Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2024
Erectile Dysfunction: Epidemiological and Clinical Case Series Profile at the Ibn Rochd University Hospital in Casablanca
Yassine Daghdagh, El Mostapha Abdi, Mahmoud Alafifi*, Anas Tmiri, Mouad Elbade, Amine Moataz, Mohamed Dakir, Adil Debbagh, Rachid Aboutaieb
Department of Urology, University Hospital Center IbnRochd Casablanca and Faculty of Medicine and Pharmacy of Casablanca, Morocco
*Corresponding author: Dr. Mahmoud Alafifi, Department of Urology, University Hospital Center IbnRochd Casablanca and Faculty of Medicine and Pharmacy of Casablanca, 19 Tarik ibnou quartiers des hôpitaux, Morocco, Phone: +212700148612, E-mail: [email protected]
Received Date: April 04, 2024
Published Date: April 17, 2024
Citation: Al-Affifi M, et al. (2024). Erectile Dysfunction: Epidemiological and Clinical Case Series Profile at the Ibn Rochd University Hospital in Casablanca. Mathews J Urol Nephrol. 6(1):18.
Copyrights: Al-Affifi M, et al. © (2024).
ABSTRACT
Erectile dysfunction (ED) is a prevalent condition with significant impacts on individuals quality of life and intimate relationships. Despite its common occurrence, ED often remains underreported and undertreated. This retrospective study aimed to investigate the epidemiological and clinical characteristics of ED among patients consulting at the andrology department of Ibn Rochd University Hospital in Casablanca over a two-year period (January 2022 to January 2024). A total of 205 patients were included in the study, with 101 presenting with ED, constituting 49.3% of the cohort. The average age of patients with ED was 55 years, with a notable prevalence observed among individuals aged 61-70 years. Most patients were monogamous and of urban origin. The majority of patients exhibited a sedentary lifestyle, overweight status, and a high prevalence of smoking, alcoholism, and cannabis use. The onset of ED was gradual in the majority of cases, with a significant delay in seeking medical help, often consulting traditional healers first. Comorbidity factors such as diabetes, hypertension, and ischemic heart disease were prevalent among ED patients. Physical examination findings revealed various anomalies, including penile curvature and benign prostatic hypertrophy. Psychosocial impacts of ED were evident, with marital conflicts and dissatisfaction in sexual relationships being primary concerns. The severity of ED ranged from moderate to severe, with associated disorders such as lower urinary tract symptoms, libido disorders, and premature ejaculation. The findings of this study underscore the importance of proactive screening for ED in clinical practice, particularly among individuals with comorbidities such as diabetes and hypertension. Early identification of ED and its associated risk factors can facilitate timely intervention and management, ultimately improving patients' overall health outcomes and quality of life. Furthermore, our study highlights the need for comprehensive management strategies tailored to individual patient needs, including lifestyle modifications, pharmacological interventions, and psychosexual counseling. Future clinical practice should prioritize a multidisciplinary approach to ED management, integrating urology, endocrinology, and psychology services to provide holistic care. Monitoring the outcomes of these interventions will be crucial to evaluating their effectiveness and refining treatment protocols to optimize patient outcomes.
Keywords: Erectile Dysfunction, Impotence, Urology Department, Ibn Rochd University Hospital, Casablanca, Penile Erection.
INTRODUCTION
Erectile dysfunction (ED) is a condition defined by the persistent or recurrent inability to obtain or maintain penile erection permitting sufficient satisfactory sexual intercourse [1]. The term erectile dysfunction replaced the term impotence in the 1990s.
Erectile dysfunction is a common pathology which considerably affects the couple's quality of life. It affects nearly one in two men over the age of 45 [2].
Age is one of the risk factors for ED which includes poor general health, and the presence of diabetes, cardiovascular disease, psychiatric illness, psychological disorders, unfavorable socioeconomic conditions, and hormone deficiency are proven risk factors for ED.
The aim of our study is to study the epidemiological and clinical characteristics of erectile dysfunction in patients consulting in the urology department in the Ibn Rochd University Hospital in Casablanca. This study explores various factors related to ED, including patient backgrounds, health conditions, and how ED affects their lives, it considers how Moroccan culture and society influence ED, which helps in tailoring healthcare to local needs.
PATIENTS AND METHODS
This was a retrospective study, carried out over a period of 2 years from January 2022 to January 2024 in the andrology department of Ibn Rochd university hospital center in Casablanca.
205 patients were seen in consultation, 101 of which suffering from erectile dysfunction, patients consent were taken. The parameters evaluated were: sociodemographic data, comorbidity factors, risk factors, clinical and par-clinical data, and severity of the disorder. Patients in whom psychogenic, organic or treatment-induced ED was included (ED after pelviperineal surgery, spinal cord trauma, androgen deprivation or any other treatment that could cause ED).
The evaluation of erectile function was made on the basis of the International Index of Erectile Function (IIEF) simplified into 5 questions.
RESULTS
In total, 205 patients were seen in andrology department, of which 101 patients presented with erectile dysfunction, or 49.3% (Table 1). The average age of the patients was 55 years with extremes of 24 and 77 years. The most represented age group was between 61 and 70 years old with 32.5% (Table 2). 73 patients were monogamous (72.3%), 16 patients were single (15.8%), widowed were only 1% of cases and divorced were 11 patients (10.9%) (Figure 1). Most of our patients were of urban origin (66.3%).
Table 1. Distribution according to reasons for consultation
|
Reason for consultation |
Number of patients |
Percentage % |
|
Erectile dysfunction |
101 |
49.3 |
|
Infertility |
43 |
21 |
|
Penis seams |
25 |
12.2 |
|
Ejaculation disorders |
20 |
9.8 |
|
Hemospermia |
9 |
4.3 |
|
Scrotal pain |
7 |
3.4 |
|
Total |
205 |
100 |
|
Age range |
Number of patients |
Percentage % |
|
19-30 |
6 |
6 |
|
31-40 |
12 |
12 |
|
41-50 |
14 |
14 |
|
51-60 |
27 |
26.5 |
|
61-70 |
33 |
32.5 |
|
71-80 |
9 |
9 |
.png)
Figure 1. Distribution of patients according to marital status.
Professional situation: Traders were the most represented (26.7%) followed by retirees 16.8% (Figure 2). Income was less than 3000 dirham (300 euros) in 77 patients (76.3%). The informal sector was the most represented (68.3%) followed by the private sector (16.8%) then the public sector (14.9%).
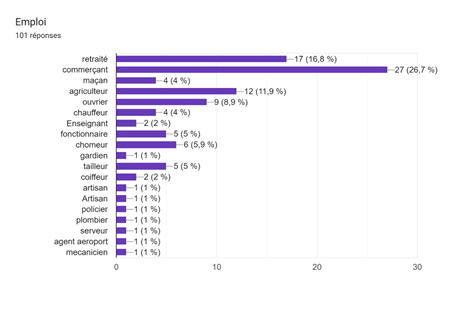
Figure 2. Distribution of patients according to profession.
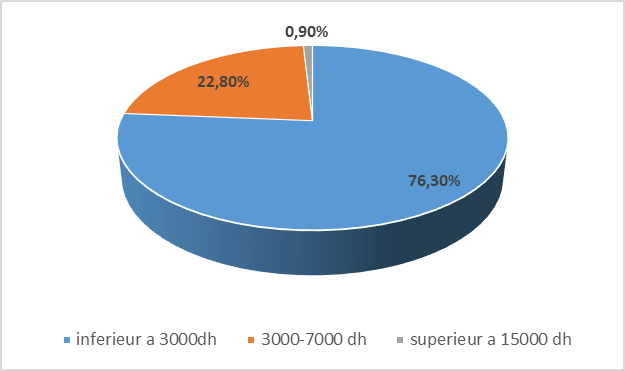
Figure 3. Distribution of patients according to income.
The level of education: patients without schooling were the most represented (34.7%) followed by patients with a primary level (31.7%), secondary (23.7%) then university (9.9%) cases.
The typical duration of consultations spanned over 3 years, ranging from as short as 1 month to as long as 24 months. The majority of patients (72%) initially seek advice from a traditional doctor.
Severity of the disorder (Figure 4): Most patients (55.5%) experienced moderate sexual impotence. Additionally, we observed other associated sexual disorders, including libido disorder in 3 patients, bending of the penis in 3 patients, premature ejaculation in 2 patients and lower urinary tract disorders in 10 patients.
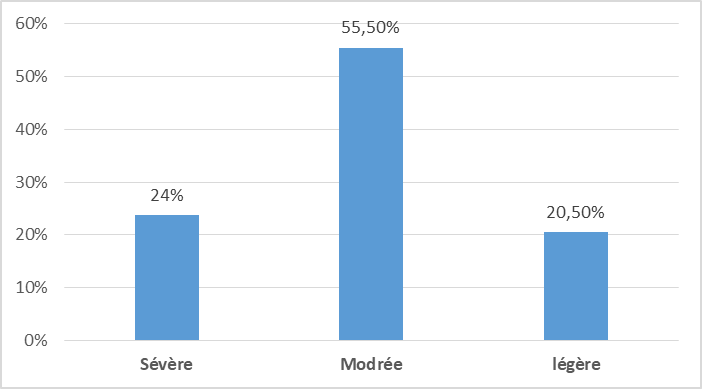
Figure 4. Distribution according to the severity of erectile dysfunction.
The course of the condition was severing in 28.7% and progressive in 71.3% of cases. Morning erections were preserved in 77.2%.
Triggering factor performance stress was noted among young people under 40.
Comorbidity factors were recorded: diabetes in 21 patients (20.8%), hypertension (14.9%) and ischemic heart disease in 6 patients (5.9%).
Previous histor (table 3): multiple sclerosis in a single patient, prostate cancer treated with radiohormonotherapy (6.9%), colorectal surgery (4.9%), spinal cord trauma in a single patient, femeropopliteal bypass surgery (1.9%), and coronary angioplasty in 5 patients (4.9 %).
Table 3. Comorbidities and history
|
Co-morbidities and history |
Number of patients |
Percentage |
|
Diabetes |
21 |
20.80% |
|
High blood pressure |
15 |
14.90% |
|
Ischemic heart disease |
6 |
5.90% |
|
multiple sclerosis |
1 |
0.90% |
|
Coronary angioplasty |
5 |
4.90% |
|
Prostate cancer under hormonal therapy and radiotherapy |
7 |
6.90% |
|
Colorectal surgery |
5 |
4.90% |
|
femeropopliteal bypass |
2 |
1.90% |
|
spinal cord injury |
1 |
0.90% |
Physical Examination: Most patients exhibited a normal clinical examination (73%). Other anomalies included penile curvature in 3 patients (2.9%), gynecomastia in 0.9% of cases, an enlarged prostate upon rectal examination in 19.8% of patients, testicular hypotrophy in 1.9%, and hydrocele in 0.9%.
Biological Findings: Hyperglycemia was observed in 21 patients (20.8%), elevated cholesterol levels in 10 patients (10%), and low testosterone levels in 2 patients.
Doppler Ultrasound Findings: Doppler ultrasound of the penis revealed decreased perfusion of the corpora cavernosa in 2 cases, with calcifications in the cavernous arteries. Additionally, thickening of the albuginea was noted in 3 patients with Peyronie's disease.
Impact on Married Patients: Marital conflict was the primary impact observed in 20 patients (27%), followed by divorce in 10 patients (13.7%). An unsatisfactory sexual relationship resulting in disappointment was noted in 10 female partners (13.7%), while 33 partners showed understanding.
DISCUSSION
The prevalence of erectile dysfunction (ED) varies widely across studies, ranging from (11%) to 44% according to Costa et al. [3] and 26% according to Nwaonu et al. [4]. Organic ED, found in 82% of our patients, appears to be the most common etiology.
Age
ED can affect young patients in their third and fourth decades of life, a population engaged in active sexual activity where even minor erectile dysfunction can be deeply distressing, perceived as a humiliation in front of their partner. Although numerous studies correlate ED with advancing age [5], primarily due to the accumulation of predisposing factors such as hypertension, diabetes, and dyslipidemia, our study found an average age of 55 years among patients.
Marital status
In our study, none of the patients were polygamous, which contrasts with findings from many African studies [4]. Polygamy is rare in Morocco due to strict cultural restrictions [6], unlike some African countries like Senegal and Mali. The occurrence of ED can lead to marital conflicts and psychological distress for the partner [7]. Diao et al [7] found a higher prevalence of polygamous relationships among patients with ED (29.2%), with the severity of ED increasing with the number of wives. In contrast, monogamous relationships represented (72.3%) of cases in our study.
Level of education
ED was found to be more prevalent among less educated men according to Johannes C et al. [8]. This observation is consistent with our study, where a significant proportion of patients without formal education were observed (34.7%). Lack of education may contribute to delayed consultation with a doctor, as patients may not recognize ED as a medical condition.
Professional situation
In our study, traders exhibited the highest frequency of ED (26.7%), followed by retirees (16.8%). The majority of patients had an income of less than 300 euros (76.3%). This contrasts with Senegalese studies where the prevalence of ED is higher among unemployed individuals [7].
The installation method and consultation time
The onset of ED was gradual in 71.3% of cases and abrupt in 28.7% in our study, with an average consultation time of 3 years ranging from 1 month to 24 months. This prolonged delay in seeking medical help can be attributed to patients initially consulting traditional healers, viewing ED as a taboo subject.
Preservation of morning erections and lifestyle habits
Morning erections were preserved in 77.2% of our patients, indicating a blend of psychogenic and organic factors contributing to ED. Tobacco use has long been associated with ED due to the vasoconstrictive effects of nicotine and certain free radicals [9,10]. Similarly, alcoholism is known to adversely affect penile vasculature, contributing to the high prevalence of ED in this population. In our study, smoking (72.3%), alcoholism (12%), and cannabis use (10%) were prevalent toxic habits among patients.
The severity of the disorder
In our study, a substantial portion of erectile dysfunction (ED) cases were classified as moderate (55.5%) according to the International Index of Erectile Function. These findings closely resemble those reported in the Egyptian series [11] and by Derby C et al. [12], but contrast with results from French [13] and American series [14], where the proportion of moderate cases was inversely proportional.
The variation in findings could be attributed to taboos surrounding sexual health, lack of awareness, and delayed consultation among our study population, factors that may not be as prevalent or impactful in other cultural contexts.
Other associated disorders
In our series, disorders of the lower urinary tract related to benign prostatic hypertrophy were the most prevalent, affecting 10 patients, followed by libido disorders in 3 patients, penile curvature in 3 patients, and premature ejaculation in 2 patients. These findings are consistent with the study by Diao et al. [7], which reported a decrease in libido in 47.1% of patients and premature ejaculation in 30.8% of patients. Additionally, Selvin et al. [15] found that 42.6% of patients with a history of prostatic hypertrophy presented with erectile dysfunction (ED). Other studies have also demonstrated a correlation between lower urinary tract disorders and ED [16,17].
Comorbidity factors
Erectile dysfunction (ED) has long been recognized as a potential indicator of cardiovascular disease [18]. High blood pressure is a prevalent risk factor for ED [19]. In the study conducted by Salomon et al. [20], 40% of patients hospitalized in cardiology presented with ED, with 30% of them diagnosed with coronary artery disease, which often necessitated delaying treatment for their ED. Peripheral neuropathy is proposed as a pathophysiological mechanism leading to ED [21]. Selvin et al. [15] reported that 42.6% of patients with ED had a history of diabetes, and 45.8% had not engaged in any physical activity during the 30 days preceding the onset of ED. In our series, comorbidities included diabetes in 21 patients (20.8%), hypertension in 14.9% of cases, and ischemic heart disease in 6 patients (5.9%).
Background
Trauma and pelvic surgery can lead to erectile dysfunction through nerve damage and hormonal imbalances such as hyperprolactinemia and hypotestosteronemia [22]. In our series, pelvic surgery was performed in 4.9% of cases, and 6.9% received radio-hormonotherapy treatment. Additionally, one case of spinal cord trauma was observed.
Implicating medication as a cause of erectile dysfunction (ED) can be challenging as it is often associated with comorbidity such as hypertension or diabetes. Among antihypertensive medications, beta blockers and thiazide diuretics are frequently implicated in the occurrence of ED due to their action in lowering blood pressure, which consequently reduces peripheral tissue perfusion [23].
On a biological level
Several authors have reported an association between hypercholesterolemia and erectile dysfunction (ED) [24]. The occurrence of ED in the presence of hypercholesterolemia is attributed to the development of endothelial dysfunction. Approximately 10% of our patients had hypercholesterolemia. In the study by Selvin et al. [15], 49.4% of patients were reported to have hypercholesterolemia.
Doppler ultrasound
Atherosclerosis of the pudendal arteries is more prevalent in patients with erectile dysfunction. According to Droupy, alterations in the function or structure of the cavernous artery endothelium are responsible for vascular-related ED [25]. Doppler ultrasound of the penis revealed reduced perfusion of the corpora cavernosa in 2 cases (1.9%) in our series, along with calcifications in the cavernous arteries. Additionally, thickening of the albuginea was observed in 3 patients (2.9%) with Peyronie's disease. This thickening is associated with pain and curvature, which can impede penetration [26].
CONCLUSION
Erectile dysfunction is a prevalent condition, yet it often remains a taboo topic for many of our patients. Despite its common occurrence, it can serve as a symptom indicating an underlying organic disease. However, it is often underestimated due to cultural modesty and reliance on traditional treatments. The epidemiological, clinical, and para-clinical characteristics of erectile dysfunction appear to be similar to those observed in other African countries. Therefore, it is imperative for healthcare providers to actively inquire about it during consultations, particularly in patients with chronic illnesses. Early detection and management can significantly improve patients' overall health and quality of life.
ACKNOWLEDGEMENTS
None.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interest.
REFERENCES
- Diallo Y, Coume M, Ze Ondo C, Diao B, Sylla C. (2012). Erectile dysfunction: epidemiological profile in a population of retired subjects in Senegal. Basic and Clinical Andrology. 22:241-245.
- Anaissie J, Hellstrom WJ. (2016). Clinical use of alprostadil topical cream in patients with erectile dysfunction: a review. Res Rep Urol. 8:123-131.
- Costa P, Avances C, Wagner L. (2003). Dysfonction érectile: connaissances, souhaits et attitudes. Résultats d'une enquête française réalisée auprès de 5.099 hommes âgés de 18 ans à 70 ans [Erectile dysfunction: knowledge, wishes and attitudes. Results of a French study of 5.099 men aged 17 to 70]. Prog Urol. 13(1):85-91.
- Nwakanma NC, Ofoedu JN. (2016). Depressive symptoms and marital adjustment among primary care patients with erectile dysfunction in Umuahia, Nigeria. S Afr J Psychiatr. 22(1):979.
- Fall Diop, F et al. (2013). Epidemiological profile of patients with erectile dysfunction at the Oua_kam health center, Dakar-Senegal. Med Afr Black. 60(11): 449-458.
- Rybalkina I. (2020). About the 2004 Family Code of the Kingdom of Morocco. Journal of the Institute for African Studies. DOI: 10.31132/2412-5717-2020-53-4-96-118.
- Diao B, Ndoye AK, Fall PA, Niang L. (2007). Erectile dysfunction in Senegal: epidemiological profile. Androl. 17(3):223-229.
- Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, McKinlay JB. (2000). Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts male aging study. J Urol. 163(2):460-463.
- Kovac JR, Labbate C, Ramasamy R, Tang D, Lipshultz LI. (2015). Effects of cigarette smoking on erectile dysfunction. Andrologia. 47(10):1087-1092.
- Biebel MG, Burnett AL, Sadeghi-Nejad H. (2016). Male Sexual Function and Smoking. Sex Med Rev. 4(4):366-375.
- Elbendary MA, El-Gamal OM, Salem KA. (2009). Analysis of risk factors for organic erectile dysfunction in Egyptian patients under the age of 40 years. J Androl. 30(5):520-524.
- Derby CA, Araujo AB, Johannes CB, Feldman HA, McKinlay JB. (2000). Measurement of erectile dysfunction in population-based studies: the use of a single question self-assessment in the Massachusetts Male Aging Study. Int J Impot Res. 12(4):197-204.
- Giuliano F, Chevret-Measson M, Tsatsaris A, Reitz C, Murino M, Thonneau P. (2002). Prévalence de l'insuffisance érectile en France: résultats d'une enquête épidémiologique menée auprès d'un échantillon représentatif de 1004 hommes [Prevalence of erectile dysfunction in France: results of an epidemiological survey conducted on a representative sample of 1004 men]. Prog Urol. 12(2):260-267.
- Moreira ED Jr, Lisboa Lôbo CF, Villa M, Nicolosi A, Glasser DB. (2002). Prevalence and correlates of erectile dysfunction in Salvador, northeastern Brazil: a population-based study. Int J Impot Res. 14(Suppl 2):S3-S9.
- Selvin E, Burnett AL, Platz EA. (2007). Prevalence and risk factors for erectile dysfunction in the US. Am J Med. 120(2):151-157.
- Khallouk A, Ahallal Y, Mellas S, Fadl Tazi M, Elfassi MJ, Farih MH. (2010). The erectile dysfunction associated with symptomatic benign prostatic hypertrophy (BPH): its link with the progressive stage of BPH, and its evolution under different therapeutics. 20:262-265.
- Richard F, Lukacs B, Jardin A, Lanson Y, Chevret-Measson M, Grange JC, Navratil H. (2001). Résultats d'une enquête épidémiologique menée chez des hommes âgés de 50 à 80 ans étudiant troubles mictionnels, qualité de vie et fonction sexuelle [Results of an epidemiologic surgery carried out with men 50-80 years of age to study urinary disorders, quality of life and sexual function]. Prog Urol. 11(2):250-263.
- Dubosq F, Lebret T, Guiomard A, Tainturier C, Botto H. (2006). Erectile dysfunction, an early marker of cardiovascular damage. Androl. 16(1): 24-27.
- Stephan D, Gaertner S, Bertrand C, Quelet J. (2008). Erectile dysfunction and antihypertensive treatment. Androl. 18(2):137-139.
- Solomon H, Man J, Wierzbicki AS, O'Brien T, Jackson G. (2003). Erectile dysfunction: cardiovascular risk and the role of the cardiologist. Int J Clin Pract. 57(2):96-99.
- El AY, Berraho M, Benslimane A, Chrit M, El Hassani H, Lyoussi B, et al. (2008). Diabète et dysfonction erectile au Maroc: etude epidémiologique auprès d'une population de consultants [Diabetes and erectile dysfunction in Morocco: epidemiological study among outpatients]. East Mediterr Health J. 14(5):1090-1100.
- Azemar MD, Menard J, Ripert T, Staerman F. (2009). Is the usual treatment regimen for erectile dysfunction suitable after age 65? Prog Urol. 19:202-208.
- Philipe F, Bondil P. (2006). Erectile dysfunction a new symptom for the cardiologist. Annal Cardiol and Angéolo. 55(4):187-189.
- Kambou T, Zaré C, Paré AK, Ouattara A, Somé YL, Sanon BG. (2014). Erectile Dysfunction among Diabetic Men in Two Medical Centers in Burkina Faso: Epidemiological, Diagnosis and Therapeutic Aspects. Advances in Sex Med. 4(1):1-5.
- Droupy S, Giuliano F, Cuzin B, Costa P, Vicaut E, Levrat F. (2009). Enquête Menée en Partenariat avec l'Association Française d'Urologie (AFU). Prévalence de la dysfonction érectile chez les patients consultant en urologie: l'enquête ENJEU (Enquête nationale de type 1 Jour sur la prévalence de la dysfonction Erectile chez des patients consultant en urologie) [Prevalence of erectile dysfunction in patients consulting urological clinics: the ENJEU survey (one day national survey on prevalence of male sexual dysfunction among men consulting urologists)]. Prog Urol. 19(11):830-838.
- Alenda O, Beley S, Ferhi K, Cour F, Chartier-Kastler E, Haertig A, et al. (2010). Physiopathologie et prise en charge de la maladie de La Peyronie [Pathophysiology and management of Peyronie's disease in adult patients: an update]. Prog Urol. 20(2):91-100.