Information Links
Related Conferences
Previous Issues Volume 5, Issue 2 - 2020
Critical Skills Mannequin Training for Cricothyrotomy
Victor Scali1, James Espinosa2*
1Victor Scali DO Emergency Medicine Residency Academic Coordinator, Rowan University SOM/Jefferson - Stratford, NJ, USA
2James Espinosa MD, Department of Emergency Medicine, Rowan University SOM/Jefferson - Stratford, NJ, USA
*Corresponding Author: James Espinosa, Department of Emergency Medicine Rowan University SOM/Jefferson - Stratford, NJ, USA, 18 East Laurel Road, Stratford, NJ 08084, USA, E-mail: [email protected]
Received Date: November 05, 2020 Published Date: December 21, 2020 Copyright: Scali V, et al. © 2020. Citation: Scali V, et al. (2020). Does Computed Tomography of Kidney, Ureter and Bladder (CTKUB) affect the management of patients with suspected renal colic in Emergency Department?. Mathews J Emergency Med. (5)2:38.
ABSTRACT
The purpose of this study was to assess whether the low frequency/critically high skill set of cricothyrotomy can be taught to emergency medicine residents at various levels of training. Our study was prospective in design, involving a brief survey concerning years of training, prior experience with cricothyrotomy, sense of comfort with procedure and number witnessed. Participants were emergency medicine residents PGY 2-5. After the survey, participants watched a demonstration video. Cricothyrotomy was then performed by participants on a mannequin using a preassembled cricothyrotomy kit, up to a maximum of 10 attempts. Successful performance was defined as 40 seconds or less as per the training model of Wong et al. When participants were pooled by attempt, the overall reduction in time performance reached a plateau by the 5th attempt. This plateau is identical to the plateau described by Wong in his study of cricothyrotomy training in anesthesiologists. When success was operationally defined as less than or equal to 40 seconds per attempt, the success threshold was definitely reached by the 2nd attempt and reached a plateau by the 5th attempt. Statistical significance of less than p= 0.01 was reached by the second attempt and reached a plateau (p=0.001) by the 5th attempt.
Participants who reported 1 minimum previous experience with the procedure had a better performance than those who reports no previous experience with the procedure. [p=0.03] These differences became negligible by the 5th attempt. Participants who reported “very comfortable” had a better performance than those who stated “not comfortable”. [p=NS] “Not comfortable” participants had a better performance than those who stated “could do if needed.” [p=NS] These differences became negligible by the 5th attempt. Participants who reported three minimum previous procedures witnessed had a slower performance than those who reported 1 minimum previous procedure witnessed. [p=NS] Those with no previous procedures witnessed had a slower pooled time for the first attempt than those with more experience. [p=NS] These differences became negligible by the 5th attempt. This underscores that training up to the 5th attempt may be the most efficient model in future training work.
KEYWORDS: Cricothyroidotomy training; Cricothyroidotomy training and emergency medicine; Mannequin training for cricothyrotomy; Emergency medicine resident training and cricothyrotomy
INTRODUCTION
Cricothyrotomy is an infrequently performed procedure in the emergency department in the last 10 years since the introduction of Rapid Sequence Intubation, high tech airway adjuncts, and difficulty airway training. With the low frequency of cricothyrotomy performance in the emergency department, there is need to address training at least at the laboratory level with cadaver and/or mannequin training as a formal part of the teaching of the Core Competencies. The purpose of this study was to assess whether the low frequency/critically high skill set of cricothyrotomy can be taught to emergency medicine residents in the UMDNJ/SOM training program at various levels of training utilizing the teaching/assessment procedure developed by Dr. David T. Wong in his study of cricothyrotomy training in anesthesiologists [1].
In his study, Dr. Wong instituted a didactic training program utilizing the Seldinger cricothyrotomy technique, a demonstration video, a question/answer session and then a mannequin performance session utilizing the Melker cricothyrotomy kit by Cook Inc. An anatomically corrected standard cricothyrotomy mannequin supplied by Nasco, Fort Atkinson, Wisconsin, was used for the training session. All participants performed 10 consecutive procedures while being timed by a stopwatch. The procedure was considered successful is the cricothyrotomy was performed properly in 40 seconds or less. Dr. Wong concluded that mannequin training could produce success in the performance of the procedure after a minimum of five training attempts with a success rate of 96%. Success was measured as procedure times of less than 40 seconds. He concluded that mannequin training of cricothyrotomy is valuable and all providers of emergency airway management should be trained in this procedure. The purpose of this study was to look at this approach in emergency medicine residents.
MATERIALS AND METHODS
The study was prospective in design, involving a brief survey concerning years of training, prior experience with cricothyrotomy and a sense of comfort with procedure and number witnessed. Participants were emergency medicine residents PGY 2-5.
After the survey, participants watched a demonstration video. [Melker Demonstration Video (Video-C-VC-18; Cook, Inc.] There was a question and answer session followed by a hands-on session with a cricothyrotomy kit. [Melker Kit (C-TCCS-400; Cook, Inc.] Cricothyrotomy was then performed by participants on a mannequin [Cricothyrotomy Simulator #LF01082U; Nasco, Inc.] using preassembled Melker Kit up to a maximum of 10 attempts. Successful performance was defined as 40 seconds or less, as per the training model of Wong et al.
RESULTS
Number of Participants and Years of Training
There were 17 participants in the study group. The years of training ranged from 1 year to 4 years. The median in years of training was 3.
Prior Experience of Participants with Performance of Cricothyrtotomy
11 participants (65%) had no prior experience with the performance of a cricothyrotomy. The remaining 6 participants (35%) had 1 or more prior experiences with the performance of a cricothyrotomy.
Prior Experience of Participants with Witnessing of a Cricothyroidotomy
Eight participants (47%) had never witnessed a cricothyrotomy. The remaining 9 participants (53%) had witnessed one or more.
Pre-Intervention Self-Rating of Study Group Participants Concerning Comfort with Procedure
Eleven participants (65%) were self-rated as either comfortable or could do if needed. The remaining 6 participants (35%) were self-rated as not comfortable with the procedure.
Overall Time Performance (Participants Pooled) by Attempt
When participants were pooled by attempt, the overall reduction in time performance reached a plateau by the 5th attempt. [Table 1] This is visualized in a line chart. [Figure 1].
|
Attempt number |
||||||||||
|
Attempt (participants pooled) |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
|
Average time per attempt |
58.9 |
40.1 |
34.6 |
33.7 |
26.8 |
26.4 |
27.0 |
25.0 |
24.1 |
24.8 |
Table 1: Overall time performance (participants pooled) by attempt.
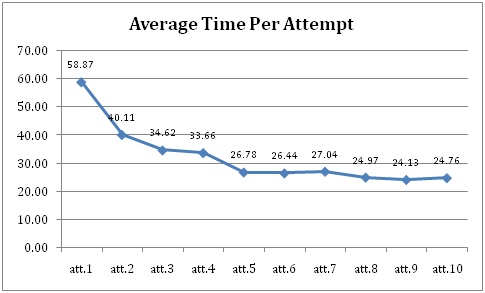
Figure 1: Line chart-- Overall time performance (participants pooled) by attempt.
Determination of Success Threshold (Wong Model)
When success was operationally defined as less than or equal to 40 seconds per attempt, the success threshold was definitely reached by the 2nd attempt and reached a plateau by the 5th attempt [Figure 2].
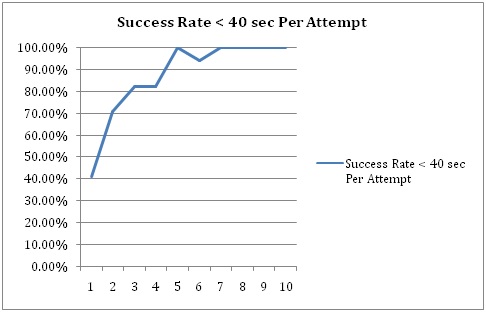
Figure 2: Determination of success threshold (Wong model).
Determination of Failure Threshold (Wong Model):
When failure was operationally defined as greater than or equal to 41 seconds per attempt, the failure plateau was crossed by the 2nd attempt and reached a plateau by the 5th attempt. [Figure 3].
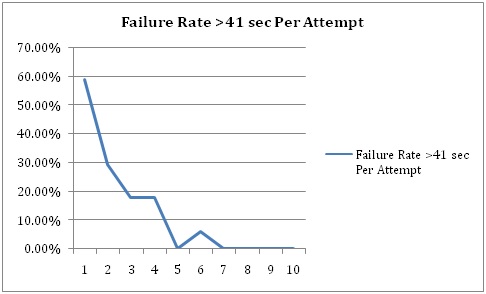
Figure 3: Determination of failure threshold (Wong model).
Statistical Significance: Attempt 1 Compared to Subsequent Attempts
Statistical significance of less than p= 0.01 was reached by the second attempt and reached a plateau (p=0.001) by the 5th attempt.
Performance by Attempts in relationship to pre-test self-reported comfort level
Participants who reported “very comfortable” had a better performance than those who stated “not comfortable”. [p=NS] “Not comfortable” participants had a better performance than those who stated “could do if needed.” [p=NS] These differences became negligible by the 5th attempt.
Performance by Attempts in relationship to number of times witnessed procedure
Participants who reported 3 minimum previous procedures witnessed had a slower performance than those who reported 1 minimum previous procedure witnessed. [p=NS] Those with no previous procedures witnessed had a slower pooled time for the first attempt than those with more experience. [p=NS] These differences became negligible by the 5th attempt.
Performance by Attempts in relationship to number of prior experiences with procedure
Participants who reported 1 minimum previous experience with the procedure had a better performance than those who reports no previous experience with the procedure. [p=0.03] These differences became negligible by the 5th attempt.
Performance by Attempts in relationship to number years training
Participants with one year of training had a lower level of performance than participants with two or more years of training. [p=NS] Participants in their second year had a better performance than third or fourth year residents. [p=NS] These differences became negligible by the 5th attempt.
DISCUSSION
There were 17 participants in the study group. The years of training ranged from one to four years. The median in years of training was 3. This appears to be representative of a residency training program in emergency medicine.
Eleven participants (65%) had no prior experience with the performance of a cricothyrotomy. The remaining six participants (35%) had 1 or more prior experiences with the performance of a cricothyrotomy. The nature of the previous experiences was not an element of the study. 8 participants (47%) had never witnessed a cricothyrotomy. The remaining 9 participants (53%) had witnessed one or more. In Wong’s study of cricothyroidotomy training with anesthesiologists, 51% had prior experience [1].
Eleven participants (65%) were self-rated as either comfortable or could do if needed. The remaining 6 participants (35%) were self-rated as not comfortable with the procedure. No comparison data was found in the literature concerning degree of comfort with cricothyrotomy prior to mannequin training.
When participants were pooled by attempt, the overall reduction in time performance reached a plateau by the 5th attempt. This plateau is identical to the plateau described by Wong in his study of cricothyrotomy training in anesthesiologists.
When success was operationally defined as less than or equal to 40 seconds per attempt, as per the method of Wong et al, the success threshold was reached by the 2nd attempt and reached a plateau by the 5th attempt. Wong found an identical plateau by the 5th attempt in his study cricothyrotomy training in anesthesiologists.
When failure was operationally defined as greater than or equal to 41 seconds per attempt, as per the method of Wong et al, the failure plateau was crossed by the 2nd attempt and reached a plateau by the 5th attempt.
Statistical significance of less than p= 0.01 was reached by the second attempt and reached a plateau (p=0.001) by the 5th attempt.
Participants who reported 1 minimum previous experience with the procedure had a better performance than those who reports no previous experience with the procedure. [p=0.03] These differences became negligible by the 5th attempt. This finding may have implications in retraining work as well as in testing of retention of skills.
Participants who reported “very comfortable” had a better performance than those who stated “not comfortable”. [p=NS] “Not comfortable” participants had a better performance than those who stated “could do if needed.” [p=NS] These differences became negligible by the 5th attempt.
Participants who reported three minimum previous procedures witnessed had a slower performance than those who reported 1 minimum previous procedure witnessed. [p=NS] Those with no previous procedures witnessed had a slower pooled time for the first attempt than those with more experience. [p=NS] These differences became negligible by the 5th attempt.
Participants with one year of training had a lower level of performance than participants with two or more years of training. [p=NS] Participants in their second year had a better performance than third or fourth year residents. [p=NS] These differences became negligible by the 5th attempt.
LIMITATIONS OF THE STUDY
The sample size was relatively small. However, the effect size of the training was such that statistical significance was seen in several aspects of the study (first attempt to subsequent attempts, relationship of previous experience to performance, attempts to plateau at five attempts).
There is no comparison made to other methods of training. Cadaver models have been used in cricothyrotomy training [2]. Time to success data was not published in Breitmeier’s study. Aboud et al describe cadaver training with what are called “live cadavers”—a model in which cannulation of vessels, blood reservoir use and an intra-aortic pump is used to simulate live conditions. Only five such models were prepared [3]. Porcine models have been used [4]. However, Iverson et al found no objective training advantage of animal model training over simulation training using models [5]. A similar conclusion was reached by Hall et al [6]. Virtual reality simulation has been used in teaching surgical skills. Hence, the use of simulation mannequins appears to be quite reasonable in such training. Outcomes in actual cricothyroidotomy practice were not studied.
CONCLUSIONS
Cricothyrotomy is an infrequently performed procedure in the emergency department. With the low frequency of cricothyrotomy performance in the emergency department, there is need to address training at least at the laboratory level with cadaver and/or mannequin training as a formal part of the teaching of the Core Competencies.
The purpose of this study was to assess whether the low frequency/critically high skill set of cricothyrotomy can be taught to emergency medicine residents at various levels of training utilizing the teaching/assessment procedure developed by Dr. David T. Wong in his study of cricothyrotomy training in anesthesiologists. In this study of emergency residents, when success was operationally defined as less than or equal to 40 seconds per attempt, the success threshold was definitely reached by the 2nd attempt and reached a plateau by the 5th attempt.. Statistical significance of less than p= 0.01 was reached by the second attempt and reached a plateau (p=0.001) by the 5th attempt. This plateau is identical to the plateau described by Wong in his study of cricothyrotomy training in anesthesiologists. Participants who reported 1 minimum previous experience with the procedure had a better performance than those who reports no previous experience with the procedure. [p=0.03] These differences became negligible by the 5th attempt. This finding may have implications in retraining work as well as in testing of retention of skills.
REFERENCES
- Wong DT, Prabhu AJ, Coloma M, Imasogie N, Chung FF. (2003). What is the minimum training required for successful cricothyroidotomy?: a study in mannequins. Anesthesiology. 98(2):349-53.
- Breitmeier D, Schulz Y, Wilke N, Albrecht K, Haeseler G, et al. (2004). Piepenbrock S. Cricothyroidotomy training on cadavers - experiences in the education of medical students, anaesthetists, and emergency physicians. Anasthesiol Intensivmed Notfallmed Schmerzther. 39(2):94-100.
- Aboud ET, Aboud G, Aboud T. (2015). "Live cadavers" for practicing airway management. Mil Med. 180(3 Suppl):165-70. doi: 10.7205/MILMED-D-14-00396.
- Netto FA, Zacharias P, Cipriani RF, Constantino Mde M, Cardoso M, et al. (2015). A porcine model for teaching surgical cricothyroidotomy. Rev Col Bras Cir. 42(3):193-6. doi: 10.1590/0100-69912015003012.
- Iverson K, Riojas R, Sharon D, Hall AB. (2015). Objective comparison of animal training versus artificial simulation for initial cricothyroidotomy training. Am Surg. 81(5):515-8.
- Hall AB. (2011). Randomized objective comparison of live tissue training versus simulators for emergency procedures. Am Surg. 77(5):561-5.