Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2023
Comparison of Acetabular Cup Positioning In Total Hip Arthroplasty: Direct Lateral VS Posterior Approach
Adeel Hamid1, Usman Gill1,*, Mian Hanif2
1Consultant Lahore General Hospital, Pakistan
2Head of Department of Orthopedics, Lahore General Hospital, Pakistan
*Corresponding Author: Usman Gill, Consultant Lahore General Hospital, Pakistan; Email: [email protected]
Received Date: July 27, 2023
Publication Date: August 22, 2023
Citation: Hamid A, et al. (2023). Comparison of Acetabular Cup Positioning In Total Hip Arthroplasty: Direct Lateral VS Posterior Approach. Orthop Res J. 5(1):26.
Copyright : Hamid A, et al. © (2023)
INTRODUCTION
Total hip arthroplasty is one of the most successful operations in orthopedic surgery with regards to patient out-come [1-3]. Proper component placement is one of the fundamental factors to achieve good results and avoid complications. Suboptimal component positioning particularly that of the acetabular cup has been associated with poor outcomes and complications including dislocation, increased wear, impingement, component loosening, and limp [2,4-7].
Various surgical approaches have been used to perform total hip arthroplasty. Two of the most commonly used surgical approaches are the Direct lateral (Hardinge) and Posterior (Moore’s) approach [8-11]. Proponents of each have cited advantages of each surgical approach. Orientation of the anatomical landmarks and exposure of proximal femur and acetabulum varies with the approach which may potentially effect the component positioning [4,12,13] Varying clinical outcomes and incidence of complications have been reported with these two surgical approaches [14-16]. Therefore, it is important to investigate if the difference in component positioning, if any, is the cause of difference in results.
The aim of this retrospective study was to compare the acetabular cup positioning UN terms of cup inclination and anteversion in various patients who had undergone THA by direct lateral and posterior approaches.
METHODS
This study was carried out at the Department of Orthopedic and spine surgery at Lahore general hospital, Lahore Pakistan. We conducted a retrospective study identifying 25 patients who had undergone THA by direct lateral and 25 patients who had undergone the same procedure by posterior approach. The patients were operated in between 2018-2020.
Inclusion Criteria
Patients of all ages undergoing primary THA due to NOF fracture. Hip OA, AVN, post traumatic arthritis and DDH
Exclusion Criteria
Patients undergoing revision THA or reconstruction for pathological fracture due to mets, pts with fixed spino-pelvic deformities identified on routine preoperative workup.
Patients with sub optimal x-rays which made measurement of required angles difficult were also excluded.
All surgeries were carried out by the same senior consultant adept in both approaches due to high volume pelvic/acetabular trauma. The surgeon aimed to place the cups within the ‘safe zone’ in each case. The choice of surgical approach was determined by various factors including previous surgical scar, abductor muscle strength, BMI of pt etc.
Surgeries included both cemented and uncemented acetabular components depending on the the relevant indications. Anatomical landmarks (transverse acetabular ligament and acetabular margin) were used to guide cup positioning. Navigation was not used.
Standard Post-operative x-rays (AP and lateral views) were scrutinised to check the acetabular cup positioning. The angles of anteversion and inclination were drawn and measured by the author in consultation with radiologist. The safe zone described by Lewwinik, et al. [2] i.e inclination of 40 degrees +/- 10 and anteversion of 15 degrees +/- 10 was used to check adequacy of cup placement. We calculated how many patients from each group the acetabular cups had placed in Lewwineck’s safe zone.
RADIOLOGICAL EVALUATION
All X-rays were taken in the radiology department of Lahore general hospital using a standardized protocol. Post-operative X-ray pelvis with both hips AP view was used to measure the angle of inclination of the acetabular cup, taking line passing through the inferior most part of obturator foramen as horizontal. Second line was drawn thought the long axis of the ellipses on the cup. The angle between these two lines showed the angle of inclination.
Cross table lateral X-rays were used to measure the angle of anteversion. Using the method described by Woo and Morey [17], version was taken as the angle between the line touching the open surface of acetabular cup and a line perpendicular to the table.
RESULTS
50 patients were placed in two groups; PA (posterior approach group) and LA (lateral approach group). The results are shown as follows:
|
Age |
Male/Female |
Right/Left hip |
Cup inclination |
Cup anteversion |
In safe zone |
|
|
PA group |
60.16 years |
17/8 |
14-Nov |
37.08 |
22.32 |
19 |
|
LA group |
57.4 years |
16/9 |
16-Sep |
39.52 |
18.4 |
21 |
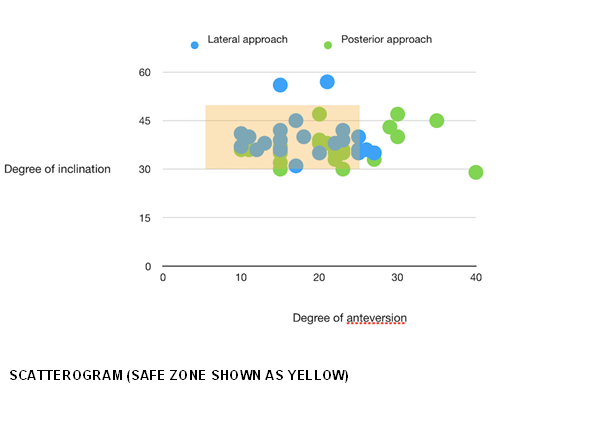
The cup inclination in the PA group ranged from 29-47 degrees whereas the inclination in the LA group ranged from 31-57 degrees. On average the cup was placed in more inclination in the LA group (39.52 vs 37.08 degrees, p value 0.12). The anteversion of the cup in PA group was found to between 10-40 degrees where as in the LA group; 10-27 degrees. So the surgeon tended to place the cup in more anteversion (average 22.32 vs 18.40, p value 0.04) in the PA group. The means for angle of inclination and anteversion were compared using Unpaired student’s t test and p value was found to be significant i.e; <0.05 for anteversion but insignificant for inclination.
The orientation of the acetabular component corresponded to Lewinnek’s safe zone in 19 patients from the PA group and 21 patients from the LA group.
DISCUSSION
The article presents a retrospective study comparing the acetabular cup positioning in patients who underwent total hip arthroplasty (THA) using the direct lateral and posterior approaches. The study aimed to investigate if there were differences in component positioning between the two surgical approaches and if these differences could potentially affect outcomes and complications.
It has been observed that different approaches offer a different view and orientation of the anatomical landmarks [9-11] PA has been postulated to offer a better view of the proximal femur whereas the LA offers a better and complete view of the acetabulum [8,17,19]. Also, historically PA has shown slightly greater chances of dislocation after THA as compared to LA [20,21].
The results of the study showed that there were indeed differences in cup positioning between the two groups. The angle of inclination in the LA averaged slightly more that PA group by 1.5 degrees with a much wider range (31-57 degrees). However these findings were not statistically significant. The angle of anteversion averaged a significant 4 degrees more in the PA group compared to the LA group with a p-value of <0.05. The greater anteversion seen in the PA group could be related to the surgeons subconscious attempt to minimize the chances of post-operative dislocation of the hip [22] components in the LA group were placed in the safe zone compared to 19 in PA group.
The study findings support previous research that has shown differences in cup placement between the direct lateral and posterior approaches. Studies by and Kruse, et al. [13], which was a randomized control trial comparing the two approaches and by Callanan, et al. [12,24,25], based on evaluation of 1823 hips, showed the same difference in cup placement between the PA and LA.
It is important to note that both groups in this study had their cup placements within the "safe zone" as described by Lewinnek, et al. [4]. However, the PA group had a slightly lower percentage of cups placed in the safe zone compared to the LA group. This indicates that the LA approach may offer better visualization of the acetabulum, allowing for more precise cup positioning within the safe zone.
While the differences in cup positioning were statistically significant, it is unclear if these differences have any clinical impact on hip function, wear rate, or dislocation risk. The study did not assess these clinical outcomes, and further research is needed to determine if the observed radiographic differences translate into meaningful differences in patient outcomes.
The study has some limitations that should be considered. Firstly, it was a retrospective study with a relatively small sample size. A larger sample size and prospective study design could provide more robust results. Secondly, the study was conducted by a single senior consultant, which may limit the generalizability of the findings. It would be beneficial to include multiple surgeons to assess if the differences in cup positioning persist across different practitioners.
In conclusion, this study adds to the existing body of knowledge regarding the differences in cup positioning be-tween the direct lateral and posterior approaches in THA. The findings suggest that the choice of surgical approach may influence component positioning, particularly in terms of cup anteversion [17,19-21]. Further research is needed to assess the clinical implications of these differences and to determine the impact on patient outcomes and complications associated with THA.
REFERENCES
- Jolles BM, Zangger P, Leyvraz PF. (2002). Factors predisposing to dislocation after primary total hip arthroplasty: a multivariate analysis. J Arthroplasty. 17(3):282–288.
- Seagrave KG, Troelsen A, Malchau H, Husted H, Gromov K. (2017). Acetabular cup position and risk of disloca- tion in primary total hip arthroplasty. Acta Orthop. 88(1):10–17.
- Kennedy JG, Rogers WB, Soffe KE, Sullivan RJ, Griffen DG, Sheehan LJ. (1998). Effect of acetabular compo- nent orientation on recurrent dislocation, pelvic osteolysis, polyethylene wear, and component migration. J Arthroplasty. 13(5):530–534.
- Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR. (1978). Dislocations after total hip-replacement arthro-plasties. J Bone Joint Surg Am. 60(2):217–220.
- Leslie IJ, Williams S, Isaac G, Ingham E, Fisher J. (2009). High cup angle and microseparation increase the wear of hip surface replacements. Clin Orthop Relat Res. 467(9):2259–2265.
- Mahmood SS, Mukka SS, Crnalic S, Wretenberg P, Sayed-Noor AS. (2016). Association between changes in global femoral offset after total hip arthroplasty and function, quality of life, and abductor muscle strength. Acta Orthop. 87(1):36–41.
- Tonnis D. (1976). Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 119:39–47.
- Kim YH, Choi Y, Kim JS. (2009). Influence of patient, design, and surgery-related factors on rate of dislocation after primary cementless total hip arthroplasty. J Arthroplasty. 24(8):1258–1263.
- Cassidy KA, Noticewala MS, Macaulay W, Lee JH, Geller JA. (2012). Effect of femoral offset on pain and func- tion after total hip arthroplasty. J Arthroplasty. 27(10):1863–1869.
- McGrory BJ, Morrey BF, Cahalan TD, An KN, Cabanela ME. (1995). Effect of femoral offset on range of motion and ab-ductor muscle strength after total hip arthroplasty. J Bone Joint Surg Br. 77(6):865–869.
- Romero AC, Imrie S, Goodman SB. (2001). Sliding trochanteric osteotomy preserves favorable abductor bio- mechanics in revision total hip arthroplasty. J Arthroplasty. 16(1):55–64.
- Callanan MC, Jarrett B, Bragdon CR, Zurakowski D, Rubash HE, Freiberg AA, et al. (2011). The John Charnley Award: risk factors for cup malpositioning: quality improvement through a joint registry at a tertiary hospital. Clin Orthop Relat Res 469(2):319–329.
- Kruse CR, Broeng L., Overgaard S. (2017). Radiographic cup position following posterior and lateral approach to total hip arthroplasty. An explorative randomized controlled trial. PLoS One. 13(1):e0191401.
- Wan Z, Malik A, Jaramaz B, Chao L, Dorr LD. (2009). Imaging and navigation measurement of acetabular component position in THA. Clin Orthop Relat Res. 467(1):32–42.
- Ranawat CS, Rao RR, Rodriguez JA, Bhende HS. (2001). Correction of limb-length inequality during total hip arthroplasty. J Arthroplasty. 16(6):715–720.
- Landis JR, Koch GG. (1977). The measurement of observer agreement for categorical data. Biometrics. 33(1):159–174.
- Patel AB, Wagle RR, Usrey MM, Thompson MT, Incavo SJ, Noble PC. (2010). Guidelines for implant place- ment to minimize impingement during activities of daily living after total hip arthroplasty. The Journal of arthroplasty. 25(8):1275–1281.
- Jolles BM, Bogoch ER. (2006). Posterior versus lateral surgical approach for total hip arthroplasty in adults with os-teoarthritis. Cochrane Database Syst Rev. (3):Cd003828.
- Arthursson AJ, Furnes O, Espehaug B, Havelin LI, Soreide JA. (2007). Prosthesis survival after total hip arthro- plasty—does surgical approach matter? Analysis of 19,304 Charnley and 6,002 Exeter primary total hip arthroplasties reported to the Norwegian Arthroplasty Register. Acta Orthop. 78(6):719–729.
- Hailer NP, Weiss RJ, Stark A, Karrholm J. (2012). The risk of revision due to dislocation after total hip arthro- plasty depends on surgical approach, femoral head size, sex, and primary diagnosis. An analysis of 78,098 operations in the Swedish Hip Arthroplasty Register. Acta Orthop. 83(5):442–448.
- Masonis JL, Bourne RB. (2002). Surgical approach, abductor function, and total hip arthroplasty dislocation. Clin Orthop Relat Res. 405:46–53.
- Jacobsen S, Sonne-Holm S, Lund B, Soballe K, Kiaer T, Rovsing H, et al. (2004). Pelvic orientation and assess- ment of hip dysplasia in adults. Acta Orthop Scand. 75(6):721–729.
- Rosenlund S, Broeng L, Jensen C, Holsgaard-Larsen A, Overgaard S. (2014). The effect of posterior and lateral approach on patient-reported outcome measures and physical function in patients with osteoarthritis, undergoing total hip replacement: a randomised controlled trial protocol. BMC Musculoskelet Disord. 15:354.
- Hoppenfeld S, DeBoer P, Buckley R. (2009). The Hip. Surgical Exposures in Orthopaedics The Anatomic Approach. Philadelphia: Lippincott Williams & Wilkins:403–462.
- Mulliken BD, Rorabeck CH, Bourne RB, Nayak N. (1998). A modified direct lateral approach in total hip arthro- plasty: a comprehensive review. J Arthroplasty. 13(7):737–747.