Information Links
Related Conferences
Previous Issues Volume 7, Issue 2 - 2023
Broken File Retrieval in the Lower Left Second Molar Using the Ultrasonic Technique
Wided Glii, Amira Kikly, Fouad Brigui, Ameni Chadlia Belguith, Neila Zokkar, Nabiha Douki
Dental Medicine Department of Sahloul Sousse Hospital, Faculty of Dentistry of Monastir, Tunisia
*Corresponding Author: Wided Glii, Dental Medicine Department of Sahloul Sousse Hospital, Faculty of Dentistry of Monastir, Tunisia, Tel: (+216) 93546683, E-mail: [email protected].
Received Date: August 04, 2023
Published Date: August 22, 2023
Citation: Glii W, et al. (2023). Broken File Retrieval in the Lower Left Second Molar Using the Ultrasonic Technique. Mathews J Dentistry. 7(2):36.
Copyrights: Glii W, et al. © (2022).
ABSTRACT
Endodontic file fracture is a common problem in root canal treatment. This may be due to overuse of instruments or incorrect technique in root canals with difficult anatomy. However, a broken endodontic file does not always mean that treatment has failed. Frequently the broken fragment can be removed, and the root canal treatment completed. Separation of a file usually occurs in molars, mainly in the mesiolingual canal due to major curvature, poor access or small diameter. Aim: This article reports the management of an intracanal separated NiTi instruments under operating microscope using ultrasonic technique. Observation: A patient in good general condition was referred by a colleague following an instrument fracture (SX file) in the left mandibular 2nd molar (37). Radiographic examination revealed the presence of a 4mm instrument blocking the middle third of the M°L root. To clean and disinfect the part of the canal beyond the instrument fracture, we decided to remove the instrument from the canal using an ultrasonic technique under an operating microscope. Discussion: Advances in technology have provided a number of tools for the extraction of files, including ultrasonic devices, with the aid of a microscope to facilitate visibility and minimise extraction of dentin from the root canal. Therefore, this report discusses the management of a broken file in a mandibular molar using an ultrasound device with the aid of a microscope. Conclusion: The ultrasonic technique is effective for the removal of broken instruments. Direct, visible access to the fragment under the dental microscope is essential for successful fragment recovery.
INTRODUCTION
Endodontics is by definition the discipline of dentistry concerned with the prevention, diagnosis and treatment of pulp diseases and associated periradicular infections. The aim of endodontic treatment is to treat pulp and periapical diseases, transforming a pathological tooth into a healthy, asymptomatic and functional entity.
Root canal treatment is a complex process that involves cleaning, shaping and filling the tooth's root canals. If an instrument is broken in the canal, it can impede the cleaning and shaping process, leading to treatment failure. Broken files are more common on molars, particularly in the lower jaw, as the root canals of these teeth are smaller and more curved. The manual and mechanical instruments used for root canal treatment are mainly made of stainless steel or nickel-titanium, materials that can break if not used correctly. The incidence of broken files is 0.25% for manual instruments and 1.68% to 2.4% for rotary instruments. If an instrument fragment prevents the necessary instrumentation and decontamination of the root canal, an extraction attempt should be considered. The endodontic operating microscope allows direct and improved visualisation of separated instruments in the root canal, and the use of fine ultrasonic tips allows the fragment to be loosened and removed. The likelihood of removing a fractured instrument is directly related to visibility. The ability to access it in a straight line. When the fragment is located within the curvature of the root canal, visibility requires the root canal to be straightened.
This article reports the management of an intracanal separated NiTi instruments under operating microscope using ultrasonic technique.
OBSERVATION
Case report
29-year-old patient in good general condition referred by a colleague to the dental medicine department of Sahloul hospital following an instrumental fracture (SX file) at the level of the 2nd left mandibular molar (37).
The radiograph (Figure 1) shows a 4 mm instrument blocked in the middle third of the M°L root.

Figure 1. Pre-operative radiograph.
The instrument fracture prevented successful endodontic treatment of this tooth. In order to instrument and decontaminate the part of the canal beyond the fracture, we decided to remove the instrument from the canal. Briefly, rubber dam isolation and access cavity allowing for straight line access were performed (Figure 2).
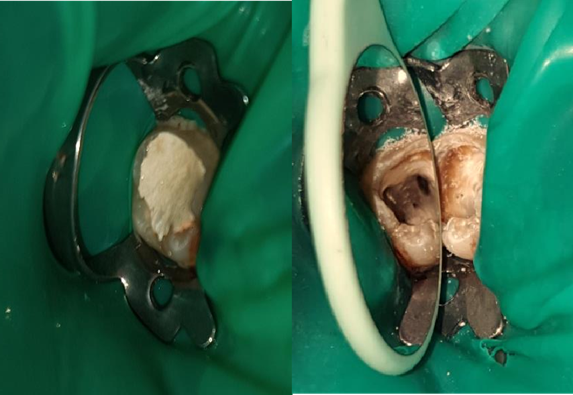
Figure 2. Rubber dam isolation and access cavity.
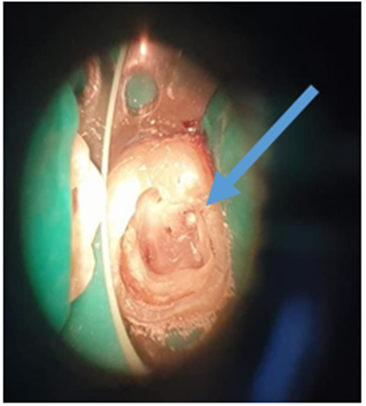
Figure 3. Microscopic view: locating the instrument at CM°L level.
Largo drill/an ultrasonic diamond insert (ET18D) are used to widen the coronal funnel-shaped channel at the instrument fragment to allow access to the fractured instrument (Figure 4).
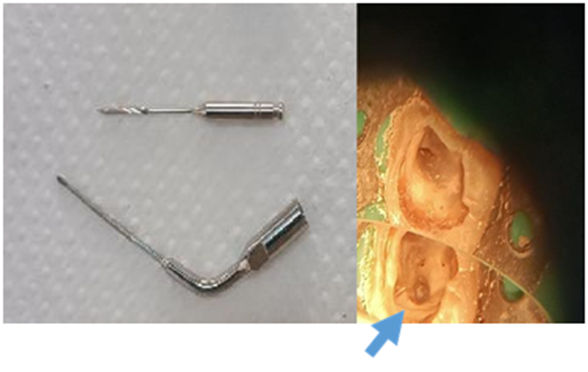
Figure 4. Enlargement of the coronal part above the instrument.
Figure 5. Lateral passage to the fragment of the instrument with a 10" file.
A fine ultrasonic insert (ET20/ ET25) was then used to clear the head of the instrument. Then, using the tip of the insert, the instrument was vibrated in an anti-clockwise direction → the file was removed (Figure 6).

Figure 6. ET20; ET25 / removed broken file.
A retro-alveolar radiograph is then taken to ensure that the fractured instrument has been completely removed and that the canal is permeable (Figure 7). Once the canal has been re-permeabilised, the canal is reshaped and disinfected. A postoperative radiograph was taken, showing complete clearance and obturation of the canal (Figure 8).
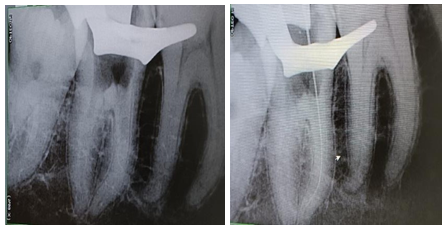
Figure 7. Per-operative X-ray.

Figure 8. Postoperative X-ray.
DISCUSSION
During root canal therapy instrument fracture is a troublesome incident that can interfere with efficient cleaning and shaping of the root canal or act as an irritant to the periapical tissues. There are several treatment options for separated intracanal instrumentation. Conservative options include bypassing the fragment, removing the fragment or preserving the fragment with instrumentation and a coronal filling to the fragment. The surgical option consists in surgically removing the separated instrument [1]. The optimal treatment method is retrieval of the instrument as in cleaning the root canal and eliminating microorganisms can then be accomplished adequately [2].
The factors determining the potential to remove a separated instrument should be considered during the diagnostic workup [3].
Studies have shown that the successful retrieval depends on:
- The position of the fragment in the root, apical or coronal, before or after the curvature, a direct visual access: Depending on its position, it may be more or less easy to remove. For the middle and coronal thirds, the success rate is very good, whereas for the apical third, removal is more difficult. The most decisive factor will be the position of the instrument in relation to the root canal curvature, and the degree and radius of this curvature. If the coronal part of the fragment is apical to the curvature and it is impossible to establish direct visual access, the chances of removal are slim [4].
- Type of instrument fractured: the chances of removing a steel instrument are better than for fragments of NiTi files. The latter tend to fracture secondarily when ultrasound is used. This is because the build-up of heat at the point of contact with the insert adds stress to the already weakened fragment. Conversely, steel is capable of distributing energy, making ultrasound more effective [5].
- Fragment length and width: The width of the coronal part of the fragment is also important to consider. The wider the coronal portion, the greater the amount of root dentine that needs to be removed to free it. This increases the risk of perforation or root embrittlement. A counter-indication to the removal attempt may then be considered. Length must also be assessed. A long fragment may lie on either side of the curvature. The fragment can be removed if direct visual access is established [4].
- Root anatomy, depressions, curvature, width.
The operator must be trained and must have access to an adequate technical platform.
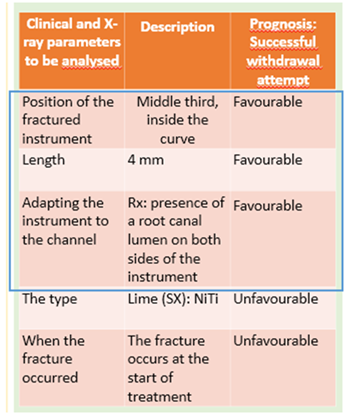
In our case, attempts to bypass the instrument having failed, recovery of the fragment was attempted successfully after an analysis of the clinical and radiological parameters detailed in the following table,
Variety of techniques and systems have been developed Endodontic instrument retrieval systems, such as the Masserann kit or IRS, can damage root canal dentin. Ultrasound, on the other hand, is the most effective and reliable tool for removing a separated endodontic instrument from a root canal. Nevares et al. found that separated instruments were twice as likely to be successfully removed when visible under the microscope than when not. Yet, removal of fractured fragment from the root canal requires manual skills, equipment, instruments and good knowledge of root canal anatomy [6].
The use of an operating microscope and small-diameter ultrasonic tips in endodontic treatment can improve minimally invasive root canal preparation and increase the safety of instrument extraction. In general, the success rate in instrument retrieval is high for separated instruments located before the canal curvature, moderate for those located in the curvature, and reduced for those located beyond the curvatureIn addition, studies have shown that the success rate of removing separated instruments is higher when the curvature of the canal is lower and the radius is longer. Canal curvature was measured by drawing a straight line from the orifice to the fractured end of the separated instrument, then drawing a line parallel to its long axis. The angle between the two lines was used to calculate canal curvature [7]. The use of an ultrasonic instrument assisted by a microscope is a gentler method of treating broken files than other methods [8,9,10]. It can erode dentin structure more conservatively and is less likely to damage root structure and periodontal tissues [8].
Broken files can be removed under either dry or wet conditions. Dry conditions offer better visibility under the microscope, which can help avoid procedural errors. However, heat generated from ultrasonic vibrations is unavoidable, and the temperature has the possibility to increase to more than 10° C on the external root surface causing damage to the periodontal tissue Files can generate secondary heat when in contact with the ultrasonic tip. This can damage tooth tissue. Therefore, EDTA irrigation was performed when the ultrasonic tip was activated at the lowest power setting.
This improved the cleanliness of the root canal wall and reduced the risk of tissue damage. The tips used were ET20 and ET25. They were made of titanium-niobium alloy and diamond-coated, making them abrasive. The ET20 was moved counter-clockwise into the coronal 1/3 of the root canal, while the ET25 was moved into the central 1/3 of the root canal. This gave the file an unscrewing effect, helping to remove the broken instrument from the root canal. [8].
CONCLUSION
Instrument fracture as a procedural accident can be treated in a number of non-surgical ways: removal of the fragment using ultrasonic instruments or recovery kits, contouring using small manual files, cleaning and filling of root canals down to the coronal level of the broken instrument [10]. The optimal treatment method consists of recovering the instrument. However, the chances of success must be assessed before any attempt is made to remove a fractured instrument.
ACKNOWLEDGMENTS
None.
CONFLICTS OF INTERESTS
The authors have no conflicts of interest to declare.
REFERENCES
- Fouad B, Kikly A, Belghith AC, Glii W, Hodroj LF, et al. (2023). Broken file: bypass or ultrasonic removal technique. J Dent Maxillofacial Res. 6(2):33-36.
- Dako T, Bica CI, Lazar L, Lazar AP, Monea M. (2020). Separated Instrument Management as a Procedural Accident in Endodontics Using the EDTA (C10H16N2O8) Aided Bypassing Technique and the Ultrasonic Removal Method. An in vitro Study. Revista de Chimie. 71(11):73-79.
- Heydari A, Rahmani M, Heydari M. (2016). Removal of a Broken Instrument from a Tooth with Apical Periodontitis Using a Novel Approach. Iran Endod J. 11(3):237-240.
- Gencoglu N, Helvacioglu D. (2009). Comparison of the different techniques to remove fractured endodontic instruments from root canal systems. Eur J Dent. 3(2):90-95.
- Andrabi SM, Kumar A, Iftekhar H, Alam S. (2013). Retrieval of a separated nickel-titanium instrument using a modified 18-guage needle and cyanoacrylate glue: a case report. Restor Dent Endod. 38(2):93-97.
- Rai A, Ayer A, Vikram M. (2022). Management of Separated Endodontic Instrument and a Blocked Canal-A Case Report. Journal of Nepalese Association of Pediatric Dentistry. 3(1):40-43.
- Terauchi Y, Sexton C, Bakland LK, Bogen G. (2021). Factors Affecting the Removal Time of Separated Instruments. J Endod. 47(8):1245-1252.
- Meidyawati R, Suprastiwi E, Setiati HD. (2019). Broken File Retrieval in the Lower Right First Molar Using an Ultrasonic Instrument and Endodontic Micro Forceps. Case Rep Dent. 2019:7940126.
- Fu M, Zhang Z, Hou B. (2011). Removal of broken files from root canals by using ultrasonic techniques combined with dental microscope: a retrospective analysis of treatment outcome. J Endod. 37(5):619-622.
- Shiyakov KK, Vasileva RI. (2014). Success for removing or bypassing instruments fractured beyond the root canal curve–45 clinical cases. Journal of IMAB–Annual Proceeding Scientific Papers. 20(3):567-571.