Previous Issues Volume 2, Issue 1 - 2017
Bleeding Disorder Education in Obstetrics & Gynecology Residency Training: A Follow up National Survey
Jennifer E. Dietrich1 , Elizabeth Baumler2 , Corey J. Sigue4 , Angelo P. Giardino4 *
1Division of Pediatric and Adolescent Gynecology, Department of Obstetrics and Gynecology, Baylor College of Medicine and Texas Children's Hospital, USA. 2Center for Health Promotion and Prevention and Research, School of Public Health, The University of Texas Health Science Center at Houston, USA. 3Texas Children's Health Plan, USA. 4Department of Pediatrics, Section of Academic General Pediatrics, Baylor College of Medicine, Senior Vice President/Chief Quality Officer, Texas Children's Hospital, USA. Corresponding Author: Angelo P. Giardino, Department of Pediatrics, Section of Academic General Pediatrics, Baylor College of Medicine Senior Vice President/Chief Quality Officer, Texas Children's Hospital, USA, Tel: (832) 824-1128; Email: [email protected]
Received Date: 10 Mar 2017 Accepted Date: 15 Mar 2017 Published Date: 17 Mar 2017
Copyright © 2017 Giardino AP
Citation: Dietrich JE, Baumler E, Sigue CJ and Giardino AP. (2017). Bleeding Disorder Education in Obstetrics & Gynecology Residency Training: A Follow up National Survey. Mathews J Gynecol Obstet. 1(1): 008.
ABSTRACT
Background Heavy menstrual bleeding in the most common bleeding manifestation seen by OB/GYNs with subsequent bleeding disorders discovered in 11% of women of all ages. Methods A 25-item questionnaire survey was mailed to all OB/GYN residents in US ACGME approved programs in 2012 which evaluated demo¬graphic information, practice, and heavy menstrual bleeding risk situations. Results were compared to a similar 2010 survey. Descriptive statistics and independent sample t-tests were performed. Results The 2012 survey response rate was 28% (n=68/241). The majority of chief residents (77.9%) reported viewing their training in the medical evaluation of heavy menstrual bleeding as sufficient preparation for future practice and reported an average of 15 hours devoted to education during each year of residency. Residents showed: improvement in the types of history questions they asked; no change in the evaluation for bleeding disorders (BDs) from 2010 to 2012; and continued (80.9%) identification of heavy menstrual bleeding at menarche as the most likely reason for BD evaluation. Conclusions The results highlight that continued opportunities exist to improve the education of OB/GYN residents in this area.
KEYWORDS
Bleeding Disorders; Heavy Menstrual Bleeding; Evaluation and Management of Bleeding Disorders.
INTRODUCTION
The evaluation of potential bleeding disorders continues to be an important residency training topic and an important area of clinical practice affecting approximately 1.3 percent of the US population [1, 2]. Heavy menstrual bleeding continues to be the most common bleeding manifestation seen by obstetrician-gynecologists (OB/GYNs) and the Center for Disease Control (CDC) reports that bleeding disorders (BD) are diagnosed in nearly 11% of women with heavy menstrual bleeding [3]. Among women presenting with heavy menstrual bleeding, approximately 11%–13 % have Von Willebrand Disease (VWD). [3] In addition, women with BD might be at an increased risk for other gynecological complications, such as ovarian cysts, endometriosis, fibroids, and miscarriage [4]. The National Heart, Lung, and Blood Institute of the National Institutes of Health (NHLBI) issued guidelines in 2007 concerning the diagnosis, evaluation, and management of VWD. The guidelines make recommendations for the questioning of patient history, physical exami¬nations, and laboratory testing, which is necessary to make the correct diag¬nosis of a BD such as VWD [5]. The publication of these guidelines provided an ideal platform to create an evaluation tool to assess the current content of BD assessment in OB-GYN residency training [6, 7]. [7-12] Two sections currently address the evaluation of menstrual disorders: Unit 4-Gynecology and Unit 5-Reproductive Endocrinology and Infertility. Within Unit 4 is a section focusing on the evaluation and management of abnormal uterine bleeding or dysfunctional uterine bleeding, which states that a resi¬dent should be able to elicit pertinent history to evaluate for causes of abnormal uterine bleeding and to appropriately interpret a complete blood count as well as coagulation tests [7]. In Unit 5, under the subsection Pediatric and Adolescent Gynecology, the evaluation of menstrual and endocrine disorders refers back to Unit 4. Currently, there is no specific language included regarding the consistent evaluation for bleeding disorders in women and adolescents [7]. In 2010, a national survey of OB-GYN residency programs evaluated the state of training around menorrhagia and bleeding disorders and found what was described as a mixed approach (combing both didactic and bedside teaching) regarding training around dysfunctional uterine bleeding. The results of this survey study also suggested that improvements in this content area would enhance training and to further align with the NHLBI guidelines [5]. The purpose of this follow-up study was to monitor the progress being made in the educational approach to BD evaluation in OB/GYN residency training programs in the two year period of time between the first survey and the current one reported herein. Using a nearly identical survey, information was collected from chief residents in OB/GYN residency programs regarding training experiences and fund of knowledge on BD was assessed.
METHODS
The survey study was reviewed and approved by the Institutional Review Board at the Baylor College of Medicine for both the 2010 survey and the 2012 survey. A 25-item questionnaire similar to the survey used in the 2010 survey was designed with three sections: demo¬graphic information, practice patterns, and risk situations. Demographic questions included information about the size of the residency training program and patient base. Topics such as the evaluation of menorrhagia and knowledge of BD were also assessed. Practice habits regarding history-taking and laboratory testing related to BD evaluation were assessed on a 6-point Likert scale. Questionnaires were sent to the chief residents of all nonmilitary Obstetrics and Gynecology residency programs in the continental United States listed in the American Medical Association's Graduate Medical Education Directory 2012. Findings of the 2012 questionnaire were then compared to the 2010 survey responses. Differences among the residents within a given program were not assessed due to small numbers. Nonresponding programs were sent subsequent questionnaires at one-month intervals, with a maximum of 3 mailings. Chief residents not responding to three mailed questionnaires received two telephone calls to request participation. Residents consented to participation by voluntarily completing the questionnaire and then mailing the survey back to the research team via the stamped selfaddressed return mail envelope. The study sample included 241 Chief-Residents from 241 non-military Obstetrics and Gynecology residency programs. In the context of a heavy menstrual bleeding work-up, chief residents were asked questions about the tests that might be routinely sent on such a patient, including coagulation studies, complete blood counts, iron studies, platelet evaluation, von Willebrand studies and thyroid studies. Respondents were asked which specific BDs were included in their training on the evaluation of heavy menstrual bleeding. Finally, clinical situations that indicated an increased risk for an underlying BD were assessed, as were situ¬ations that might improve or worsen a BD, such as use of hormones (improves) or use of aspirin (worsens). The database was analyzed using SPSS version 21. Descriptive statistics and independent sample t-tests for binomial proportions were performed.
RESULTS
After 3 rounds of mailing, the response rate for the 2012 survey was 28% (n=68/241) and the 2010 survey response rate was 30% (n=71/241). Descriptive statistics (means and frequency) were calculated for each questionnaire item within the 3 sections (demo-graphic information, practice patterns, and risk situations). The 2012 data was compared to the 2010 survey. Procedures included independent sample t-test for binomial proportions. No survey responses were excluded in this survey, as all participants filled out >50% of the questions included. Demographic information on chief residents revealed few differences. In the 2012 survey, the 91.2% responding chief residents were male, as opposed to the in 2010 where 76.9% of the responding chief residents were female. There were no significant differences in the number of respondents in 2010 versus 2012 and trainees at similar levels participated in each survey by year (Table 1). The patient population served by the 2012 responding programs was identified as predominately urban at 75%, similar to the 2010 survey (74%).
Table 1:: Sample descriptive
| 2012 n = 68 | 2010 n = 65 | |||
| Outcome | n | % | n | % |
| Gender (%) | ||||
| Male | 62 | 91.2 | 14 | 21.5 |
| Female | 6 | 8.8 | 50 | 76.9 |
| Size of Residency Program (Mean) | ||||
| Overall | 68 | 25.3 | 65 | 20 |
| Post Grad Year 1 | 68 | 6.5 | 65 | 4.7 |
| Post Grad Year 2 | 68 | 6.3 | 65 | 4.9 |
| Post Grad Year 3 | 68 | 6.2 | 65 | 4.9 |
| Post Grad Year 4 | 68 | 6.2 | 65 | 5 |
| Patient Setting (%) | ||||
| Urban | 51 | 75 | 48 | 73.8 |
| Suburban | 14 | 20.6 | 10 | 15.4 |
| Rural | 2 | 2.9 | 5 | 7.7 |
| Not Sure | 1 | 1.5 | 2 | 3.1 |
| Insurance: Public (%)* | ||||
| less than 10% | 1 | 1.5 | ||
| 10 - 25% | 7 | 10.4 | ||
| 26-50% | 29 | 43.3 | ||
| 51 - 75% | 21 | 31.3 | ||
| Over 75% | 9 | 13.4 | ||
| Insurance: Private (%)* | ||||
| less than 10% | 6 | 8.8 | ||
| 10 - 25% | 26 | 38.2 | ||
| 26-50% | 30 | 44.1 | ||
| 51 - 75% | 5 | 7.4 | ||
| Over 75% | 1 | 1.5 | ||
| Insurance: Self-Insured (%)* | ||||
| less than 10% | 17 | 25.4 | ||
| 10 - 25% | 30 | 44.8 | ||
| 26-50% | 16 | 23.9 | ||
| 51 - 75% | 1 | 1.5 | ||
| Over 75% | 3 | 4.5 | ||
* Data only available for 2012 study.
In the 2012 survey, residents reported an increase in focused training on the medical evaluation of heavy menstrual bleeding during residency with a mean of 15.8+/-22.3 hours per year in the first year of residency and 15.9+/-21.5hours/year in the 2nd year, 15.1+/-20.2 hours/year in the 3rd year and 15.3+/-21.5 hours/year in the 4th year of training. The number of hours specific to this topic was reported by trainees as slightly improved compared to 2010 survey results where the range was from 9-11 hours each year of training. Nonetheless, teaching formats still favored the lecture format (100%) followed by faculty-supervised clinical care (82.4%) even in 2012 (Table 2a).
RESULTS
Correlations Between Physical Features and Body Sway
Between the 3rd trimester and postpartum, there were significant differences in the body weight, BMI, and abdominal circumference (Table 1). Parameters of body sway in the 3rd trimester and postpartum are shown in (Table 2).
Table 2a:: Resident Training.
| 2012 n = 68 | 2010 n = 65 | |
| Outcome | % | % |
| Teaching Formats | ||
| Occasional didactic presentations on Dysfunctional Uterine Bleeding* | 100 | 96.9 |
| Addressed bleeding disorders | 89.7 | 83.1 |
| Systematically taught throughout training | 75 | 67.2 |
| Dysfunctional Uterine Bleeding - Taught in REI | 55.9 | 65.1 |
| Clinical care/evaluation, supervised by faculty* | 100 | 92.2 |
| Clinical care/evaluation, without faculty supervision | 82.4 | 79.7 |
| Taught in Pediatric & Adolescent Gynecology | 44.1 | 43.8 |
| Taught in General Gynecology | 98.5 | 90.8 |
| Training on bleeding disorders to be sufficient? | ||
| Yes | 77.9 | 67.7 |
| No | 14.7 | 21.5 |
| No opinion | 7.4 | 9.2 |
* P-values for test of difference in proportions between 2010 and 2012 * - Indicates no statistical test carried out due to violation of assumptions for difference in binomial proportions (n(p) and n(1-p) >5) No significant differences in proportions were found between 2010 and 2012.
In 2012, the majority of chief residents (77.9%) reported they viewed their training in the medical evaluation of heavy menstrual bleeding and BD as sufficient preparation for clinical practice with an additional 7.4% of participants offering no opinion either way. This was not statistically different from 2010 results where 67.7% of residents felt their training was adequate in this area (p value=0.187) (Table 2b).
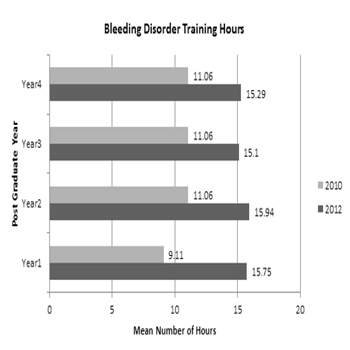
Table 2b: Chief Residents Training.
Practice situation were once again reviewed in the follow up survey. Only 16.2% of chief residents reported performing >50 evaluations during their own residency training which is a decrease the 23% in the 2010 survey. The majority of chief residents (52.9%) reported having performed 20 or fewer evaluations during residency. In 2012 survey, 77.9% of chief residents reported having performed a BD work-up for heavy menstrual bleeding as opposed to 69% in the 2010 survey (Table 3).
Table 3:: Resident Practice.
| 2012 | 2010 | ||
| Outcome | % | % | p* |
| Bleeding Disorder Evaluations performed in Residency | |||
| None | 2.9 | 4.6 | - |
| 01-Oct | 29.4 | 33.8 | NS |
| Nov-20 | 23.5 | 20 | NS |
| 21-30 | 7.4 | 9.2 | NS |
| 31-40 | 13.2 | 3.1 | - |
| 41-50 | 7.4 | 4.6 | - |
| More than 50 | 16.2 | 23 | NS |
| Any menorrhagia work ups this year? | |||
| Yes | 77.9 | 69 | NS |
| No | 20.6 | 26.2 | NS |
| Not sure | 1.5 | 1.5 | - |
| How often do you ask about cycle length? | |||
| Always (100% of the time) | 36.8 | 62.5 | 0.003 |
| Most of the time (< 90%) | 52.9 | 26.6 | 0.002 |
| Usually (70-90%) | 8.8 | 9.4 | NS |
| How often do you ask about days of bleeding? | |||
| Always (100% of the time) | 38.2 | 59.4 | 0.014 |
| Most of the time (<90%) | 52.9 | 31.3 | 0.012 |
| Usually (70-90%) | 7.4 | 7.8 | NS |
| How often do you ask about how # pads/tampons used in a 24 hour period? | |||
| Always (100% of the time) | 48.5 | 23.4 | 0.014 |
| Most of the time (<90%) | 20.6 | 42.2 | 0.007 |
| Usually (70-90%) | 27.9 | 17.2 | NS |
| How often do you ask about post partum hemorrhage? | |||
| Always (100% of the time) | 8.8 | 9.4 | NS |
| Most of the time (< 90%) | 26.5 | 14.1 | NS |
| Usually (70- 90%) | 20.6 | 26.6 | NS |
| Sometimes (50-69%) | 27.9 | 26.6 | NS |
| Less than half the time (1- 49%) | 14.7 | 20.3 | NS |
| How often do you routinely ask about frequent nose bleeds? | |||
| Always (100% of the time) | 1.5 | 1.6 | - |
| Most of the time (<90%) | 4.5 | 3.2 | - |
| Usually (70- 90%) | 7.6 | 4.8 | - |
| Sometimes (50-69%) | 27.3 | 20.6 | NS |
| Less than half the time (1-49%) | 47 | 47.6 | NS |
| Never (0%) | 12.1 | 22.2 | NS |
| How often do you ask about frequent bleeding gums? | |||
| Always (100% of the time) | 1.5 | 1.6 | - |
| Most of the time (< 90%) | 4.5 | 3.2 | - |
| Usually (70- 90%) | 7.6 | 9.5 | NS |
| Sometimes (50-69%) | 24.2 | 23.8 | NS |
| Less than half the time (1- 49%) | 47 | 44.4 | NS |
| Never (0%) | 15.2 | 17.5 | NS |
| How often do you ask about thyroid abnormalities? | |||
| Always (100% of the time) | 12.1 | 17.5 | NS |
| Most of the time (< 90%) | 31.8 | 39.7 | NS |
| Usually (70- 90%) | 28.8 | 15.9 | NS |
| Sometimes (50-69%) | 18.2 | 22.2 | NS |
| Less than half the time (1- 49%) | 9.1 | 4.8 | - |
| How often do you ask about easy bruising? | |||
| Always (100% of the time) | 4.5 | 9.5 | - |
| Most of the time (< 90%) | 15.2 | 17.5 | NS |
| Usually (70- 90%) | 19.7 | 19 | NS |
| Sometimes (50-69%) | 24.2 | 15.9 | NS |
| Less than half the time (1- 49%) | 33.3 | 30.2 | NS |
| Surgical history: How often do you ask about excessive bleeding following tonsillectomy and adenoidectomy? | |||
| Always (100% of the time) | 0 | 6.3 | - |
| Most of the time (< 90%) | 6.1 | 6.3 | - |
| Usually (70- 90%) | 7.6 | 6.3 | - |
| Sometimes (50-69%) | 12.1 | 14.1 | NS |
| Less than half the time (1- 49%) | 37.9 | 29.7 | NS |
| Never (0%) | 36.4 | 37.5 | NS |
| How often do you order an ultrasound with an adolescent with menorrhagia? | |||
| Always (100% of the time) | 6.1 | 9.8 | - |
| Most of the time (< 90%) | 9.1 | 16.4 | NS |
| Usually (70- 90%) | 27.3 | 11.5 | 0.021 |
| Sometimes (50-69%) | 19.7 | 26.2 | NS |
| Less than half the time (1- 49%) | 31.8 | 32.8 | NS |
| Never (0%) | 6.1 | 3.3 | NS |
| Given a history of heavy periods, which of the following would you send routinely? | |||
| CBC | 97.1 | 98.5 | - |
| Factor VIII | 4.4 | 9.2 | - |
| Von Willebrand's Factor | 33.8 | 23.1 | NS |
| TSH thyroid stimulating hormone | 82.4 | 84.6 | NS |
| PT, PTT, INR coagulation panel | 36.8 | 60 | 0.007 |
| PFA100 platelet function analyzer 100 | 1.5 | 3.1 | - |
| Von Willebrand multimers | 2.9 | 6.2 | - |
| Ristocetin cofactor | 5.9 | 1.5 | - |
| TEG thromboelastogram | 0 | 1.5 | - |
| For the following clinical scenarios, what would prompt you to perform a bleeding disorder work-up? | |||
| Menorrhagia at menarche | 80.9 | 84.6 | NS |
| Post partum hemorrhage | 25 | 15.4 | NS |
| Menorrhagia as an adult woman postchild bearing | 33.8 | 23.1 | NS |
* P-values for test of difference in proportions between 2010 and 2012 - Indicates no statistical test carried out due to violation of assumptions for difference in binomial proportions (n(p) and n(1-p) >5).
Regarding basic patient histories, residents were asked about the types of questioning for patients. Cycle length and days of bleeding were commonly cited as the questions they asked "most of the time" by 52.9%of respondents as opposed to 26.6% (P=0.002) and 31.3% (P=0.012) in the 2010 survey (Table 3).Questions assessing whether residents asked about nosebleeds and gum bleeding consistently revealed that residents asked these types of questions less than half the time (47%). Approximately 38% of residents asked about excessive bleeding with tonsillectomy compared to the previous survey in 2010 when a majority reported never asking this question. Residents in the 2012 survey asked about thyroid abnormalities 31.8% of the time, a decrease from the previous study 39.7%, though not significantly different (p=0.342). Easy bruising was a question they asked as often in 2012 as they did in 2010 (Table 3). Routine ultrasounds were not typically ordered as part of work-up for heavy menstrual bleeding among chief residents (11.5%) in 2010, however in 2012 more chief residents tended to order an imaging study (27.3%) (p=0.021) (Table 3). BD work-ups were also assessed by asking which tests would be sent routinely if a clinical scenario requiring the heavy menstrual bleeding work-up arose in a clinical setting. When given the clinical scenarios of heavy menstrual bleeding at menarche, versus post-partum hemorrhage or heavy menstrual bleeding in an adult female, residents were more likely to perform BD evaluation among those with history of heavy menstrual bleeding at menarche; this varied little between 2010 (44.1%) and 2012 (52.3%) and differences were not statistically significant (p value=0.342) (Table 3). OB/GYN chief residents were then asked about situations they thought increased the risk of having underlying BD, even in the absence of a patient specific risk factor. Residents reported being concerned about family history the most in both surveys (89.2% in 2010 versus 73.5% in 2012, p=0.02). In addition, residents assessed whether the presence of certain medical conditions or symptoms related to their likelihood to order a BD workup. Symptoms of concern in the 2012 and 2010 surveys respectively included easy bruising (66.2% versus 89.2%, p=0.002), nosebleeds (58.8% versus 70.8%, p=0.010) and gum bleeding (64.7% versus 89.2%, p=0.001). Medical history of concern identified on the 2012 and 2010 surveys respectively, included chronic renal or liver conditions and thyroid disease, although responses were not statistically different from one survey year to the other (Table 4).
Table 4: Risk Training.
| 2012 | 2010 | ||
| Outcome | % | % | p* |
| Please check the following disorders which may have been included in a training session on evaluation of menorrhagia. | |||
| VWD Type 1 | 72.1 | 78.5 | NS |
| VWD Type 2 | 48.5 | 67.7 | 0.025 |
| VWD Type 3 | 45.6 | 63.1 | 0.043 |
| Bernard Soullier | 10.3 | 3.1 | - |
| ITP Idiopathic thromocytopenic purpura | 57.4 | 78.5 | 0.009 |
| TTP (thrombotic thrombocytopenic purpura) | 54.4 | 72.3 | 0.032 |
| Anemia chronic disease | 57.4 | 63.1 | NS |
| IDA iron deficiency anemia | 67.6 | 7.7 | 0 |
| Blackfan-Diamond syndrome | 2.9 | 1.5 | - |
| Hemophilia | 42.6 | 69.2 | 0.002 |
| Glanzman's thrombasthenia | 7.4 | 4.6 | - |
| Please check those situations which you believe increase the risk for bleeding disorders. | |||
| Family history | 73.5 | 89.2 | 0.02 |
| Menorrhagia only at menarche | 44.1 | 52.3 | NS |
| Menorrhagia anytime | 33.8 | 35.4 | NS |
| Easy bruising | 66.2 | 89.2 | 0.002 |
| Gum bleeds | 64.7 | 89.2 | 0.001 |
| Hematoma development | 41.2 | 43.1 | NS |
| Nosebleeds | 58.8 | 70.8 | NS |
| Blood type | 14.7 | 4.6 | - |
| Thyroid disease | 50 | 60 | NS |
| Other chronic conditions such as renal or liver disease | 55.9 | 76.9 | 0.01 |
* P-values for test of difference in proportions between 2010 and 2012 - Indicates no statistical test carried out due to violation of assumptions for difference in binomial proportions (n (p) and n (1-p) >5).
Many chief residents displayed an awareness that a bleeding condition could improve with hormones (76.9%) or during pregnancy (50%) and could worsen with liver or renal disease (96.2%), aspirin use (96.2%), or no steroidal anti-inflammatory drug use (75%) in the 2012 survey. These were not statistically different from survey responses gathered from the 2010 OB/ GYN resident survey (Table 4). Chief residents reported background knowledge on various BDs as well. When provided a list of various BDs on the 2012 survey, OB/GYN residents reported knowing about the following: VWD Type 1 (72.1%), VWD Type 2 (48.5%), VWD Type 3 (45.6%), idiopathic thrombocytopenic purpura (57.4%), thrombotic thrombocytopenic purpura (54.4%), anemia of chronic disease (57.4%), and hemophilia (42.6%). Residents reported infrequent exposure to other rare conditions such as Glanzmann throm¬basthenia (7.4%) and Bernard-Soulier syndrome (10.3%) (Table 4).
DISCUSSION
The NHLBI developed guidelines for providers potentially caring for women with BDs in 2007. Although specific educational goals and objectives in OB/GYN resident training are outlined, the results of this follow up survey highlight additional opportunities for focused training in this area. Most OB/GYN chief residents viewed their education as being sufficient (77.9% in 2012 and 67.7% in 2010), although some decreases were noted from 2010 to 2012 in areas related to knowledge and practice patterns. The challenges inherent in moving from evidence guidelines to actual implementation of these guidelines into clinical practice as a standard of care are well documented in the professional literature.10-12Green likens the adoption of such guidelines as an extended longitudinal process that is similar to a pipeline that goes from concept development to dissemination of evidence-based findings.10 Cabana and colleagues examined practice logistics related to guideline adoption they highlight the importance of providers in this pipeline process and identifies that some of the barriers to implementation related to providers who may not be aware, familiar or agree with the guideline.11 Shortell and colleagues call for the linking of the evidence-based medicine contained in the guideline to a clinical translation process that is rooted in the management science that informs an effective implementation effort.12 Clearly, practicing providers enter the pipeline as resident trainees so their education on the clinical value of guidelines such as the NHLBI VWD guideline is important to track and monitor. Limitations of the 2012 survey are similar to the 2010 survey and include the use of a non-validated investigator designed questionnaire as well as a low response rate. The questionnaires while not externally validated focused on important provider guidance published in the NHLBI guidelines. Use of a validated survey and future studies confirming these findings will be needed in the future to limit potential interpretation bias namely, confirming that the questions are asking questions reflective of knowledge actual clinical practice. The relatively low response rate could be related to a response bias in that those who responded to this survey view training in BDs as important but the large number of those who did not participate may in fact not view training BDs as important or may not feel confident in their BD knowledge which of course could then skew the results and findings. Future work will likely need to address engaging ways to connect to potential participants so that response rates will be higher and complement the self-reports with actual medical record reviews and observations to confirm actual practice.
CONCLUSION
Although most OB/GYN residents in this survey study were aware of situations that could improve or worsen within a bleeding condition in clinical settings, many were not consistent in the screening for BDs in women with heavy menstrual bleeding. Because heavy menstrual bleeding is one of the common conditions faced by the OB/GYN, the ability to identify which women are at risk for BDs is vital. The results of the 2012 survey compared to the 2010 survey, highlight that continued opportunities exist to improve the education of OB/ GYN residents in the evaluation and treatment of BDs, specifically VWDs that is consistent with the 2007 NHLBI guideline.
IMPACT
Opportunities exist for improved education in the evaluation of heavy menstrual bleeding and bleeding disorders among OB/GYN residents. Although most OB/GYN residents were aware of situations that could improve or worsen within a bleeding condition in clinical settings, many were not consistent in the screening for bleeding disorders in women with heavy menstrual bleeding.
ACKNOWLEDGEMENTS
The authors would like to thank Texas Children's Health Plan for operational support of the survey process and CSL-Behring for an unrestricted educational grant to fund the project.
REFERENCES
- (2014). Office of the Associate Director for Communication, Digital Media Branch, Division of Public Affairs Bleeding Disorders in Women Centers for Disease Control and Prevention.
- (2011). National Heart Blood and Lung Institute. Explore Von Willebrand Disease National Heart Blood and Lung Institute Website.
- Ebrahim SH, Kulkarni R, Parker C and Atrash HK. (2010). Blood Disorders Among Women AM J Prev Med [serial online]. 38(4): S459-S467.
- Lynch T. (2014). Blood Disorders in Women in Home. Centers for Disease Control and Prevention.
- US. Department of Health and Human Services. National Heart, Lung, and Blood Institute of the National Institutes of Health (NHLBI). The Diagnosis, Evaluation and Management of von Willebrand Disease.
- Dietrich JE, Tran XG and Giardino AP. (2011). Bleeding disorder education in obstetrics and gynecology residency training: a national survey. J Pediatr Adolesc Gynecol. 24(2): 94-97.
- Council on Resident Education in Obstetrics and Gynecology (CREOG). Units 4 and CREOG Objectives, 9th Edition. ACOG. Professional Publishing Group, Washington DC.
- Seltzer VL, Fishburne JI and Jonas HS. (1998). Obstetrics and Gynecology Residencies: Education in preventive and primary health care for women. Obstet Gynecol. 91(2): 305-310.
- Teunissen PW, Stapel DA, Scheele F, Scherpbier AJ, et al. (2009). The influence of context on residents’evaluations: effects of priming on clinical judgment and affect. Adv in Health Sci EducTheory Pract. 14(1): 23-41.
- Green L. (2008). Making research relevant: If it is an evidence-based practice, where’s the practice based evidence? Family Practice. 25(suppl 1): 120-124.
- Cabana M, Ebel BE, Cooper-Patrick L, Powe NR, et al. (2000). Barriers Pediatricians Face When Using Asthma Practice Guidelines. Arch Ped Adolesc Med. 154(7): 685- 693.
- Shortell SM, Rundall TG and Hsu J. (2007). Improving Patient Care by Linking Evidence-Based Medicine and Evidence- Based Management. JAMA. 298(6): 673-678.