Previous Issues Volume 2, Issue 2 - 2017
Change Takes Time: EMS as the Spark Plug for Faster Acute Ischemic Stroke Care
Karen Greenberg*, Alexander Lesenskyj, Daniel Eichorn, Christina R. Maxwell, Michael D'Ambrosio, Erol Veznedaroglu, Mandy J. Binning
Drexel Neurosciences Institute, Drexel University College of Medicine, 219 North Broad St 7th Floor, Philadelphia, USA.
Corresponding Author: Karen Greenberg, Drexel Neurosciences Institute, Drexel University College of Medicine, 219 North Broad St 7th Floor, Philadelphia, USA Tel: (215) 762-6915; E-Mail: [email protected]
Received Date: 06 Jun 2017 Accepted Date: 23 Jun 2017 Published Date: 27 Jun 2017
Copyright © 2017 Greenberg K
Citation: Greenberg K, Lesenskyj A, Eichorn D, Maxwell CR, et al. (2017). Change Takes Time: EMS as the Spark Plug for Faster Acute Ischemic Stroke Care. Mathews J Emergency Med. 2(2): 025. ABSTRACT
Introduction :
It is well documented that a Prehospital Stroke Alert (PHSA) protocol leads to decreased treatment times for stroke patients. Outcomes measured typically include Door to Physician (DTP), Door to CT (DTCT), and Door to Needle (DNT) times. Our comprehensive stroke center's PHSA system has been in place since 2012. This study evaluates 3 specific endpoints. First, Emergency Medical Services (EMS) improve their recognition of stroke symptoms as they gain experience with PHSA. Second, a PHSA protocol decreases treatment times of DTP, DTCT, and DNT over a study period of 3 years compared to times recorded prior to implementation of the PHSA system. Third, when patients present to our Neurologic Emergency Department (Neuro ED) as a PHSA, rather than a non-PHSA, the treatment times are markedly decreased, and acute ischemic stroke care is significantly expedited.
Methods :
A retrospective chart review was conducted for patients who presented to our hospital with an admitting diagnosis of stroke from 2012, 2013 and the first half of 2014. Patients were screened for presentation to the Neuro ED and further stratified based on whether a PHSA was called. PHSA was called if EMS deemed the patient's Cincinnati Stroke Scale score as positive, and symptom onset was within 6 hours. We recorded DTP, DTCT, and DTN times over the years for all patients meeting these inclusion criteria.
Results :
Three hundred and five patients with an admission diagnosis of stroke were seen in the Neuro ED (Hours are 0700- 1800, 7 days a week) from 2012 through the first half of 2014, 128 of which presented as PHSAs. EMS responders accurately diagnosed stroke in 72% of cases. When EMS diagnosis was combined with Neuro ED physician expertise, accuracy improved to 85%. Previously, EMS assessment of stroke was accurate only 66% of the time. PHSA patients had decreased DTP, DTCT, and DTN times over the two and a half year period. When comparing the PHSA group to non-PHSA group, statistically significant differences were found in DTP and DTCT times within each year (p = 0.0001).
Discussion :
In conclusion, gaining experience with a PHSA protocol did in fact lead to EMS better recognizing stroke symptoms, reduction in the times of delivery of care for acute ischemic stroke patients over the years 2012-2014, and a markedly statistically significant difference in treatment times if patients were seen as a PHSA as opposed to a non-PHSA.
INTRODUCTION
In recent years, specialized emergency departments (EDs) have led to superior patient care. These specialized EDs, such as trauma, geriatrics, and pediatrics, cater to unique patient needs that are not met by the design of standard EDs [1-3]. Our small community hospital has specialized neurological services, including a Prehospital Stroke Alert (PHSA) protocol and a Neurological ED (Neuro ED). These innovative practices working in conjunction with each other have effectively decreased the time to treatment for stroke patients [4, 5].
The emergency medical services (EMS) responders have been integral in achieving rapid identification and treatment of acute stroke patients. Although the EMS responders are from different systems and have different levels of training such as Basic EMT or paramedic, all of the EMS responders are trained in Advanced Stroke Life Support (ASLS®). The curriculum designed by the University of Miami, Miller School of Medicine (Miami, FL) helps EMS personnel accurately pre-notify the hospital of incoming potential stroke patients. Upon completion of this training, EMS recognizes the importance of both early identification of symptoms, and delivery of patients to a facility that is equipped to capitalize on this advantage. Con tinuing to practice these skills allows EMS to improve upon accuracy and efficiency with ASLS and the PHSA.
Appropriate stroke evaluation in the field prior to arrival at our hospital is accomplished using the Cincinnati Prehospital Stroke Scale; if positive, a PHSA is called [6] The Cincinnati Prehospital Stroke Scale quickly assesses facial droop, arm drift, and abnormal speech. If any one of these 3 signs is abnormal, the probability of a stroke is 72% (Table 1) [7, 8].
Table 1: Cincinnati Prehospital Stroke Scale assessment guidelines. Table reproduced from The American Stroke Association document, "Target: Stroke," previously modified from Kothari and colleagues (1999).
| Cincinnati Prehospital Stroke Scale | Normal | Abnormal |
|---|---|---|
| Facial Droop - patient shows teeth or smile | Both sides of face move equally | One side of the face does not move as well as the other side |
| Arm Drift - patient closes eyes and extends both arms straight out, with palms up, for 10 sec. | Both arms move the same or both arms do not move at all (other findings, such as pronator drift, may be helpful) | One arm does not move or one arm drifts down compared with the other |
| Abnormal Speech "have the patients say "you can't teach an old dog new tricks" | Patient uses correct words with no slurring | Patient slurs words, uses the wrong words, or is unable to speak |
Quick in-field EMS notification is the spark plug in a cascade of events: a cascade that involves being evaluated by a trained physician and obtaining a plain head CT almost simultaneously, and receiving appropriate treatment (Schematic 1).
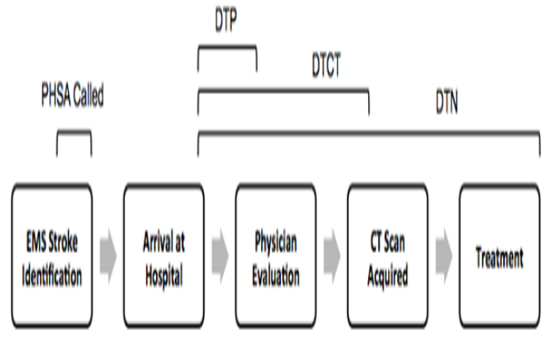
Schematic 1: Typical sequence of events for the PHSA protocol. The linear depiction above of DTP and DTCT can be interchangeable. This is because physician evaluation can occur immediately before, on the way to, or immediately after CT scanning. DTN was chosen as the treatment modality of interest due to availability of needle puncture times.
These steps illustrate the PHSA and Neuro ED's interdisciplinary function [5]. Further, this PHSA protocol allows for patients to meet the Neuro ED team at computed tomography (CT) imaging immediately upon arrival to the hospital. Since the opening of the Neuro ED and the initiation of the PHSA, the door-to-CT (DTCT) and door-to-needle (DTN) times have decreased by 67% and 23%, respectively [5]
Persistent decreases in DTP, DTCT, and DTN times, facilitated by EMS, allow for rapid administration of tissue plasminogen activator (tPA). This is critical because overwhelming evidence suggests rapid tPA administration following ischemic stroke onset improves patient outcomes [9]. More specifically, quicker time to treatment is linked to decreases in hospital mortality rate, reduced symptomatic intracranial hemorrhage, increased chance of independent ambulation at discharge, and shortened hospital length of stay [10]. The chance of achieving an excellent clinical outcome 90 days post-stroke, measured by a modified Rankin score (MRS) of 0 or 1, increased by 37% when patients were treated within 90 minutes of moderate stroke onset. Simply stated, early treatment of ischemic stroke leads to a decrease in likelihood of post-stroke disability [11].
Our study highlights the crucial role EMS responders play for patients arriving at the hospital with a suspected stroke diagnosis. Through the lens of the PHSA, we will examine DTCT times, door-to-physician (DTP) times, and DTN times over the years. By looking at door-to-treatment times from the years 2012-2014, we aim to show how quality of care improves when EMS responders and practitioners gain experience with the PHSA system.
METHODS
A retrospective chart review was approved by the local institutional review board. From 2012 to the first half of 2014, 1025 patients presented directly to our hospital either by EMS or as a walk-in through the Emergency Department, with the diagnosis of stroke. 305 of the patients seen with the admitting diagnosis of stroke were evaluated specifically in the Neuro ED. The Neuro ED runs from 0700-1800 hours, seven days a week. Hours were chosen based on previous data that has demonstrated the time of day when strokes most frequently occurred was between 8 AM and noon [12]. These patients were then stratified based on whether a PHSA was called. PHSA was called by EMS if the patient has a positive Cincinnati score and onset of symptoms was less than 6 hours (Schematic 2).
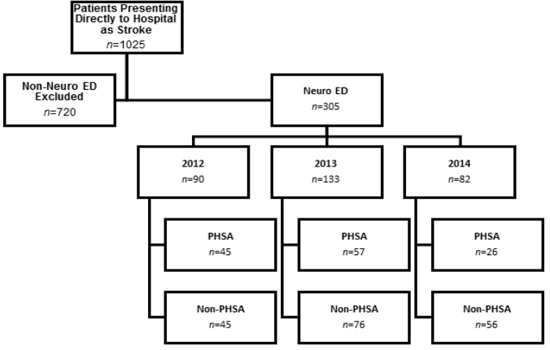
Schematic 2: Screening process used to obtain final experimental and control group populations from 2012 to 2014. All patients who did not present during the Neuro ED hours (See Methods) were excluded. Patients who presented to the Neuro ED (n = 305) were split into experimental (PHSA, n = 128) and control (non-PHSA, n = 177) groups. PHSA group includes patients with positive Cincinnati score and onset of symptoms < 6 hours.
Three different endpoints were calculated. The first endpoint looked at EMS accuracy of diagnosis for stroke symptoms. The second endpoint looked at whether treatment times improved over each year from 2012-2014 with the PHSA in place. Treatment outcomes measured including DTCT, DTP, and DTN times for administration of tPA. The third endpoint looked at treatment time differences between patients who were PHSAs vs those patients that arrived to the ED with no prenotification made to the Neuro ED.
STATISTICS
IBM SPSS Version 22 was used to perform all statistics. Statistical analyses included using descriptive statistics, independent samples t-tests, correlations and Chi-Square analyses when appropriate.
RESULTS
One hundred and fifty of all the reviewed stroke patients were female and 155 were male that were seen in the Neuro ED (n=305). Ages ranged from 16 to 98 years with a mean of 66.4 years (SD ±15.3).
Of the 128 patients that were seen as PHSA called by EMS in the field, the Neuro ED physicians agreed with the diagnosis of stroke for 93 patients which is 72% of cases. Of these 93 patients with an admitting diagnosis of stroke, the discharge diagnosis of stroke was concordant in 79 patients. When matched with discharge diagnoses, EMS collaborating with the Neuro ED physicians, improved accuracy and identified stroke patients 85% of the time (79/93 cases). Discharge diagnoses are displayed in Figure 1. The most common discharge diagnoses other than stroke were diabetic symptoms (4%) and TIA (2%).
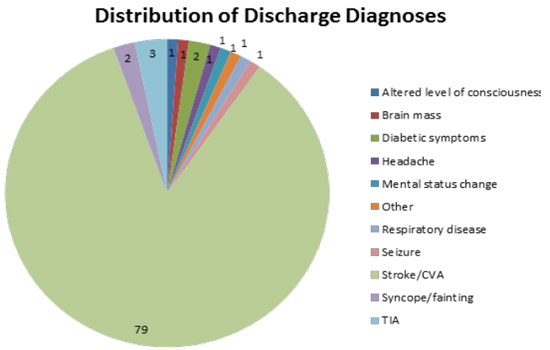
Figure 1 : Distribution of discharge diagnoses among PHSA patients with stroke as admission diagnosis. (n-93).
Trends in "door-to-treatment" times were noted from 2012 to 2014 (Figure 2). When looking within the PHSA group specifically and comparing DTP times across years, statistically significant differences were noted (p = 0.0001). No statistically significant differences for PHSA patients were found in the DTCT or DTN groups across the years 2012 to 2014; however, a general decreasing trend was noted from the start of study in 2012 to the conclusion in 2014.
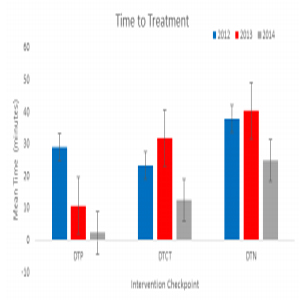
Figure 2 : Trend in mean time-to-treatment from 2012-2014 in PHSA patients. DTN, DTCT, and DTP represent the same "door-to-treatment" groups as described in Introduction and Methods. (Door-to-treatment; n2012, n2013, n2014). (DTP; 45, 57, 26), (DTCT; 45, 57, 26). (DTN; 6, 9, 10). 2012 is displayed in blue, 2013 in red, and 2014 in gray.
128 out of 305 patients presented as PHSAs. A control group of non-PHSAs was made up of 177 patients. These patients either arrived by ambulance but no PHSA was called by EMS, or these patients arrived as walk-ins. All 305 patients were evaluated in the Neuro ED. Mean door-to-treatment times for both groups are shown in (Figure 3). When comparing the PHSA group to non-PHSA group, statistically significant differences were found in DTP and DTCT times within each year (p = 0.0001).

Figure 3: Door to treatment times for three checkpoints in the management of stroke patients. In the DTN group there were 26 PHSAs and 13 non-PHSAs. In the DTCT group there were 128 PHSAs and 166 nonPHSAs. In the DTP group there were 128 PHSAs and 177 non-PHSAs.
DISCUSSION
Accurate diagnoses are critical in emergent settings. When EMS evaluates a patient with acute neurologic symptoms utilizing a prehospital stroke assessment, such as the Cincinnati Stoke Scale, they can significantly aid in the clinical decision making process. Our study demonstrates that EMS correctly identified prehospital stroke patients in 72% of the alerts called. This percentage is exactly in line with the expected prediction of utilizing the Cincinnati Stroke Scale and supports its continued use in the prehospital setting [7, 8].
Our study also found that EMS responders working collaboratively with the Neuro ED physicians, improved accuracy of diagnosing stroke to 85% of patients presenting as a PHSA they alerted from the field. Previously, EMS assessment of stroke was accurate only 66% of the time [5]. This high percentage can be, in part, attributed to ASLS training and the use of the Cincinnati Prehospital Stroke Scale; but most importantly, by both groups of EMS and the Neuro ED gaining experience with the PHSA protocol together. The enhanced accuracy of EMS stroke diagnosis supports their use as an initial step of PHSAs and is a promising tactic for achieving improved post-stroke outcomes.
Our ability to rely on EMS personnel hinges on their activation of the PHSA protocol. Current literature suggests that EMS is underutilized for certain patient populations, such as acute myocardial infarction and stroke. Tataris and colleagues found that between 2003 and 2009 EMS usage did not increase throughout the six-year period for either of these emergencies [13]. This trend prompted our specific inquiry regarding EMS's role in stroke treatment and care, as data indicates the importance of early stroke identification.
A few earlier studies also recognize the importance of early stroke treatment in the effort to improve outcomes. These studies demonstrate that PHSAs in general help stroke patients to be evaluated quicker [4, 5, 14]. Cumbler and colleagues (2012) showed that establishing an alert protocol for incoming strokes decreased time from stroke alert to CT from 69.0 to 29.5 minutes [15]. Another similar study describes a system in which a neurointerventional (NI) fellow was notified of the stroke patient and clinical criteria prior to imaging, at which time the fellow activated the rest of the NI suite team members of the case. This system decreased the time from imaging to the NI suite by 35 minutes, subsequently decreasing time to treatment [16]. These novel systems have been identified as potential solutions for improving the clinical outcomes of stroke patients
Despite important differences between our PHSA protocol and the above systems, we have found similar improvements in time-to-treatment as the Neuro ED team gained experience with the PHSA protocol themselves. Our results indicate mean times in the PHSA group of 33.7 ± 3.68 SEM, 24.9 ± 4.15 SEM and 15.5 ± 2.06 SEM for DTN, DTCT, and DTP. The DTN times specifically are lower than our historical means of 44 minutes [5]. More importantly, the Target: Stroke campaign has implemented even more aggressive recommendations that acute ischemic stroke patients have a DTN of less than 60 minutes in at least 75% of patients, and a DTN of less than 45 minutes in at least 50% of patients [8]. For hospitals across the country and the world that are struggling to treat acute ischemic patients in a timely manner, a PHSA protocol such as ours can be an easy implementation to help achieve the Target: Stroke guidelines.
Not only has this protocol yielded immediate reduction in door-to-treatment times, but these improvements have withstood an initial test of time while managing to consistently diminish over the two and a half year period measured in this study. The difference for DTP times from 2012-2014 was statistically significant (p = 0.001). DTCT and DTN remained statistically similar across the years (p = 0.35), but both average times were decreased from the start of the study in 2012 to the endpoint in 2014. DTCT times had a slight increase in 2012 from 2013, but then a marked decrease from 2013 to 2014. We attribute the slight spike in 2013 to variability in PHSA patients being seen by a physician first versus going straight to CT scan. Also, in a small amount of cases, PHSA patients first needed stabilization in the Neuro ED prior to being transported to imaging.
The most striking outcome of our study is the large difference in door-to-treatment times when patients present as a prehos- pital stroke alert vs a non-prehospital stroke alert. Our paper is unique in this aspect to look at the stark differences of treatment times based on how patients arrive to the ED: with EMS as prenotification of possible stroke, with EMS and no notification of possible stroke, or walk-ins with stroke symptoms.
Recent literature has focused on both EMS and ED physician miss rates of stroke patients and how this leads to delay in care. For instance, EMS-suspected strokes made it to the CT scan on average at 34 minutes, while EMS-missed strokes took an average of 84 minutes. Consequently, 14.9% of EMSsuspected stroke patients received fibrinolytics, compared to only 4.4% of EMS-missed stroke patients [17].
Arch, et al. looked at the missed stroke rates of patients presenting either to a comprehensive stroke center or a community based primary stroke center. 103 strokes were initially misdiagnosed, which is 22% of the included strokes at the combined centers. 33% of missed cases of ischemic stroke presented within a three-hour time window for tPA eligibility. An additional 11% presented between 3 and 6 hours of symptom onset for consideration of endovascular therapy [18].
It is well known that failure to recognize an ischemic stroke in the emergency department (ED) is a missed opportunity for acute interventions and for prompt treatment with secondary prevention therapy [18]. Now that our paper emphasizes how patients physically present to the ED correlates directly with their efficiency of stroke care, public awareness by EMS and hospitals alike needs to become paramount.
Future studies to help determine how resources should be allocated for treating stroke patients may help determine which hospitals can and should have a PHSA in place. Despite these limitations, we can conclude that EMS prenotification contributes to the efficacy of the PHSA. Striving to improve door-totreatment times is a strategy to enhance acute stroke care; and the role of EMS is one component to critically weigh when attempting to create a lasting change over time.
CONCLUSION
A retrospective review of stroke patients presenting to the Neuro ED shows that EMS prenotification has a beneficial effect on the PHSA practice, door-to-treatment times, and in turn the delivery of care. Our trends across the years reveal a reduction in the time to delivery of care for patients arriving at the hospital as PHSAs. Given the notable differences between time to care for PHSA patients and non-PHSA patients, we demonstrate the role EMS plays in our PHSA protocol is not only crucial to identifying stroke patients, but also significantly aids ED providers to deliver timely care and treatment. Additional prospective studies are necessary to specifically identify the crux of the PHSAs success, with the ultimate goal of improving post-stroke outcomes.
REFERENCES
- Hwang U and Morrison RS. (2007). The geriatric emergency department. J Am Geriatr Soc. 55: 1873-1876.
- Cowley RA and Scanlan E. (1979). University trauma center: Operation, design and staffing. Am Surg. 45: 79-85.
- Wang HE and Yealy DM. (2012). Distribution of specialized care centers in the united states. Ann Emerg Med. 60: 632-637
- Greenberg K, Maxwell CR, Moore KD, D'Ambrosio M, et al. (2015). Improved door-to-needle times and neurologic outcomes when iv tissue plasminogen activator is administered by emergency physicians with advanced neuroscience training. Am J Emerg Med. 33: 234-237.
- Binning MJ, Sanfillippo G, Rosen W, D'Ambrosio M, et al. (2014). The neurological emergency room and prehospital stroke alert: The whole is greater than the sum of its parts. Neurosurgery. 74: 285
- Hurwitz AS, Brice JH, Overby BA and Evenson KR. (2005). Directed use of the cincinnati prehospital stroke scale by laypersons. Prehosp Emerg Care. 9: 292-296.
- Kothari RU, Pancioli A, Liu T, Brott T, et al. (1999). Cincinnati prehospital stroke scale: Reproducibility and validity. Ann Emerg Med. 33: 373-378.
- The American Stroke Association. Target: Stroke.
- Chapman SN, Mehndiratta P, Johansen MC, McMurry TL, et al. (2014). Current perspectives on the use of intravenous recombinant tissue plasminogen activator (tpa) for treatment of acute ischemic stroke. Vasc Health Risk Manag.10: 75-87.
- Saver JL, Fonarow GC, Smith EE, Reeves MJ, et al. (2013). Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 309: 2480-2488.
- Mitka M. (2013). Early treatment of ischemic stroke with intravenous tpa reduces disability risk. JAMA. 310: 1111.
- Kelly-Hayes M, Wolf PA, Kase CS, Brand FN, et al. (1995). Temporal patterns of stroke onset. The Framingham Study. Stroke. 26(8): 1343-1347.
- Tataris K, Kivlehan S and Govindarajan P. (2014). National trends in the utilization of emergency medical services for acute myocardial infarction and stroke. West J Emerg Med. 15: 744-748.
- Desai JA and Smith EE. (2013). Prenotification and other factors involved in rapid tpa administration. Curr Atheroscler Rep.15: 337
- [Window Title] Adobe CS6 Service Manager[Main Instruction] Adobe CS6 Service Manager has stopped working[Content]Windows is checking for a solution to the problem... [Cancel]
- Mehta BP, Leslie-Mazwi TM, Chandra RV, Bell DL, et al. (2014). Reducing door-to-puncture times for intra-arterial stroke therapy: A pilot quality improvement project. J Am Heart Assoc. 3: e000963
- Oostema JA, Konen J and Chassee T. (2015). Clinical predictors of accurate prehospital stroke recognition. Stroke.46(6): 1513-1517.
- Arch AE, Weisman DC and Coca S. (2016). Missed ischemic strokek diagnosis in the Emergency Department by Emergency Medicine and Neurology Services. Stroke. 47: 668-673.