrease in unsafe sexual practices including multiple partners [34]. Although it is not possible to prove that sexual education leads to a lower rate of teen pregnancies/STIs/HIV it also doesn’t increase the risk in adolescents. Even though you cannot say that one program that is effective in one school or country will be effective in another it has been observed to also have a positive outcome in other locations. With these programs in place it has also created a platform not only when it comes to sexual health, but also how healthy relationships look like and also advocates for equal gender rights [34].
UNESCO recommendations on major themes to be included in sexual education curriculum spread among the various age groups include: “Relationships, Values, Rights, Culture and Sexuality, Understanding Gender, Violence and Staying Safe, Skills for Health and Well-being, The Human Body and Development, Sexuality and Sexual Behaviour, Sexual and Reproductive Health” [34]. Included in these programs is to the aim to fight sexual abuse and sexual abuse of children including child pornography by means of education. These programs will soon also include information of harmful sexual practices such as genital mutilation, forced abortions and sterilisations against will and forced marriage.
The European Union Member States are expected to follow these recommendations set out by WHO and UNESCO for sexual education in Europe. In the last years the International Planned Parenthood Federation (IPPF) released data on the member states and their efficiency of sexual education [34]. Since 2019 amongst the different Member States (MS) sexual education is compulsory in 19 and optional in 8. Refer to Figure 2 to see the EU member states where sexual education is mandatory and in which it is optional. Those uncoloured indicate that the data is unknown. The age at which children are educated also differs depending on the law [34]. Even though the member states are required to follow the protocols set out by WHO and UNESCO, there is still variation in the curriculum presented to the students and the way it is being delivered [34].
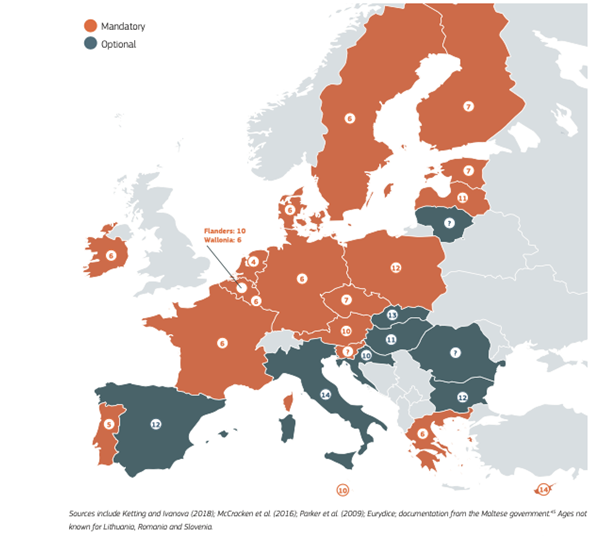
Figure 2. A representation of EU member states with mandatory or optional sexual education. Data of the uncoloured countries is unknown [34].
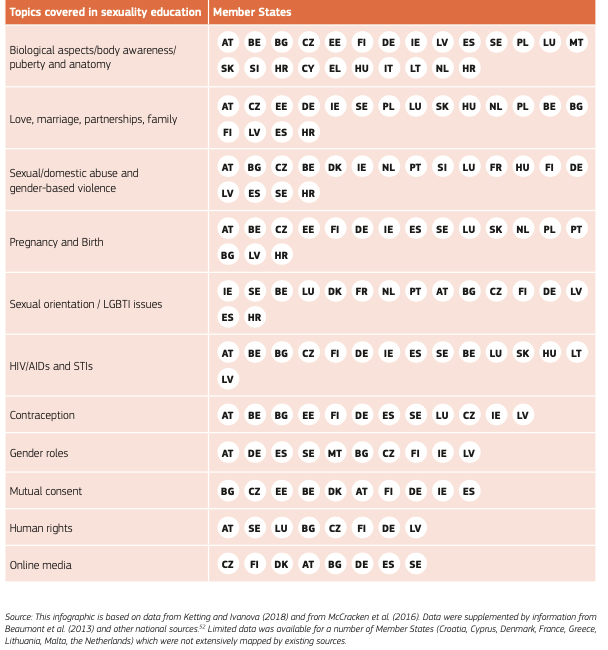
Refer to Table 1, where it shows data that was collected by different sources to have a better understanding of what is covered in the curriculum of the different Member States. The topics covered was obtained by the UNESCO guidelines and the IPPF in 2018.In this table we can see majority of Member States pointed their attention to anatomy, the human bodies and sexual reproduction and this corresponds with a survey from School Education Gateway Sex Education Survey where 86% stated that the same topics were taught. Many of the MS (Member States also taught safe sexual practices including contraception, STIs, pregnancy and birth and gender based violent attacks. In several countries (Cyprus, Italy, Romania, and Slovenia) the programs main teaching topics included the biological side [34]. Another few only focused on biological and risk prevention (Bulgaria, Croatia, Czech Republic, Ireland, Lithuania). In Bulgaria, Croatia, Italy, Lithuania, and Romania sexual education is not mandatory.
Table 1. A Representation of the Themes Covered During Sexual Education in the EU States [34].
Examples of member states that focus on biological and risk prevention.
In Italy some schools do provide their students with sexual education, but this is depending on the school heads and if provided has the tendency to only include the biological side.
In Ireland on the other hand, it there is a focus on biological aspects, as well as risk prevention by means of promoting abstinence. Even though most of the member states offer some sexual education the variability among them is large. For example in Slovakia it is labelled “Education for Marriage and Partnership”, but in Denmark it is inclusive and explores different relationship approaches.
An example of a Member State that has a Holistic approach is Austria. They believe that sexuality is part of someone’s overall being and that sexual education should support these young people in their development into adulthood [34]. It is therefore very detailed and holistic following the guidelines set by WHO. They focus on biology, prevention of teen pregnancy and venereal diseases as well as topics such as identity, consent and online media, gender-based violence.
Training of teachers in sexual education also seems to lack across all EU MS. Close to half of MS where sexual education is compulsory there is only training for teachers when necessary or on a voluntary basis this includes countries such as Belgium, Denmark, Germany, Ireland, and Latvia amongst others [34]. And when surveyed only 1/10 including teachers and parents as well as others involved in the education process had training that was continuous and relevant on sexual education. In MS such as Estonia and Sweden sexual education is part of their bachelor’s program, but not taught again. In Finland as of 2020 sexual education is now a continuous learning program [34].
In contrast to the guidelines set out. Some MS (Austria, Bulgaria, Ireland, and Poland) allow parents to remove their children from school when sexual education is being taught and in Poland even though it is legally required to teach there is a lot of opposition and thus not commonly taught [34]. In Poland there have even been attempts to criminalise sexual education when there is promotion of sexual behaviour among minors.
EVOLUTION OF THE PORNOGRAPHY INDUSTRY AND THE EFFECTS IT HAS ON TEENAGE USERS
Evolution of the Pornography industry until present day
Up until the 1860s the medium through which pornography (hereafter referred to as porn) was portrayed was via art, paintings, pottery, sculptures. The first known time porn was published was in the year 1524 in Rome, Italy, it was of 16 explicit engravings by the artist Guilio Romano, I Modi [35].
The next century saw the invention of photographs and in the late 1890s the start of porn magazines. A couple decades later in the early 1900s short films were developed for viewing and towards the mid-end of the 1900s full length films with sound replaced the previously silent films and these decades also saw the start of peepshow booths [35]. Between the 70s and 90s more and more publications emerged then even starting to offer porn content to be discretely sent to buyers homes. These decades also saw video cassettes developed and allowed people to rent/buy content and watch it at home. TV programmes also started showing late night porn [35,36].
Between the 90s and early 2000s internet at home was introduced making it even more accessible for users to watch porn anonymously [36]. Fetishes and every imaginable position were now at the fingertips of users anonymously and at prices that were affordable [37]. Sexuality drifted more into the film and music industry and flooded our current society [35]. Between then and now the paying for a single time viewing of images or videos has become an advertisement platform and viewers can access many sites with no charge [35-37].
The Effect Pornography has on its Users
The notion that pornography can have harmful effects on the way people act in relationships is important as well as the effect it can have on one’s image of one’s body and self-esteem. One needs to understand that one’s body image needs to come from inside and one needs to try limiting external factors such as pornography from affecting it. Youth should not allow their partners or friends to verbally tell them what is not beautiful about them.[31] It is something most people struggle with, but accepting one’s body is of vital importance to one’s happiness. Not only pornography creates stereotypes, but also mainstream media as seen on TV often includes scenes with partial or even full nudity, this may also be seen in fashion magazines, store mannequins and Facebook or Instagram as to how women and men need to physically appear which creates many problems [38].
A systemic review which analysed more then 20 studies with regards to the sexual behaviours and possible violence seen in porn based of analysing pornographic videos reported that a everyday theme in pornos include not using condoms, gender inequality towards females as well as the possibility to result in absence of a healthy sexual relationship can be observed in regular users of pornographic content [39].
A systemic literature review on adolescent pornography use showed that victimization also seems to be an important topic of discussion, where 11 studies showed that when adolescents were consuming pornography of violent and degradative nature especially towards women [40]. One of those studies showed that users were more likely victims of physical or sexual abuse [41] and later they released another study which showed that adolescents between 10-15 years of age, irrespective of gender were more likely to admit a history of aggression during sexual activities with prior use of pornography [42].
A systemic review conducted by Litsou with regards to the effect pornography use has on females in committed relationships. Both positive and negative aspects were reported with regards to the participants and their partner’s relationships. The reasons given by the females as to why they use pornography included that their masturbation was enhanced, fantasy, to research their own needs, when there was unequal needs between them and their partners [43].
However on the negative side it impacted their intimacy and some felt like it was a form of cheating whether their partner knew or not; giving rise to feelings of guilt. It also gave some women an unrealistic expectation when it comes to sex and their relationships. Those who reported watching pornography with their partners stated that it was to bring intrigue and newness to the relationship trying new things, as well as opens a topic for discussion where partners could discuss their sexual needs and what they like and don’t, but on the other hand the females felt some pressure from their counterparts to take part in sexual activities that don’t feel comfortable with [43].
IMPORTANCE OF FEMALE MASTURBATION FOR SEXUAL HEALTH INCLUDING RISK FACTORS WHEN IT IS NOT MET
According to WHO sexual health is defined as “a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease, dysfunction or infirmity. Sexual health requires a positive and respectful approach to sexuality and sexual relationships, as well as the possibility of having pleasurable and safe sexual experiences, free of coercion, discrimination and violence. For sexual health to be attained and maintained, the sexual rights of all persons must be respected, protected and fulfilled” [1].
All medical health practitioners especially Obstetricians and Gynaecologists are responsible for having open conversations with their patients regarding sexual health. Sexual health is significant because annually approximately 45 000 new HIV cases, 20 million STIs, 3 million unplanned pregnancies and 1 million sexual assaults are reported. Being a healthcare provider one has the ability to reduce these numbers [44].
Masturbation is a way for people to discover more about their sexual side in a safe manner. It can be used as a method of self-pleasure with many benefits from people all over the world. There are many myths that exist regarding masturbation and the damages it poses to one’s health. In fact not only does it not have harmful effects to the human body, it has health benefits. It can help with stress, anxiety depression, promotes better ability to sleep, positive effects on mood, a source of pleasure, improve self-worth, improves knowledge of own sexual needs when later on engaging in sexual intercourse with a partner knowing what exactly arouses them, and how one best reaches sexual fulfilment [45].
A study involving those with a history of solo masturbation and have experienced orgasms were more likely to have a positive sexual development and bodily self-esteem. Those participants were also shown to more likely advocate for their sexual satisfaction by masturbating, speaking up when engaging in sexual activities with a partner, they were more efficient in orgasming, and tended to reflect more on their experiences compared to those who didn’t [46]. Above all of these health benefits it also acts as a contraceptive in preventing pregnancy as well as reduces risk of contracting a STI.
Myths about the harmful effects of masturbation include that it can cause infertility, vision loss, low libido all mentioned in chapter one of this paper during the history of masturbation [9]. The possible harmful effects that could be described surrounding masturbation are that some people could have feelings of guilt as a result of religious and cultural beliefs as mentioned in chapter 2. It is thus important for these people to voluntarily confide in someone with regards to their feelings and how to resolve those inner conflicting thoughts. Another possible negative connotation to masturbation can be those who become addicted to masturbation or sexual activity, but it is not classified in the ICD-10 or DSM-5 as a condition, but depending on the effect it has on one’s everyday life it can be classified under an obsessive-compulsive disorder or an impulse control disorder [45]. People would consider it an addiction the same as any other signs of an addiction when it starts preventing them from doing everyday activities including work, school, cancelling social plans and not attending events.
When assessing one’s sexual health one can use the 5 P’s put forward by the Centre for Disease Control and Prevention. These include Partners, Practices, and Protection from STIs, Past History of STIs, and Pregnancy intention [45]. It is important to counsel patients on safe sexual practices such as STI prevention using barrier methods, and reducing number of sexual partners, preventing unwanted pregnancies with contraceptive usage and promoting safe abortion through clinics. While at the same time marking the importance of safe consensual sexual activities [45].
RESEARCH: A CROSS-SECTIONAL STUDY OF FEMALE MASTURBATION PRACTICES AMONG DIFFERENT POPULATIONS, AGE GROUPS AND THE INFLUENCING FACTORS
Hypothesis
- Religion, culture and parental factors influence once’s views on masturbation.
- Schools do not provide sufficient sexual education including female masturbation to allow women to feel well informed for safe and consensual sexual activities.
- Frequency of Orgasm when masturbating and when engaging in Sexual Intercourse is not dependent on age.
Aim
- To see if Sexual education is thorough including the teaching about female masturbation practices.
- To see if culture, religion, and family influences females’ views on masturbation.
- To see if females from different age groups experience orgasms just as often when masturbating and when engaging in sexual activities with partners.
- To see what mode of masturbation makes females orgasm most frequently.
- To see what emotions females’ experience when masturbating and whether they are more positive or negative.
METHODS
The research for this thesis was done in the form of a questionnaire in the form of a sample of convenience. It was made on Google forms with 24 questions that were both multiple choice and open ended to ensure accurate personal answers were given by participants. The introduction to the questionnaire indicated that upon the time of completing the questionnaire the participants give consent to usage of their anonymous data for the research purposes, that participants remain completely anonymous. The inclusion criteria for the questionnaire was that participants are female/identify as female and 18 years or older.
The questionnaire was approved by the Riga Stradins Research Ethics Committee for research purposes. It was released electronically via various social media platforms including Facebook, Instagram, and WhatsApp. Via different web pages who promote sexual health. It was possible to complete the survey. Upon ending the period of publication, the data was analysed using the SPSS 27 system with the help of Riga Stradins University Statistics Unit staff together with myself. Categorical variables were described as counts and percentages and analyzed with Chi-Square tests or fishers exact tests.
Quantitative data that did not follow normal distribution were later analysed by nonparametric tests. The p=0.05 or less was described as statically significant
During the analysation the participants who answered that they identified as “other” were then excluded from the study since that would bring too many unforeseeable changes in the data set. The data was then imported back to an Excel document from which all the tables and graphs were made. All the research below I claim to be my own and was not obtained by any other sources.
RESULTS
The study included 1068 participants grouped into 4 age groups of which 577(54%) aged 18-25, 411(38.5%) aged 26-40, 77(7.2%) aged 41-60 and 3(0.3%) aged  61 respectively (Table 2).
61 respectively (Table 2).
Table 2. Sample Size of Participants Distributed Into Age Groups
|
Age(Years) |
N |
|
18-25 |
577 (54%) |
|
26-40 |
411 (38.5%) |
|
41-60 |
77 (7.2%) |
|
|
3 (0.3%) |
|
Total |
1068 |

Table 3. Participants Country of Origin and Percentage of Sample Size
|
Country |
N |
|
Argentina |
1 (0.1%) |
|
Australia |
29 (2.8%) |
|
Azerbaijan |
1 (0.1%) |
|
Bangladesh and Singapore |
1 (0.1%) |
|
Belgium |
9 (0.9%) |
|
Brazil |
3 (0.3%) |
|
Bulgaria |
1 (0.1%) |
|
Canada |
60 (5.7%) |
|
China |
1 (0.1%) |
|
Costa Rica |
1 (0.1%) |
|
Croatia |
1 (0.1%) |
|
Denmark |
6 (0.6%) |
|
England |
77 (7.3%) |
|
Estonia |
4 (0.4%) |
|
Finland |
37 (3.5%) |
|
France |
7 (0.7%) |
|
Germany |
77 (7.3%) |
|
Greece |
1 (0.1%) |
|
Hong Kong |
2 (0.2%) |
|
Hungary |
2 (0.2%) |
|
India |
12 (1.1%) |
|
Indonesia |
1 (0.1%) |
|
Ireland |
4 (0.4%) |
|
Israel |
4 (0.4%) |
|
Italy |
32 (3%) |
|
Japan |
2 (0.2%) |
|
Kazakhstan |
1 (0.1%) |
|
Korea |
1 (0.1%) |
|
Latvia |
148 (14.1%) |
|
Mauritius |
1 (0.1%) |
|
Mexico |
4 (0.4%) |
|
Mongolia |
1 (0.1%) |
|
N. Macedonia |
1 (0.1%) |
|
Nepal |
1 (0.1%) |
|
New Zealand |
6 (0.6%) |
|
Nigeria |
1 (0.1%) |
|
Norway |
10 (1%) |
|
Pakistan |
3 (0.3%) |
|
Peru |
1 (0.1%) |
|
Philippines |
4 (0.4%) |
|
Poland |
7 (0.7%) |
|
Portugal |
7 (0.7%) |
|
Romania |
1 (0.1%) |
|
Russia |
3 (0.3%) |
|
Singapore |
3 (0.3%) |
|
South Africa |
30 (2.9%) |
|
Spain |
5 (0.5%) |
|
Sri Lanka |
1 (0.1%) |
|
Sweden |
18 (1.7%) |
|
Switzerland |
3 (0.3%) |
|
The Netherlands |
19 (1.8%) |
|
Tunisia |
1 (0.1%) |
|
Turkey |
2 (0.2%) |
|
United Arab Emirates |
1 (0.1%) |
|
United States of America |
390 (37.1%) |
|
Venezuela |
1 (0.1%) |
|
TOTAL |
1051 |
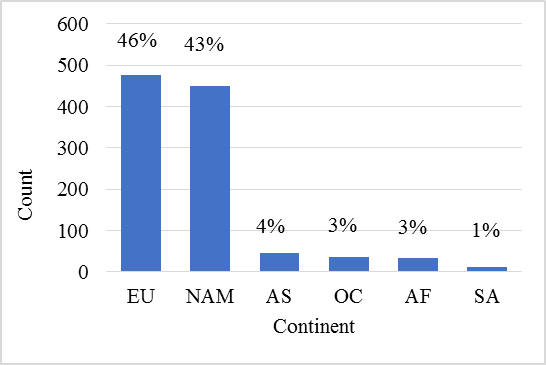
Figure 3. Distribution of participants grouped into continents.
EU - Europe, NAM – North America, AS- Asia, OC- Oceania, AF- Africa, SA- South America
Refer to Figure 4. The next part dealt with the detail in which sexual education was provided in schools based on participants opinions. Where 64.8%(373) of those aged 18-25, 64.1%(263) of those aged 26-40, and 67.5%(52) of those aged 41-60 agreed that it was only partly taught. With 22.9%(132) of the first group, 27.1%(111) of the second and 24.7%(19) of the third agreeing that it was completely taught and in detail. Minority of participants indicated that sexual education was not taught at all. The proportion of the answers in the age groups was not statistically significant, χ24= 5.256, p= 0.262.
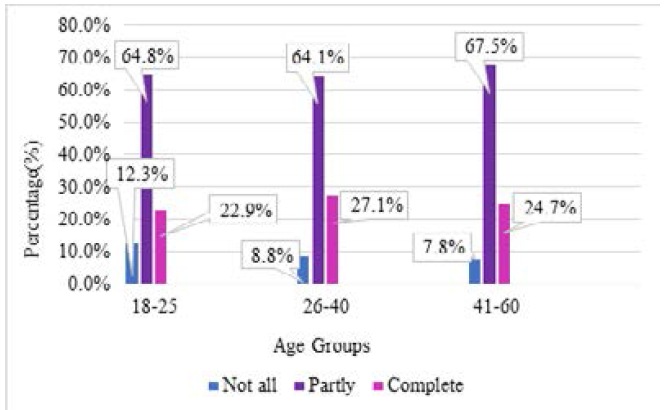
Figure 4. Depth of sexual education provided in schools based on age groups.
Moving to the question whether female masturbation was discussed during the sexual education classes taught at schools. When referring to Figure 5 we can see that amongst the three age groups there is an 84.4-85.2% opinion that female masturbation was not mentioned during the sexual education courses. With a mere 0.2% amongst those aged 18-25, 1.2% amongst those aged 26-40, and 1.3% amongst those aged 41-60 claiming to have had in detail discussions on female masturbation. The proportion of the answers in the age groups was not statistically significant, χ24= 4.486 , p= 0.344.
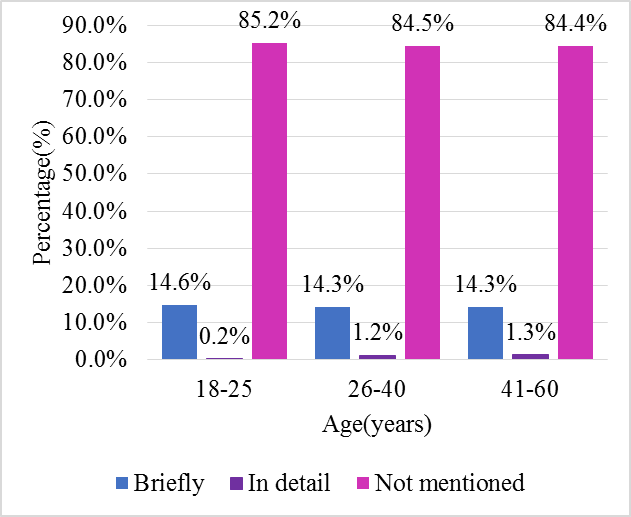
Figure 5. Discussion of female masturbation during sexual education.
The efficacy of sexual education in equipping students with regards to safe, consensual sex was then questioned. Referring to Figure 6 one can see that majority of participants between ages 18-25, 26-40, 41-60, irrelevant of age agreed that sexual education as not satisfactory in preparing them for safe consensual sexual practices. In comparison to those who believe that it was satisfactory, with 21.3% of those aged 18-25, 19.8% of those aged 26-40, and 14.3% of those aged 41-60 believing that it was efficient.
More accurate analysis was then conducted on this question. The proportion of the answers in the age groups was not statistically significant, χ24= 8.502, p= 0.075.
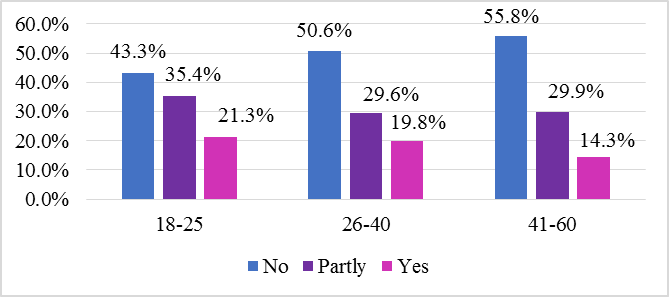
Figure 6. Efficacy of sexual education at schools in preparation regarding safe, consensual sex.
When testing whether the participants would like students to learn more about female masturbation practices at school Figure 7 Shows that 59% agreed with this statement and 8% disagree, with 33% partly agreeing. The proportion of the answers in the age groups was not statistically significant, χ24=4.232, p= 0.375.
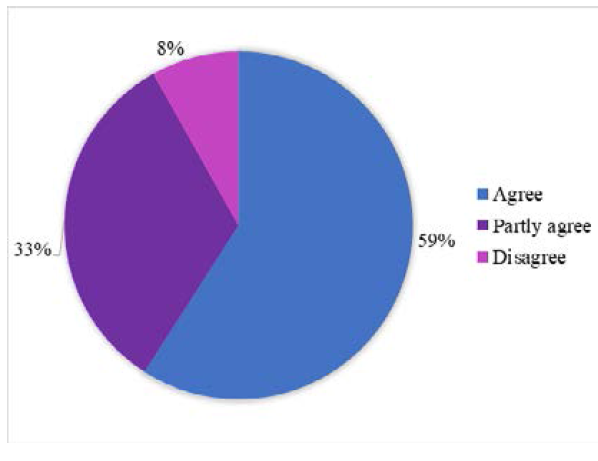
Figure 7. Students should learn more about female masturbation at school.
Referring to results seen in Figure 8 & 9, we can see that majority (39%) of participants indicated that their parents did not have sexual education conversations with them. With 36% feeling as though their parents only partly discussed it with them and a mere 25% of participants indicating that their parents had thorough conversations about sexual education with them.
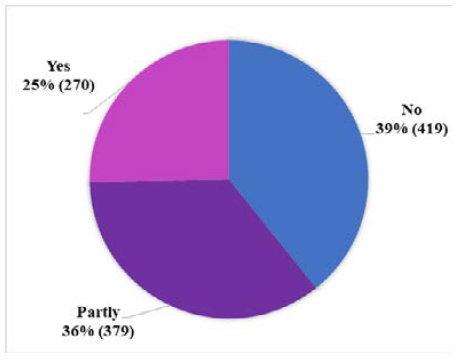
Figure 8. Parent figures discussed sexual education with adolescents.
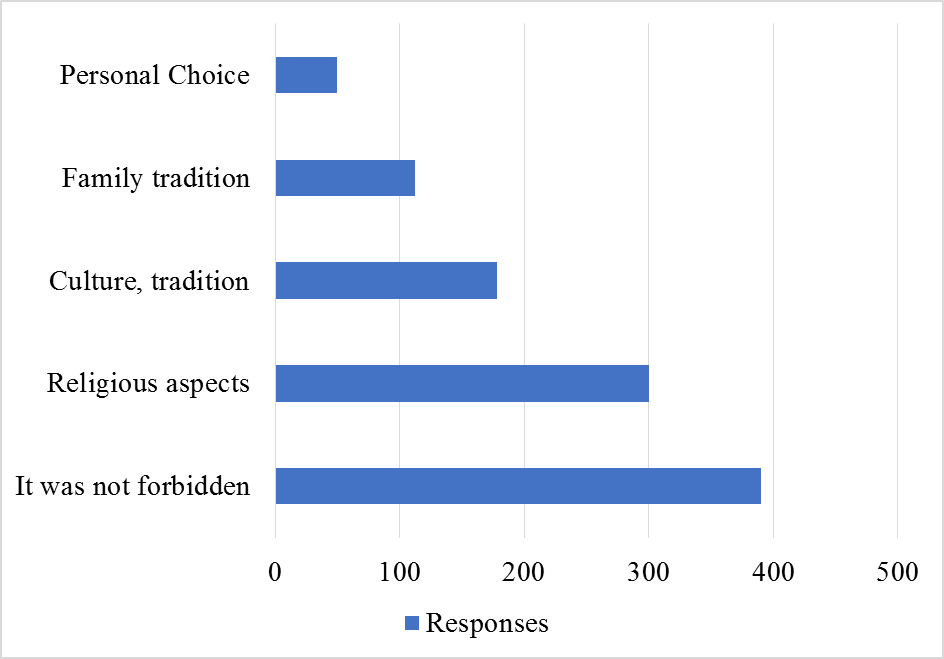
Figure 9. The reasons premarital sexual activity was banned.
Results seen in Figure 10. Following the previous question about whether sexual education was discussed with children by the parents. Now we can also see that there is tendency for those numbers to correlate with these.
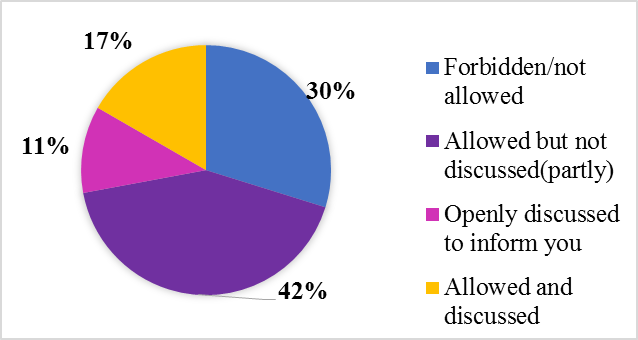
Figure 10. Premarital sexual activity was considered as.
That the minority of women were allowed to have premarital sex (16.7%) and it was discussed with them (11.2%) and majority were forbidden (29.8%) and allowed but not discussed (42.3%). Refer to Table 6 for in depth analysis.
Table 4. Reasons as to why premarital sexual activity was not allowed
|
Culture, tradition |
Religious aspects |
Family tradition |
Personal Choice |
It was not forbidden |
||||||||
|
No |
Yes |
No |
Yes |
No |
Yes |
No |
Yes |
No |
Yes |
|||
|
Age (in years) |
18-25 |
N |
483 |
94 |
442 |
135 |
523 |
54 |
550 |
27 |
350 |
227 |
|
-83.70% |
-16.30% |
-76.60% |
-23.40% |
-90.60% |
-9.40% |
-95.30% |
-4.70% |
-60.70% |
-39.30% |
|||
|
Adjusted Residual |
0,3 |
-0,3 |
3,5 |
-3,5 |
1,2 |
-1,2 |
0,0 |
0,0 |
-2,0 |
2,0 |
||
|
26-40 |
N |
344 |
67 |
282 |
129 |
365 |
46 |
392 |
19 |
270 (65.7%) |
141 |
|
|
-83.70% |
-16.30% |
-68.60% |
-31.40% |
-88.80% |
-11.20% |
-95.40% |
-4.60% |
-34.30% |
||||
|
Adjusted Residual |
0,2 |
-0,2 |
-2,1 |
2,1 |
-0,7 |
0,7 |
0,1 |
-0,1 |
1,2 |
-1,2 |
||
|
41-60 |
N |
61 |
16 |
45 |
32 |
66 |
11 |
73 |
4 |
55 (71.4%) |
22 |
|
|
-79.20% |
-20.80% |
-58.40% |
-41.60% |
-85.70% |
-14.30% |
-94.80% |
-5.20% |
-28.60% |
||||
|
Adjusted Residual |
-1,0 |
1,0 |
-2,8 |
2,8 |
-1,2 |
1,2 |
-0,2 |
0,2 |
1,5 |
-1,5 |
||
|
Chi SQUARE Test Value |
1.036 |
15.472 |
2.191 |
0.048 |
4.938 |
|||||||
|
P value |
0.596 |
<0.001 |
0.334 |
0.976 |
0.085 |
|||||||
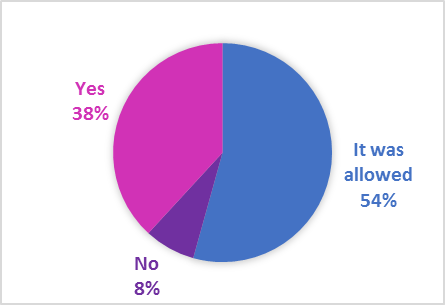
Figure 11. Masturbated despite prohibition of premarital sex.
Referring to Table 5. 14 out of 1061 participants who completed this question were genitally mutilated that is 1.3%. The proportion of the answers in the age groups was not statistically significant, χ22= 1.095, p= 0.578.
Table 5. Participants That Underwent Genital Mutilation.
|
Age(years) |
N |
Total |
|
|
No |
Yes |
||
|
18-25 |
565 (98.6%) |
8 (1.4%) |
573 |
|
26-40 |
402 (98.5%) |
6 (1.5%) |
408 |
|
41-60 |
75 (100%) |
0 (0%) |
75 |
|
Total |
1042 (98.7%) |
14 (1.3%) |
1056 |
See Figure 12. The frequency of masturbation amongst the participants majority (40.3%) report to masturbate more than once per week, but less than daily. With the second group being those who masturbated at least every month, but less than once weekly (23%). The proportion of the answers in the age groups was not statistically significant, χ214= 15.474, p= 0.347.
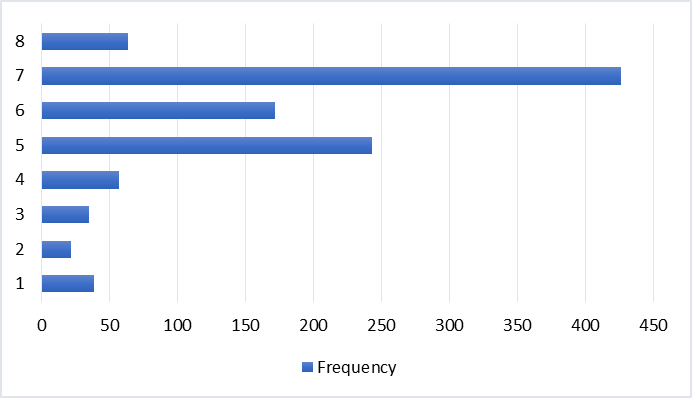
Figure 12. Frequency of masturbation.
1-Never, 2- Less than several times yearly, 3- Several times yearly, 4- Less than every month, 5- Every month, but less than one time per week, 6- One time weekly, 7- More than once per week, 8- Everyday
The mode of masturbation helps the partner to orgasm most of the time refer to Figure 13 the majority answered sex toys (43.6%) shortly followed by their own hands (42.3%). The partner’s hands came in at a mere (9.5%). With the remaining 4% consisting of participants own answers such as: All of the above, none of the above, crossing their legs, using a pillow, mental arousal, showerhead, use of pornography, variation between the different mechanisms.
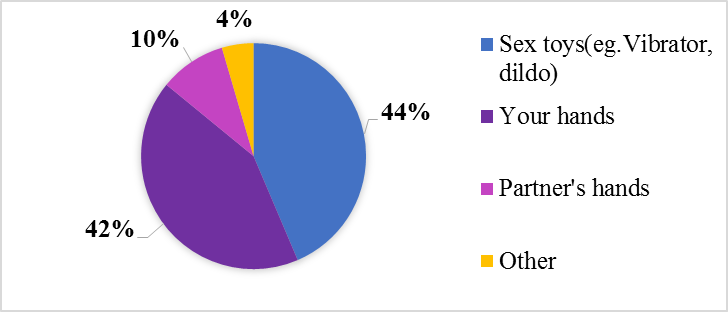
Figure 13. Mode of masturbation with most frequency ensuring orgasm.
When looking at the frequency of orgasm for this group of females refers to Figure 14 there was an even ratio between never and rarely at 3.5% whereas around 59.2% of the participants report to do always orgasm when they masturbate and 26.5% report to often orgasm when they masturbate. The proportion of the answers in the age groups was statistically significant, χ28= 15.850, p= 0.045.
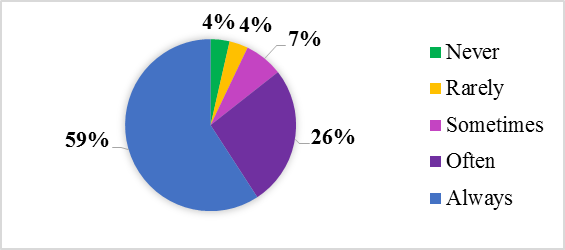
Figure 14. Frequency of orgasm when masturbating.
Looking at how often the participants experience an orgasm when they have sexual intercourse refer to Figure 15 where 14.6% report to always have an orgasm in comparison to 59.2% when they masturbate and often at 30.4% with never and rarely clocking in at 14.5% and 15.8% respectively. There is a major change in the percentage of those who always orgasm during masturbation and those during sexual intercourse. The proportion of the answers in the age groups was not statistically significant, χ28= 36.891, p= <0.001.
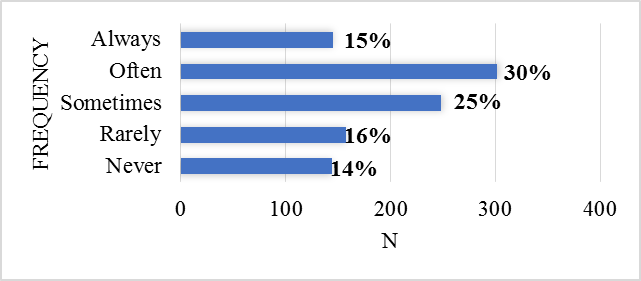
Figure 15. Frequency of orgasm during sexual intercourse.
We can see in Table 6 that majority (68.7%) feel relieved followed by those experiencing Euphoria (47.6%), at Peace(47.2%) and those feeling at Happy(45.7%). We can see majority of participants experience positive emotions, whereas (14.5%) experience feelings of guilt, 13.6%, experience no emotion, 2.3% experience feelings of disappointment (6.6%) and feeling of sin 6.3% .
Table 6. Emotions Experienced During Masturbation.
|
Emotions |
N |
Chi-Square Test Value |
P value |
|
Relieved |
718 (24,8%) |
6.899 |
0.032 |
|
Euphoric |
497 (17,1%) |
2.229 |
0.328 |
|
At peace |
493 (17,0%) |
5.603 |
0.061 |
|
Happy |
477 (16,4%) |
3.284 |
0.194 |
|
Empowered |
243 (8,4%) |
0.241 |
0.886 |
|
No emotion |
141 (4,9%) |
5.254 |
0.072 |
|
Guilty |
153 (5,3%) |
11.85 |
0.003 |
|
Disappointed |
68 (2,3%) |
2.013 |
0.366 |
|
Sinful |
66 (2,3%) |
4.897 |
0.086 |
|
Sad |
45 (1,6%) |
2.671 |
0.263 |
As seen in table 2 the total number of participants included is 1068 with age distribution of those aged 18-25(54%), 26-40(38.5%), 41-60 (7.2%) and 61 or older (0.3%) respectively. From this data it is already apparent that there is unequal distribution amongst the different age groups, but this unequal distribution was already expected due to the belief that the younger generations are more likely to talk openly about topics considered more taboo in the past due to their upbringing being more inclusive and normalization of sensitive topics for discussion taking place in contrast to those that are older who might not be willing to answer or simply because the questionnaire did not reach them based on word of mouth, or technological limitations may have played a role due to the questionnaire only being electronic.
An indication of the distribution of participants based on their country of origin (Table 3), the participants were then grouped into continents (Figure 3) with majority of participants being from Europe (45.39%) following closely is North America (42.82%) with the next closest continent being Asia (4.28%).When looking more closely at individual countries the country with the most participants was United States of America with 390(37.1%) followed by Latvia with 144( 13.7%). The reason for this unequal distribution could be linked to limited methods of distribution used, limitations in various countries to technology or unwillingness to complete the questionnaire due to various reasons.
When looking at the depth of sexual education amongst different age groups, the distribution of it was uneven and that majority (64.6%) indicated that it was only partly provided. When looking at the different age groups and how their opinions are grouped. We can see in Figure 2 that amongst all age groups there are no major differences. With the answers from different age groups ranging between 64.1-67.5% saying that sexual education was only partly provided and a mere 22.9-27.1% agreeing that it was complete and thorough. Thus, we cannot say the sexual education has necessarily improved over the last 5 or 6 decades, but those grouped in the age group 41-60 might affect the data since it was expected that sexual education became more prominent in the last 40 years, to accurately determine this data one would need to know where exactly in that age range the participants are placed.
One study was found which was conducted by Visser and van Bilsen in 1994 surrounding the efficacy of Sexual education delivery in schools [38], but no studies were found to include whether these programs prepared students enough for safe consensual sexual activities or female masturbation was a topic of discussion. Going further into whether female masturbation was discussed during the sexual education course at school Figure 5, a mere 0.2-1.3% of participants said that it was discussed in detail compared to the trend that 84.4-85.2% claims that it was not even mentioned. Since it was already thought that lack of detail would be evident in sexual educations if they are even provided.
Another question arose: Whether sexual education at schools was efficient in providing the adolescents with the knowledge of how to go about safe, consensual sexual practices and the results confirmed that belief. Looking at Figure 6 it is evident that between 14.3-21.3% of individuals believe that the courses were efficient in preparing them for safe sexual practices in comparison to 43.3-55.8% who believed that it was insufficient. Surely this should not be the results we would have liked to see, since this is an indication that almost half of all participants received incomplete sexual education.
When speaking about whether the participants would like students to learn more about female masturbation and referring to Figure 7 we can see that majority of 59% agree that it should be provided, but also a staggering 33% only partly agree with that statement. The proportion of the answers in the age groups was not statistically significant, χ24=4.232, p= 0.375.
Parent figures discussing sexual education with participants referring to the Figure 13 we can see that the majority (39.2%) answered that it wasn’t discussed, shortly following that it was partly discussed (35.5%) and then significantly lower percentage of 25.3% stated that it was discussed. As mentioned in the literature review it discussed a study by Klukas about the negative views’ students can get surrounding masturbation when it isn’t discussed with parents compared to when parent-child conversations took place [23]. That is a possible limitation to this study, since this answer was not researched.
The next question asked was how premarital sexual activity was accepted in the family setting. As mentioned in the results and Figure 10 that minority (19.7%) of women were allowed to have premarital sex with only (11.2%) having had family discussions and 29.8% being forbidden to have sexual interactions pre-matrimony. This raises concerns for our generation since firstly so few had discussions with their parents so how can they be informed about pre-marital sex if their school’s sexual education was insufficient. Secondly how are 29.8% of participant’s parents forbidding sexual activity and not discussing it with their children. Communication is a vital commodity amongst people, who should trust one another, and young students will still do what they want, but without being prepared parents can place their children at unnecessary risk of teenage pregnancies, STDs, unhealthy abusive relationships.
Despite pre-marital sex being prohibited, a mere 8% of participants did not masturbate, comparing to 38% who still masturbated. And another concern that came from this study is that 1.3%(14) participants admitted to having undergone genital mutilation. Refer to Table 5, with 8 aged 18-25 and 6 aged 26-40, even though one might have expected it to be amongst older generations and it is a practice that is dying out. The proportion of the answers in the age groups was not statistically significant, χ24=1.095, p= 0.578.
When assessing the frequency of masturbation referring to Figure 12 majority (40.3%) reported that they masturbate more than once per week with the second group masturbating every month (23%) with only 3.5% stating that they never masturbate. Showing that majority of women masturbate at least once per week to less than several times yearly.
Modes women masturbate with to ensure they orgasm most often Figure 13 include 44% with a sex toy, close second being their hands at 42% and a partner’s hands at a mere 10% which could be due to multifactorial reasons, but can include such as the sex toys vibrating, having a larger diameter to put pressure on the clitoris, the partner knowing how they move the sex toy depending on their bodily needs since they know themselves best and can manipulate their toy or hands according to their needs in comparison to a partner who might not know their body as well as they do.
Referring to Figure 14 showing the results of the frequency of orgasm in women while masturbating and comparing it with Figure 15 showing the results of orgasm frequency during sexual intercourse. Only 15% always orgasm during sexual intercourse compared to 59% always orgasm when masturbating. This is a major difference and can again be multifactorial, but can be due to a woman knowing herself and her needs in order to orgasm better than her partner. If another study were to be conducted one can also include a question asking how many partners they have, for how long and then analyse their frequency of sexual intercourse orgasm with masturbation. On the contrary, a study conducted in 2020 by Rowland using an online survey, although very specific concluded that women who engage in masturbation together with partnered sexual activities were more likely to orgasm and reach greater satisfaction, while also taking into account the satisfaction of the relationship [4].
Lastly, when women feel the need to masturbate there are various emotions that play a role, we felt it important to delve deeper in discovering what those feelings are. Table 6 shows that the majority of feelings women experience when masturbating are of relief (68.7%), followed by 47.6% Euphoric, 47.2% at Peace, 45.7% Happiness, followed by 14.5% with Guilt, 13.6% No Emotion and lower percentages with negative and positive emotions. Women all experience different emotions, whether positive or negative. Positive emotions are what should be felt, but of course negative emotions are inevitable. One study conducted by Kenneth Davidson in 1993 reported that women who had guilt feelings toward masturbation were likely to experience negative emotions towards the practice of it and less prone to report positive physiological and psychological responses post self-gratification [3]. There are various reasons to explain the negative emotions which may include influence of parents, culture, religion, previous bad experiences. These emotions can be studied in more depth when asking specific questions as to why each participant feels positive/negative towards masturbation.
Shortcomings It was attempted to see if a sample size can be reached and compare students from RSU with Latvia’s University, but unfortunately it was not reached thus a comparison cannot be made since most participants were not from either institution.
This study was distributed as widely as possible, in terms of searching for a sample size that is not biased, by sharing it to all women I knew and asking them to do the same, but of course with any study especially this one where many people often feel reluctant to disclose such personal information, even though it was anonymous it makes this study biased since only those open enough to talk about female masturbation and to disclose it, filled it out. So the opinions of those who are not willing to disclose their opinions based on culture, religion, personal privacy were not gained. It was impossible for this study not to be biased from the start, but by making the questionnaire anonymous and by telling the participants that their privacy will be respected we hoped to find a more balanced result.
CONCLUSION
The depth of Sexual Education programs in schools is insufficient in teaching students about female masturbation practices and preparing students for safe, consensual sexual intercourse. The frequency of always reaching orgasm is highest during solo masturbation compared to when engaging in sexual intercourse with a partner, irrelevant of age. The data obtained is insufficient in making a clear conclusion with regards to the influence of religion, culture and parental factors on one’s views of masturbation. Conclusions additional to the hypotheses include-the most frequent mode of masturbation that always ensures orgasm is sex toys, followed by their own hands. Lastly, majority of women experience positive emotions during masturbation.
ACKNOWLEDGEMENT
This research was conducted during my final year of Medicine studies at Riga Stradins Univeristy, in Riga, Latvia.
FUNDING AND CONFLICT OF INTEREST
I did not receive funding or support of any kind and I claim this work to be my own, being the sole author. I do not have any conflicts of interest to declare.
REFERENCES
- WHO. (2006). Sexual and Reproductive Health and Research (SRH). Available at: https://www.who.int/teams/sexual-and-reproductive-health-and-research/key-areas-of-work/sexual-health/defining-sexual-health.
- Visser AP, van Bilsen P. (1994). Effectiveness of sex education provided to adolescents. Patient Educ Couns. 23(3):147-160.
- Kenneth Davidson J, Anderson Darling C. (1993). Masturbatory guilt and sexual responsiveness among post-college-age women: sexual satisfaction revisited. J Sex Marital Ther. 19(4):289-300.
- Rowland DL, Hevesi K, Conway GR, Kolba TN. (2020). Relationship Between Masturbation and Partnered Sex in Women: Does the Former Facilitate, Inhibit, or Not Affect the Latter? J Sex Med. 17(1):37-47.
- (1998) masturbation | Britannica. Britannica Academic, Chicago, IL, USA.
- Leick G. (2003). Sex & Eroticism in Mesopotamian Literature. London and New York: Routledge. pp.1-337. Available at: https://ia800500.us.archive.org/4/items/SexAndEroticismInMesopotamianLiterature/SexAndEroticismInMesopotamianLiterature1994.pdf.
- Whorton J. (2001). The solitary vice: the superstition that masturbation could cause mental illness. West J Med 175(1):66–68.
- Laquer TW. (2003). Solitary Sex: A Cultural History Of Masturbation. USA: VDOC PUB. Available at: https://vdoc.pub/documents/solitary-sex-a-cultural-history-of-masturbation-5u3mb4rkkle0.
- (1756). Onania: or, the heinous sin of self-pollution and all its frightful consequences (in both sexes) considered with spiritual and physical advice to those who have already injured themselves by this abominable practice. London, England: Wellcome Collection. Available at: https://wellcomecollection.org/works/yxrtxsdy.
- Genesis 38. NIV Bible. YouVersion. Available at: https://my.bible.com/bible/111/GEN.38.NIV.
- Kellogg JH, Etter H. (1894). Plain facts for old and young: embracing the natural history and hygiene of organic life - Digital Collections. USA: National Library of Medicine. In: New edition, revised and enlarged. Available at: https://collections.nlm.nih.gov/catalog/nlm:nlmuid-9509955-bk.
- Rosario VA. (2020). Phantastical pollutions: The public threat of private vice in France. UK: Taylor & Francis Group. pp. 101-130.
- Maines RP. (2001). The Technology of Orgasm: “Hysteria,” the Vibrator, and Women’s Sexual Satisfaction. USA: Johns Hopkins University Press.
- Jewell E. (2008). Satyrs & Centaurs. Greece and Rome: The Australian Society for Classical Studies. p. 1-22. Available at: https://www.ascs.org.au/news/prizes_awards/aust_essay_comp/First%20Prize%202008%20Evan%20Jewell.pdf.
- Paula B, Rosario VA. (1995). Solitary pleasures : the historical, literary, and artistic discourses of autoeroticism. UK: Routledge-Taylor & Francis Group. p. 296.
- Passmore R. (1954). SEXUAL BEHAVIOUR IN THE HUMAN FEMALE. By A. C. Kinsey, W. B. Pomeroy, C. E. Martin and P. M. Gebhard. Philadelphia and London: W. B. Saunders Company. 1953. Pp. xxx + 842. £2, 10s. Experimental Physiology. 39(1):73-74.
- Fischer N, Graham CA, Træen B, Hald GM. (2022). Prevalence of Masturbation and Associated Factors Among Older Adults in Four European Countries. Arch Sex Behav. 51(3):1385-1396.
- Surat Al-Mu’minun. The Noble Qur’an-The Holy Quran. Available at: https://legacy.quran.com/23/5-7.
- Hoseini SS. (2017). Masturbation: Scientific Evidence and Islam’s View. J Relig Health. 56(6):2076–2081.
- Muhsin Khan M. (1997). The Translation of the Meanings of Sahih Al-Bukhari: Arabic-English. Illinois, USA: Kazi Pubns Inc. p. 1100.
- Rizvi SM. (2001). Marriage and Morals in Islam. Iran: Ansariyan Publications. p. 62.
- Mesbahzadeh B, Ghiravani Z, Mehrjoofard H. (2005). Effect of Ramadan fasting on secretion of sex hormones in healthy single males. East Mediterr Health J. 11(5-6):1120-1123.
- Klukas E, Draper E, Kaseweter K, Gregoire N, Cioe J. (2021). The Impact of Parenting Style on Attitudes toward Masturbation: A Latent Profile Analysis. J Genet Psychol. 182(6):435-449.
- Smith AMA, Rosenthal DA, Reichler H. (1996). High schoolers masturbatory practices: their relationship to sexual intercourse and personal characteristics. Psychol Rep. 79(2):499-509.
- Abdel-Azim S. (2013). Psychosocial and sexual aspects of female circumcision. African Journal of Urology. 19(3):141-142.
- Groeneveld AE. (2013). Female genital mutilation: Tradition versus human rights. African Journal of Urology. 19(3):134-135.
- Rushwan H. (2013). Female genital mutilation: A tragedy for women’s reproductive health. African Journal of Urology 19(3):130-133.
- Pardini P. (2022). The History of Sexuality Education. USA: Rethinking Schools. Available at: https://rethinkingschools.org/articles/the-history-of-sexuality-education/.
- Hogarth H, Ingham R. (2009). Masturbation among young women and associations with sexual health: An exploratory study. J Sex Res. 46(6):558–567.
- Herat J, Plesons M, Castle C, Babb J, Chandra-Mouli V. (2019). Correction to: the revised international technical guidance on sexuality education - a powerful tool at an important crossroads for sexuality education. Reprod Health. 16(1):30.
- Alan Guttmacher Institute. (2021). Federally funded abstinence only programs: harmful and ineffective. USA: Guttmacher Institute. Available at: https://www.guttmacher.org/fact-sheet/abstinence-only-programs.
- Alan Guttmacher Institute. (2021). Federally Funded Sex Education: Strengthening And Expanding Evidence-Based Programs. USA: Guttmacher Institute. Available at: https://www.guttmacher.org/fact-sheet/sex-education.
- Caruso I, Valdez ES, Lovell CC, Chan J, Beatriz E, Gubrium A. (2023). The Need for Community-Responsive and Flexible Sex Ed for Historically Marginalized Youth. Sex Res Social Policy. 20(1):94-102.
- Picken N. (2020). Sexuality education across the European Union. Luxembourg, Europe: Publications Office of the EU. https://op.europa.eu/en/publication-detail/-/publication/5724b7d8-764f-11eb-9ac9-01aa75ed71a1.
- Weiss R. (2020). The Evolution of Pornography: Love and Sex in the Digital Age. USA: Sussex Publishers, LLC. Available at: https://www.psychologytoday.com/nz/blog/love-and-sex-in-the-digital-age/202007/the-evolution-pornography.
- Price J, Patterson R, Regnerus M, Walley J. (2016). How much more XXX is generation X consuming? Evidence of changing attitudes and behaviors related to pornography since 1973. J Sex Res. 53(1):12-20.
- Cooper A, Delmonico DL, Burg R. (2000). Cybersex users, abusers, and compulsives: New findings and implications. Sexual Addiction & Compulsivity. 7(1-2):5-29.
- Vanessa R. (2017). We Need to Talk about Pornography: a Resource to Educate Young People about the Potential Impact of Pornography and Sexualised Images on Relationships, Body Image and Self-Esteem. Philadelphia, USA: Jessica Kingsley Publishers. p. 258.
- Fritz N, Malic V, Fu T chieh, Paul B, Zhou Y, Dodge B, et al. (2022). Porn Sex versus Real Sex: Sexual Behaviors Reported by a U.S. Probability Survey Compared to Depictions of Sex in Mainstream Internet-Based Male-Female Pornography. Arch Sex Behav. 51(2):1187-1200.
- Romito P, Beltramini L. (2015). Factors Associated With Exposure to Violent or Degrading Pornography Among High School Students. J Sch Nurs. 31(4):280-290.
- Alexandraki K, Stavropoulos V, Anderson E, Latifi MQ, Gomez R. (2018). Adolescent Pornography Use: A Systematic Literature Review of Research Trends 2000-2017. Curr Psychiatry Rev 14(1):47-58.
- Ybarra ML, Mitchell KJ. (2005). Exposure to internet pornography among children and adolescents: a national survey. Cyberpsychol Behav. 8(5):473-486.
- Litsou K, Graham C, Ingham R. (2021). Women in Relationships and Their Pornography Use: A Systematic Review and Thematic Synthesis. J Sex Marital Ther. 47(4):381-413.
- (2017). Committee Opinion No 706: Sexual Health. Obstet Gynecol. 130(1):e42-e47.
- Centers for Disease Control and Prevention. (2022). A Guide to Taking a Sexual History. USA. Centers for Disease Control and Prevention. Available at: https://www.cdc.gov/std/treatment/SexualHistory.pdf.
- Horne S, Zimmer-Gembeck MJ. (2005). Female Sexual Subjectivity and Well-Being: Comparing Late Adolescents with Different Sexual Experiences. Sexuality Research and Social Policy. 2:25-40.