Information Links
Related Conferences
Previous Issues Volume 7, Issue 1 - 2022
Effect of a Statewide Opioid Monitoring Program on a Community Emergency Department Opioid Prescribing Patterns
Nicole Caltabiano1, Ashley Keifer2, James Espinosa3, Alan Lucerna4, Nicholas Tomasello3, Russell Mordecai3, Henry Schuitema3, Victor Scali3
1Department of Emergency Medicine, Jefferson University, USA
2Department of Emergency Medicine, Emergency Medicine Residency Program, Rutgers Robert Wood Johnson, USA
3Department of Emergency Medicine, Rowan University, USA
4Program Director, Emergency Medicine, Rowan University, USA
Received Date: June 04, 2022
Published Date: July 08, 2022
*Corresponding Author: James Espinosa, Department of Emergency Medicine, Rowan University SOM/Jefferson - Stratford, NJ, USA, 18 East Laurel Road, Stratford, NJ 08084, Tel: 8563045101 E-mail: [email protected]
Citation: Caltabiano N, Keifer A, Espinosa J, Lucerna A, Tomasello N, Mordecai R, Schuitema H, Scali V. (2022). Effect of a Statewide Opioid Monitoring Program on a Community Emergency Department Opioid Prescribing Patterns. Mathews J Emergency Med. 7(1):43.
Copyright: Espinosa J, et al. © (2022).
ABSTRACT
Purpose of the Study: The purpose of this study was to determine if emergency physician’s opioid prescribing habits in three emergency departments of a three hospital community healthcare system changed following the revision of a state Prescription Monitoring Program (NJPMP). Materials and Methods: Design: A retrospective time series analysis Methods: A random sample of 50 days was be chosen from the year period prior to revised NJPMP) and a random sample of 50 days was chosen from the following two years. Data source: Retrospective data from an emergency department information system. Setting: Three campuses of a community emergency department system, with yearly visits to the ED in excess of 140,000. Inclusion Criteria: Retrospective, patients >18 years of age who present to the ED with pain and are prescribed opioid medication. Exclusion Criteria: Patients < 18 years of age, pregnant patients Data abstracted from EDIS was coded on entry into study and will thus had no unique identifiers. Variables: Percent opioid scripts written per given day (number of prescriptions/total adult patient volume) pre and post statewide prescription monitoring system. Average number of individual opioid pills written per prescription pre and post statewide prescription monitoring system. Average number of days’ supply of opioid prescription for each day ) pre and post statewide prescription monitoring system. Results: Opiate prescriptions written decreased from a mean of 35.14 (StDev 7.43) in the pre-intervention period to a mean of 21.70 (StDev 7.99) in the post intervention system. This difference was highly significant. ( p=0.001). The average number of pills prescribed decreased from a mean of 18.097 (StDev 2.245) in the pre-intervention period to a mean of 15.06 (StDev 3.101 in the post intervention period. This difference was highly significant (p< 0.001). The average number of day’s supply decreased from a mean of 4.512 (StDev 0.736) in the pre-intervention period to a mean of 3.845 (StDev 0.758 in the post intervention period. This difference was highly significant (p < 0.001). Discussion: There was a statistically significant decrease in all three measures when the pre-prescription monitoring program period and the post-prescription monitoring period were compared. This difference is evidence of a strong temporal relationship to the NJ-RX program, but does not prove causality. Other factors may have contributed. However, the temporal relationship is very statistically powerful and was certainly in the intended direction of effect of the reduction in opiate prescriptions. Conclusions: There was a statistically significant decrease in all three measures when the pre-prescription monitoring program period and the post-prescription monitoring period suggests that the monitoring system was likely causal.
Keywords: opiate prescribing patterns, emergency department opiate prescribing patterns
BACKGROUND
The lay press and academic literature have drawn attention an increase in prescription drug abuse, which has been referred to as an opioid epidemic. This has been noted to be the fastest-growing drug abuse problem in the United States (Cantrill, 2012).
Prescription drug abuse has become a major problem in the United States. In the year 2010, enough opioids were prescribed to treat every adult in the United States with 5 mg of hydrocodone every 4 hours for 1 full month (Jones, 2010). This rise in the prescription of opioids is paralleled with increasing rates of drug overdose deaths...as well as chronic, nonmedical use of opioids. In the United States, prescription drug overdose deaths outnumber those caused by motor vehicle accidents. This has been discussed as now being the single leading cause of “injury deaths” in the country (Int. Nar. Control, 2015).
With pain related injuries constituting the primary reason for emergency department visits, it is clear that emergency physicians must deal with this issue (Pletcher, 2008). Relieving pain and reducing suffering is without question a core element of the overall practice of emergency medicine. However, there is now, more than ever, a coexisting imperative to limit the harm that can result from prescription drug misuse (Cantrill, 2012).
In addition to legitimate painful conditions, emergency physicians frequently encounter patients who engage in illusive practices to obtain opiate medications. Physicians can attempt to identify patterns of substance abuse or rule out such patterns with the determination of a patient’s physical examination, medical history, and demeanor; however, this type of subjective data may lead to unwarranted conclusions and neglect of patient’s needs. (Baehren, 2010)
The United States must ensure that pharmaceuticals remain available for those with legitimate medical needs, while at the same time combatting the nation’s opioid epidemic, and this requires efforts of federal and state government agencies (Manchikanti,2005). Many regulations to monitor the prescription and distribution of legal drugs have been implemented over the past decade. For example, Prescription Drug Monitoring Programs have become a common in the United States. These are state...based monitoring programs for certain controlled substances that are prescribed by licensed practitioners and dispensed by pharmacies. Confirmation of a patient’s prescription history, in some cases, might prevent prescription of excess opioids to patients on a path toward developing substance abuse disorder, and in other cases, they might identify patients who are already abusing opioids and ‘doctor shopping’ (Stolbach, 2016). The objective information on potential misuse and abuse of prescription opioids can help physicians strike a balance between alleviating pain for patients and ensuring safe prescribing (Yuhaua, 2016).
The state of New Jersey has become increasingly aware of its place in prescription drug distribution and regulation. New Jersey’s drug related death toll has risen steadily from 843 deaths in 2010, to 1,026 deaths in 2011, and to 1,294 deaths in 2012. Approximately two-thirds of all those deaths involved prescription drugs rather than solely illicit drugs (NJ Gov, 2014). On November 1, 2015, Governor Chris Christie revised the scope and expanded the capabilities of the New Jersey Prescription Monitoring Program (NJPMP), which was initially established January 2012. (NJ Gov, 2014; NJ Att. Gen, 2 2015). These revisions required all prescribers with controlled dangerous substance registration to review prescription monitoring information before they prescribe a Schedule II (high abuse potential) medication to a new or current patient for pain, the first time they prescribe and quarterly thereafter (NJ Att. Gen, 2015). The new law also expanded the types of licensed professionals who are authorized to access the NJPMP for patient data and has increased the criminal penalties for inappropriate access and misuse of NJPMP data (NJ Att. Gen, 2015).
In order for states, regulatory agencies and organizations to make informed choices about policies and practices that will improve prescribing of opioids, further advancement in the evidence base is critical (Haegerich, 2014).
To our knowledge, there are no quantitative studies exploring the possible correlation between the revised prescription monitoring program and emergency physicians prescribing patterns.
OBJECTIVES
The objective of this study was to determine if emergency physician’s opioid prescribing habits (discharge prescriptions) at a 3site academic, community hospital in the state of New Jersey have changed following the revision of a Prescription Monitoring Program (NJPMP).
MATERIALS AND METHODS
Design: A retrospective time series analysis. Methods: A random sample of 50 days will be chosen from (period prior to revised NJPMP) and a random sample of 50 days will be chosen from the following two years. Data source: Retrospective data from an emergency department information system. Setting: Three campuses of a community emergency department system, with yearly visits to the ED in excess of 140,000. Inclusion Criteria: Retrospective, patients >18 years of age who present to the ED with pain and are prescribed opioid medication Exclusion Criteria: Patients < 18 years of age, pregnant patients Data abstracted from EDIS was coded on entry into study and will thus had no unique identifiers.
Variables:
1)Percent opioid scripts written per given day (number of prescriptions/total adult patient volume) pre and post statewide prescription monitoring system
2)Average number of individual opioid pills written per prescription pre and post statewide prescription monitoring system
3)Average number of days’ supply of opioid prescription for each day ) pre and post statewide prescription monitoring system
RESULTS
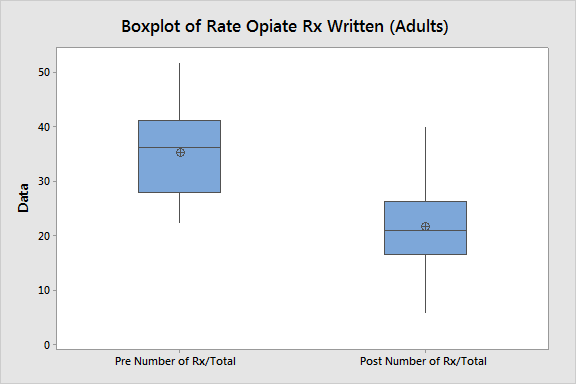
Rate Opiates Written
Opiate prescriptions decreased from a mean of 35.14 (StDev 7.43) in the preintervention period to a mean of 21.70 (StDev 7.99) in the post intervention system. This difference was highly significant. (p=0.001)
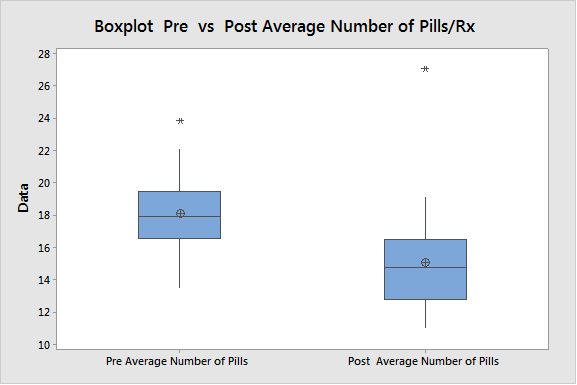
Rate Average Number Pills Per Prescription
The average number of pills prescribed decreased from a mean of 18.097 (StDev 2.245) in the pre-intervention period to a mean of 15.06 (StDev 3.101 in the post intervention period. This difference was highly significant (p< 0.001)
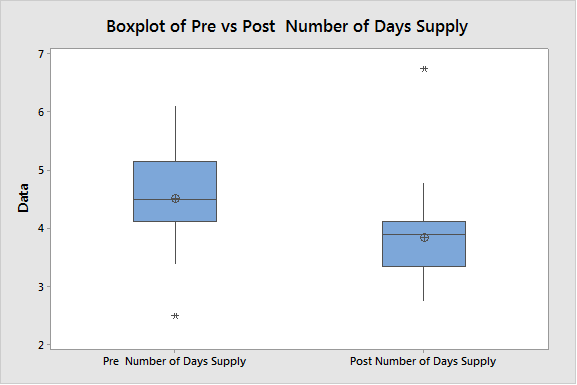
Rate Number of Days Supply Per Prescription
The average number of day’s supply decreased from a mean of 4.512 (StDev 0.736) in the pre-intervention period to a mean of 3.845 (StDev 0.758 in the post intervention period. This difference was highly significant (p < 0.001)
DISCUSSION
There was a statistically significant decrease in all three measures when the pre-prescription monitoring program period and the post-prescription monitoring period were compared. This difference is evidence of a strong temporal relationship to the NJ-RX program, but does not prove causality. Other factors may have contributed. However, the temporal relationship is very statistically powerful and was certainly in the intended direction of effect of the reduction in opiate prescriptions.
CONCLUSION
There was a statistically significant decrease in all three measures when the pre-NJRX and post-NJ RX systems of time were compared. This difference is evidence of a strong temporal relationship to the NJ-RX program, but does not prove causality. Other factors may have contributed. However, the temporal relationship is very statistically powerful and was certainly in the intended direction of effect of the reduction in opiate prescriptions.
REFERENCES
- Baehren DF, Marco CA, Droz DE, Sinha S, et al. (2010). A Statewide Prescription Monitoring Program Affects Emergency Department Prescribing Behaviors. Ann Emerg Med. 56(1); 19-23.
- Cantrill SV, Brown MD, Carlisle RJ, Delaney KA, Hays DP, et al. (2012). Clinical policy: critical issues in the prescribing of opioids for adult patients in the emergency department. Ann Emerg Med. 60(4): 499-525.
- Haegerich TM, Paulozzi LJ, Manns BJ, Jones CM. (2014). What we know, and don’t know, about the impact of state policy and systems-level interventions of prescription drug overdose. Drug and Alc Dep. 145;34-47.
- International Narcotics Control Board. (2015). Report of the International Narcotics Control Board for 2015. United Nations Publication. New York. 54.
- Jones CM, Mack KA, Paulozzi LJ. (2010). Pharmaceutical Overdose Deaths, United States. JAMA. 309:657-659.
- Manchikanti LM, Whitfield E, Pallone F. (2005). Evolution of the National All Schedules Prescription Electrionic Reporting Act (NASPER): A Public Law for balancing treatment of Pain and Drug Abuse and Diversion. Pain Physician. 8:335-347
- New Jersey Governor’s Council on Alcoholism and Drug Abuse. (2016). Confronting New Jersey’s Drug Problem: A Strategic Action Plan to Address a Burgeoning Heroin/Opiate Epidemic among Adolescents and Young Adults. 2014. Available at: www.gcada.nj.gov.
- New Jersey Office of the Attorney General. (2015) NJ Prescription Drug Monitoring Program. Available at: http://www.nj.gov/lps/ca2/pmp/.
- Pletcher MJ, Kertesz SG, Kohn MA, Gonzales R. (2008). Trends in Opioid Prescribing by Race/Ethnicity for Patients Seeking Care in US Emergency Departments. JAMA. 299(1);70-78
- Stolbach AI, Nelson LS. (2016). Choosing Opioid Policies our Patients Can Live With. Acad Emerg Med. 23(11): 1290-1292.
- Yuhaua Boa, Yijun Pan, Aryn Taylor, Radakrishnan S, Luo F. (2016). Prescription Drug Monitoring Programs are Associated with Sustained Reductions in Opioid Prescribing by Physicians. Health Affairs. 35(6): 1045-1051.