Information Links
Related Conferences
Previous Issues Volume 8, Issue 1 - 2024
Corono-Radicular Restoration Using Fragment Bonding: An Esthetic Option for Managing Fractured Lateral Incisor
Amira Kikly1, Sabra Jaâfoura2, Afif Bouslema3, Yasmine Neifer4, AmeniChadlia Belghith5, Neila Zokkar6, Nabiha Douki6,*
1Associate Professor, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
2Associate Professor, Department of Dental Biomaterials, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Laboratory of Dento-Facial, Clinical and Biological Approach (ABCDF) LR12ES10, University of Monastir, Tunisia
3Assistant, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
4Laboratory of Dento-Facial, Clinical and Biological Approach (ABCDF) LR12ES10, University of Monastir, Tunisia
5Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
6Professor, Department of Dentistry, University Hospital, Sahloul, Tunisia, Faculty of Dental Medicine, University of Monastir, Avicenna Street, 5000 Tunisia, and Research Laboratory LR12ES11, University of Monastir, Tunisia
*Corresponding Author: Nabiha Douki, University of Monastir, Dental Faculty of Monastir, Research Laboratory LR12ES11, Department of Dentistry, University Hospital, Sahloul, Tunisia, E-mail: [email protected].
Received Date: January 25, 2024
Published Date: February 06, 2024
Citation: Kikly A, et al. (2024). Corono-Radicular Restoration Using Fragment Bonding: An Esthetic Option for Managing Fractured Lateral Incisor. Mathews J Dentistry. 8(1):42.
Copyrights: Kikly A, et al. © (2024).
ABSTRACT
Oral trauma is common in both children and adults. Different clinical forms are encountered, requiring the clinician to make a correct diagnosis and provide rapid and effective treatment to preserve the vital and/or functional prognosis of the tooth. In the case of a coronal fracture, the bonding of the tooth fragment is a therapeutic procedure that is particularly advantageous from an aesthetic point of view, ensuring better preservation of the tooth's physical and chemical characteristics. This technique is simple and economic. It can be a replacement for the time-consuming procedures of conventional corono-radicular reconstruction. The main aim is to restore function and aesthetics, while retaining the original morphology, color and texture. Using a clinical case study, this paper illustrates the steps involved in the corono-radicular restoration of a fractured tooth by fragment bonding, and discusses the factors that play a role in the therapeutic decision, highlighting the essential points that determine the success of this technique.
Keywords: Dental Trauma, Reattachment, Bonding, Tooth Fragment, Dual Resin.
INTRODUCTION
Coronal fractures are common in our daily practice and represent the most common accident to permanent incisors, but few of us bring back the fractured fragment. These types of fractures are usually restored with a composite.
Today, the trend towards less invasive dentistry, combined with continuing progress in the field of adhesive dentistry, opens up new perspectives for restoring this type of fracture. In fact, in complex fractures where the tooth fragment is salvaged and can be coapted to the remaining tooth structure, endodontic treatment followed by reattachment of the fragment with a fibre-reinforced post is a valid and successful option. It is a simple conservative treatment that restores the tooth's natural shape, color, surface texture and occlusal alignment, giving the patient a positive psychological response by preserving their own tooth structure [1,2]. However, the success of this technique depends on several factors that influence the prognosis of these teeth. These included factors relating to the tooth, the tooth fragment itself, the preparation technique and the materials used [3,4].
The aim of this paper is to describe in detail, based on a clinical case, a corono-radicular restoration of a fractured tooth, to discuss factors involved in our therapeutic decision and to highlight key factors for success.
CASE REPORT
This is the case of a 13-year-old patient with a traumatic oral injury who was referred to the Department of Dental Medicine at the Sahloul Hospital in Tunisia. Endo-buccal clinical examination revealed total intrusion of the right maxillary central incisor (11) and a complex fracture of the right maxillary lateral incisor (12) down to the 1/3 cervical root with a mobile fragment (Figure 1). The surgical repositioning of the central incisor (11) was performed. The tooth fragment of the lateral incisor (12) was preserved in saline. A semi-rigid splint was applied from the right upper canine tooth to the left upper canine tooth (Figure 2). Endodontic treatment was performed on 11 and 12 (Figure 3). A palatal (subgingival margin) gingivectomy was then performed (Figures 4-6), followed by bonding of the fragment to 12 with a fiber-reinforced post. The first step was to prepare the post housing by disobturating the coronal 2/3 of the root canal (Figure 7), etching the housing for 20 seconds with orthophosphoric acid (Figure 8), applying adhesive and light-curing (Figure 9). The post was then prepared by applying adhesive and light curing (Figure 10). The post was bonded with dual resin (Figure 11). A groove was created in the coronal fragment to receive the post head. After application of the amelo-dentinal adhesive system (Figure 12), the tooth fragment was inserted along the axis of the post and bonded with dual resin, with any excess removed. A defect was observed at the cervical level (Figure 13). This defect was finally restored with composite resin using a layering technique (Figure 14).
.png)
Figure 1. Preoperative clinical view showing total intrusion of the right maxillary central incisor (11) and a complex fracture of the right maxillary lateral incisor (12).
.png)
Figure 2. Splinting of Traumatized Teeth.
.png)
Figure 3. Retroalveolar radiograph following endodontic treatment of 11 and 12.
.png)
Figure 4. Occlusal view of the cervical limit of the fracture on 12.
.png)
Figure 5. Gingivectomy.
.png)
Figure 6. Clinical view after healing.
.png)
Figure 7. Disobturation of the coronal 2/3 of the root canal.
.png)
Figure 8. Etching the housing for 20 seconds with orthophosphoric acid.
.png)
Figure 9. Applying adhesive to post housing and light-curing

Figure 10. Applying adhesive to the post and light-curing

Figure 11. Injection of dual resin into the post housing, placement of the post and light curing.
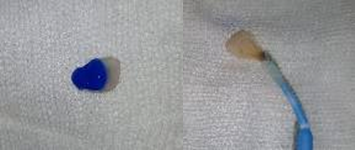
Figure 12. Etching of the tooth fragment with orthophosphoric acid, application of the adhesive and light curing.

Figure 13. After removing excess dual resin: lack of resin in the cervical area.
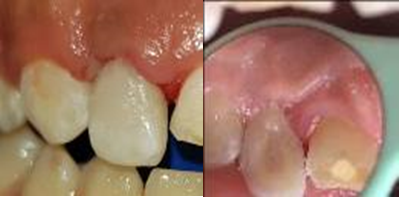
Figure 14. Final result after restoring the cervical area using composite.
DISCUSSION
Reattachment of fragments of fractured teeth offers several advantages; it is a conservative, safe and simple treatment that restores both the aesthetics and function of the natural tooth with less chair time, thus reducing the cost of treatment. The success of this technique depends on several factors that affect the prognosis of these teeth. These factors include those related to the tooth, the tooth fragment itself, the preparation technique and the materials used.
It has been shown that the extent of the coronal fracture determines fragment retention and, consequently, the reattachment technique. In our case, the fracture involves 2/3 of the coronal height of the tooth. The line of fracture must be a long way from the occlusal contact. Repeated contact generates torsional forces that can destabilize the fragment. Thus, any harmful occlusal contact with the antagonist tooth must be eliminated before reattaching the tooth fragment.
With regard to the tooth fragment, it is recommended to check its integrity first. It needs to be intact and fit well with the remaining tooth. The coronal fragment should be preserved in an appropriate hydrated medium (saline, water, saliva). This medium hydrates the tooth fragment to maintain its original aesthetics and optimise bonding. The prognosis of fractured teeth has been shown to be improved by coronal fragment preparation [5]. Indeed, additional preparation of the coronal fragment prior to reattachment offers greater resistance to fracture than simple bonding without preparation. The preparation methods mentioned include bevelling the tooth fragment and dental crown, grooving the internal dentin, external chamfering and the overcontouring technique. There are advantages and disadvantages to each of these techniques [6,7].
Bonding using the external chamfer technique involves making a small, 1 mm deep preparation of the enamel on the tooth and fragment surface, using a diamond bur with a rounded tip. [8] In the internal groove technique, a groove 1 mm deep and 1 mm wide is prepared on the internal surface at the level of the tooth fragment and at the level of the fractured tooth, and the bonding material is applied to both surfaces and into the groove. The groove also allows excess adhesive to drain away [6].
Particular attention must be paid to the violation of the biological space in the case of subgingival extension of the fracture line, which justifies the gingivectomy performed in our case. The overcontouring technique corresponds to the reattachment of the coronal fragment using the simple technique. A saucer-shaped cavity with a depth of 0.5 mm is then prepared at the fracture line with a diamond ball bur. This cavity is then filled with composite resin. This technique can contribute to the durability of the restoration. Whichever technique is used, occlusal control and a finishing step are necessary to achieve a good surface finish and satisfactory esthetics [8,9].
In terms of longevity, coronal fragment reattachment has been the subject of several studies evaluating its fracture resistance. Simple reattachment of the fragment without preparation was shown to provide only 37.1% more fracture resistance than an intact tooth. The external chamfer technique provides 60.6% fracture resistance, while the overcontour and internal groove techniques provide 97.2 and 90.5% resistance respectively. In light of these results, it is clear that the effectiveness of tooth fragment bonding depends on the preparation technique [7,10].
The use of a post was necessary to ensure good retention and to protect the tooth fragment from torsional forces. The choice of a fibre-reinforced post is justified by its ability to offer high strength, a good aesthetic result, good bonding capacity and, lastly, a modulus of elasticity close to that of dentin, which allows a harmonious distribution of forces and thus avoids any risk of root fracture. Some authors recommend surface treatment of fibre-reinforced posts to increase their retention by silanisation, ethanol pretreatment, air abrasion or phosphoric acid.
The preparation of the post housing is a very important step in receiving the fibre-reinforced post, which must be at least as long as the coronal height. Stress is distributed over a smaller surface area and the prognosis for the fractured tooth is considered unfavourable if the post is shorter than the clinical crown height. The extra-radicular portion must allow good retention of the coronal fragment [11].
Endodontic retreatment must not interfere with apical sealing. It is therefore recommended to leave 5 mm of gutta percha apically, with 3 mm being the absolute minimum. The axis of the forest should be that of the tooth to avoid misalignment.
Today, with the advent of new generations of dentin bonding agents and adhesive materials, reattachment of fractured fragments has become a reliable treatment option. In terms of adhesive systems, those using orthophosphoric acid as a conditioner are the most recommended and offer a better long-term seal, whereas the use of self-etching adhesives on intact enamel is not recommended due to their weaker bond strength [12-14].
The addition of a bonding agent between the two dental structures enhances bond strength and resistance. Several products have been used (glass ionomer cements, resin-modified glass ionomer cements, compomer, composite resin, dual resin), but composite resin-based products are the best in terms of longevity and esthetics. In fact, the highest fracture toughness was observed with composite resin and the lowest with resin-modified glass ionomer cement. It is possible to optimise the restoration in the face of a slight defect, and the esthetics can be perfected with a composite resin restoration.
The occlusion must not interfere with the fracture line, as shearing forces may destabilise the tooth fragment. In this case, an occlusal adjustment should be made [6,8].
CONCLUSION
Coronal fragment bonding saves a lot of time. The procedure is carried out in a single session, preserves dental tissue, provides immediate aesthetic results, improved aesthetic quality, perfect translucency, an incisal edge similar to that of the adjacent teeth, good morphology with the best possible colour, sufficient durability over time, the possibility of re-intervention in the event of problems, and the possibility of postponing conventional prosthetic restorations.
CONFLICTS OF INTEREST
The authors declare no conflict of interest.
DATA AVAILABILITY STATEMENT
The data presented in this study are available on request from the corresponding author.
REFERENCES
- Khandelwal P, Srinivasan S, Arul B, Natanasabapathy V. (2021). Fragment reattachment after complicated crown-root fractures of anterior teeth: A systematic review. Dent Traumatol. 37(1):37-52.
- Gunwal MK, Bagda K, Gupta S, Oak AM. (2021). Knowledge, awareness and perception amongst dental practitioners towards natural tooth fragment reattachment procedures in clinical practice-A cross-sectional survey. Dent Traumatol. 37(6):779-785.
- Arias Z, Falú Hinojosa Ledezma H, Patricia Osorio Terán C, Omori K, Yamamoto T, Zahedul Islam Nizami M, et al. (2023). Reattachment of Fractured Tooth Fragment by Multidisciplinary Treatment Approach. Bull Tokyo Dent Coll. 64(1):13-22.
- Vishwanath B, Faizudin U, Jayadev M, Shravani S. (2013). Reattachment of Coronal Tooth Fragment: Regaining Back to Normal. Hindawi Publish Corporat. 5:186-191.
- Brasil Maia G, Pereira RV, Poubel DLDN, Almeida JCF, Dias Ribeiro AP, Rezende LVML, et al. (2020). Reattachment of fractured teeth using a multimode adhesive: Effect of different rewetting solutions and immersion time. Dent Traumatol. 36(1):51-57.
- Pusman E, Cehreli ZC, Altay N, Unver B, Saracbasi O, Ozgun G. (2010). Fracture resistance of tooth fragment reattachment: effects of different preparation techniques and adhesive materials. Dental Traumatol. 26(1):9-15.
- Macedo GV, Diaz PI, De O Fernandes CA, Ritter AV. (2008). Reattachment of anterior teeth fragments: a conservative approach. J Esthet Restor Dent. 20(1):5-18.
- Abdulkhayum A, Munjal S. (2014). In vitro evaluation of fracture strength recovery of reattached anterior fractured tooth fragment using different reattachment techniques. J Clin Diagn Res. 8(3):208-211.
- Charland R, Mackay P, Mercier R, Shoghikian E, Aubre N, Gagnon S, et al. (2007). Traumatismes des dents antérieures permanentes: Fractures coronaires. J Ordre dent Québec. 44:63-68.
- AlQhtani FA. (2020). Reattachment of a Dehydrated Tooth Fragment Using Retentive Holes. Cureus. 12(1):e6640.
- Aggarwal S, Sahoo SR, Pandharkar K. (2014). Corono-radicular biological restoration of maxillary central incisors by direct method. Dent Res J (Isfahan). 11(6):695-659.
- Gurtu A, Roy S, Chandra P, Bansal R. (2019). Reattachment of complex fractures; a reality by advances in self-etch bonding systems. Indian J Dent Res. 30(1):135-139.
- Erhardt MC, Cavalcante LM, Pimenta LA. (2004). Influence of phosphoric acid pretreatment on self-etching bond strengths. J Esthet Restor Dent. 16(1):33-40.
- Van Landuyt KL, Kanumilli P, De Munck J, Peumans M. (2006). Bond strength of a mild self-etch adhesive with and without prior acid-etching. J Dent. 34(1):77-85.