Information Links
Related Conferences
Previous Issues Volume 7, Issue 3 - 2023
Asia Syndrome and Breast Implants, Report of a Case and Review of the Literature
Victor Manuel Vargas Hernández1,*, Vargas Aguilar Victor Manuel2
1Department of Gynecologic Oncologic, Reproductive Medicine, Mexican Academy of Surgery, Mexico National Academy of Medicine of Mexico
2Gynecologic Oncology National Medical Center Siglo XXI IMSS, Mexico
*Corresponding author: Dr. Víctor Manuel Vargas Hernández, Department of Gynecologic Oncologic, Reproductive Medicine, Mexican Academy of Surgery, Mexico National Academy of Medicine of Mexico, Women’s Health Clinic, Insurgentes Sur 605-1403, Nápoles 03810, Mexico, Tel: (52)5552 179782, E-mail: [email protected].
Received Date: November 28, 2023
Published Date: December 09, 2023
Citation: Vargas-Hernández VM, et al. (2023). Asia Syndrome and Breast Implants, Report of a Case and Review of the Literature. Mathews J Gynecol Obstet. 7(3):31.
Copyrights: Vargas-Hernández VM, et al. © (2023).
ABSTRACT
Background: Over the past decades, evidence has accumulated that autoimmune symptoms can be triggered by exposure to environmental immunostimulatory factors that act as adjuvants in genetically susceptible individuals, with several unexplained symptoms. Adjuvant-induced autoimmune/autoinflammatory syndrome (ASIA) was described in 2011 by Shoenfeld and Agmon-Levin and defined the diagnostic criteria; However, the association of this syndrome with silicone breast implants is controversial. Objective: to describe a case of ASIA syndrome in a silicone breast implant carrier and review of the literature. Clinical Case: JKT 36-year-old woman with luminal infiltrating ductal carcinoma; with negative extension studies, a conservative mastectomy of the skin and areola was performed with immediate reconstruction with an implant with a breast prosthesis and hormone therapy; Her follow-up was torpid with fatigue, pain in the arm, depression, and sleep disturbances and affected breast skin, without infection. As she did not respond to conservative management, it was decided to remove the prosthesis, resection of the capsule and skin, due to the suspicion of the syndrome from ASIA, as there was no involvement or persistence of breast cancer, with immediate improvement. Method: bibliographic review of original articles written in English on cases of ASIA syndromes, associated with silicone breast implants from their description to the present. Results: until 2019, 126 cases of ASIA syndrome due to silicone breast prostheses and implants were reported; Removal of the prosthesis improves symptoms. Conclusions: ASIA syndrome is recent, it is still considered an evolving concept, it is necessary to identify risk factors for the development of autoimmune phenomena in individuals who will receive some type of adjuvant to prevent cases of this syndrome.
Keywords: Silicone Breast Implant Incompatibility Syndrome, Silicone Implant Syndrome, Siliconosis, Autoimmune Dysautonomia, Autoimmunity, Inflammation, Prosthesis, Silicone, Explantation.
BACKGROUND
In 2011 Shoenfeld was first described and Agmon-Levin coined the term Autoimmune/auto-inflammatory/Syndrome Indured by Adjuvants (ASIA) or Shoenfeld syndrome to describe a set of conditions that are the result of an immune response to adjuvants [1-4], present with variable latency time and occur as a result of the interaction between genetic and environmental factors, but the idea of an autoimmune-mediated disease was not new, evidence has accumulated that autoimmune symptoms are triggered by exposure to environmental immune-stimulating factors that act as an adjuvant in susceptible individuals [2,3]. Adjuvants are compounds that, when introduced into the body, develop a specific immune response with high antibody titers against specific pathogens [4]. During the last decade, it became clear that silicone implants act as adjuvants [2,5-8]; The word adjuvant comes from the Latin adjuvare, which means help, a substance capable of increasing the immunogenicity of an antigen without awakening an immune response per se; Some adjuvants contain microbial components and stimulate the innate immune response, simulating a natural infection, while others are based on oils and there are other substances with an adjuvant effect such as silicone. Silicone has been used in many devices including breast prostheses.
The clinical symptoms of ASIA are: chronic fatigue, arthralgias, myalgias, pyrexia, sicca symptoms, cognitive impairment and/or neurological symptoms (atypical) (Table 1; Figure 1). Patients typically present with severe fatigue, non-restorative sleep, and post-exertional malaise. Sleep disorders, such as problems falling asleep and/or staying asleep, are common and poor sleep quality is linked to increased fatigue. Another early symptom is the appearance of arthralgia and in most patients like fibromyalgia [1-3]. Patients often suffer from severe morning stiffness, myalgias and/or muscle weakness. Weakness is severe and leaves the patient bedridden; most patients report fever and night sweats, while others report dry eyes and/or eyes. Dry eyes are often serious and can lead to blurred vision and/or keratitis sicca if left untreated. Symptoms of cognitive impairment are not uncommon [9]: mental confusion, memory deficits, distraction, amnestic or anomic dysphasia, and lack of attention.
In some patients, the neurological manifestations are varied and present cerebrovascular events or events similar to multiple sclerosis; or suffer from allergies and gastrointestinal symptoms such as abdominal pain, hyperperistalsis similar to irritable bowel syndrome. New-onset Raynaud's phenomenon is present, in other cases pain and burning sensations in the skin, secondary to small nerve fiber neuropathy. They may have recurrent hives or ill-defined skin rashes, unexplained pruritus, and/or alopecia. Cardiovascular complaints include signs of orthostatic intolerance, dizziness, and impaired balance; some have interstitial cystitis. The diagnosis is complicated and exclusionary. The clinical history and history are used for suspicion, there is no specific test and magnetic resonance imaging (MRI) is useful for locating the silicone at a distance, presence of granulomas and their distribution in subcutaneous cellular tissue and muscles. The diagnosis of ASIA based on the 12 criteria of Shoenfeld and Agmon-Levin [1] (Table 1).
Table 1. Criteria for the Diagnosis of Autoimmune/Inflammatory Syndrome Induced By Adjuvants (Asia)
MAJOR CRITERIA
Exposure to an external stimulus (implants such as silicone and mesh are classic adjuvants) before clinical manifestations
The appearance of "typical" clinical manifestations such as:
Chronic fatigue, non-restorative sleep, or sleep disorders
Myalgia, myositis or muscle weakness
Arthralgia and/or arthritis
Cognitive impairment, memory loss
Pyrexia
Sicca (dry mouth, dry eyes)
Neurological manifestations (especially associated with demyelination)
Elimination of the inciting agent induces improvement
Typical biopsy of affected organs
MINOR CRITERIA
The appearance of autoantibodies or antibodies directed to the suspected adjuvant.
Other clinical manifestations (i.e., irritable bowel syndrome, Raynaud's phenomenon)
Specific HLA associations (i.e. HLA DRB1, HLA DQB1)
Evolution of an autoimmune disease (i.e., multiple sclerosis, rheumatoid arthritis, Sjogren's syndrome, systemic sclerosis)
The ASIA diagnostic criteria; when two major criteria or one major and two minor criteria are present. New nine diagnostic criteria for ASIA have been proposed by Alijotas-Reig based on objective clinical data, both diagnostic criteria need to be validated. The major criteria are; exposure to external stimulus (biomarkers, vaccines, anilines or other organic and inorganic materials, prior to clinical manifestations; minimum latency time of days (1 to 2 weeks) with regard to vaccines and one month when the trigger involved is not treated of vaccines, for example biomaterials; clinical manifestations; local/regional: inflammatory nodules (cutaneous edema or angio-edema, skin induration, abscesses, lymphadenopathy, panniculitis, morphea, sarcoid-like lesion or systemic: distant inflammatory nodules, arthritis , sicca complex or Sjogren's syndrome, myositis or muscle weakness, extensive panniculitis, demyelinating neological syndromes or evolution to an organ-specific systemic autoimmune disease; biopsy of the involved area or lymph nodes with foreign body characteristics or histopathological findings coexisting with autimmune diseases/ granulomatous; elimination of the triggering agent with improvement; compatible human leukocyte antigens (HLA) (for example HLA B8, HLA N1, HLA DR3, HLA DQB1 or combinations of haplotypes); minor criteria: recent history of triggering factors prior to the onset of clinical manifestations; reticular lividity of recent onset and/or palmar erythema appearing at the beginning of the clinical manifestations; presence of any autoantibody and/or hypergammaglobulinemia and/or elevation of carcinonomatosis antigen and/or elevation of dehydrogenase and/or hypocomplementemia; The presence of 3 major criteria, or 2 major and 2 minor criteria, is required for the diagnosis of ASIA, (Figure 1) [10].
CLINICAL MANIFESTATIONS OF ASIA SYNDROME
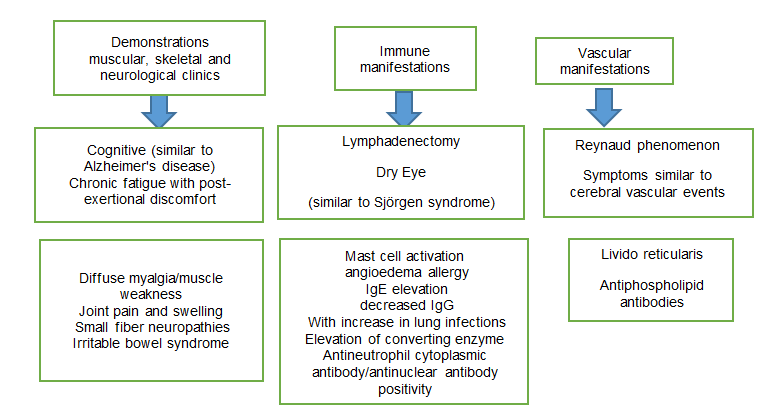
Figure 1. Clinical characteristics of adjuvant-induced autoimmune/inflammatory syndrome (ASIA).
Within the pathophysiology of ASIA syndrome [11]; the use of biomaterials are not immunogenic or toxic; but, they can trigger a foreign body reaction that results in granulomatous inflammation, form microbial biofilms, and chronic inflammatory response; These act as an adjuvant, enhancing the adaptive immune response to autoantigen [12-16]. An implant to the human body, a layer of proteins is absorbed that results in the attraction of phagocytes and leads to the attraction of proteins and phagocytes, by recruitment of mast cells, where histamine influences pain [17].
Leakage and/or rupture of the breast silicone implant leads to an increase in cell apoptosis/necrosis, antigen-presenting cells are activated, T cells are activated and granuloma formation results in lymphadenopathy, production of autoantibodies and clinical manifestations such as fatigue and arthralgia/myalgia [18].
The biomaterial induces a foreign body giant cell reaction, with an immune response that acts as an adjuvant, through several mechanisms: induction of a progressive release of the antigen (Ag) and blocking its elimination, resulting in a longer exposure to antigen presenting cells (APC); promotion of Ag translocation to lymph nodes where Ag can be recognized by T cells; conversion of soluble Ag into particulate form, which is subsequently phagocytosed by APCs such as macrophages, dendritic cells (DCs), and B cells; stimulates induction of inflammatory cytokine release and interaction with Toll-like receptors (TLRs) and nucleotide oligomerization domain-like receptors, including the inflammasome pathway NALP3 inflammasome, a multiprotein signaling complex containing NALP3 and ASC, an adapter protein, responsible for the activation of intracellular enzymes that lead to the production of inflammatory cytokines from immune cells, including IL1β and IL18 through the activation of caspase 1 [19]. The NALP3 inflammasome is a primary sensing mechanism by which debris such as silicones and induce the secretion of proinflammatory cytokines and recruit myeloid lineage cells, these adjuvants are capable of immune memory. T cells and B cells contain the amnesic characteristics of acquired immune memory through selective programming and dating of specific lymphocyte clones, these cells play a fundamental role in the recruitment, activation and effector functions of other cells of the immune system, continuous process through cellular and molecular crosstalk. Lymphocytes often dominate implant-associated ectopic lymphoid structures. Pattern recognition receptors, such as Toll-like receptor 4 (TLR4), serve as critical triggers of inflammation upon recognition of endogenous alarm molecules released by injured tissues, such as heat shock proteins, biglycan fragments, and Heparan sulfate adjuvants directly activate TLR4, promoting local inflammation and tissue remodeling through NFkB-mediated cytokine production [19,20], the release of alarm signals from injured host tissues connects initial implantation to immediate innate inflammatory and immune responses; tissue injury, presenting as necrosis in association with failed or compromised implants, may perpetuate these maladaptive pathways; The association between ASIA syndrome and breast implants results in the activation of mast cells, macrophages and, subsequently, inflammasomes, which leads to the production of cytokines such as interleukin-1β. Reactive oxygen species (ROS) and reactive nitrogen species are also produced. Subsequently, macrophage apoptosis occurs and neutrophils are attracted. These neutrophils become activated, produce ROS, and release enzymes such as myeloperoxidase. In addition, implant materials are transported to regional lymph nodes, resulting in a pronounced adjuvant effect, implants such as silicone breast implants and have been shown to induce an adjuvant effect and increase susceptibility and/or exacerbate autoimmune diseases [19]. Silicones trigger a histiocytic reaction with foreign body giant cells that form granulomas locally trigger an immune response through activated TH1/TH17 cells, indicating that the resulting fibrosis is promoted by the production of inflammatory cytokines such as IL-17, IL-6, IL-8 and other growth factors as a consequence of impaired local regulatory T cell function. Patients with ASIA syndrome to breast implants often have humoral immunodeficiencies and a suppression of natural killer cell activity [21]; Exposure to small silicone particles can induce cell death [22], indicating that immune cells are destroyed by silicones and these not only deposit around the capsule, but migrate through the periprosthetic capsule to distant sites [23-25]. The formation of biofilms with Propionibacterium acnes and/or Staphylococcus epidermidis in 6 to 36%, causes chronic indolent infection and causes systemic symptoms (Figure 2) [19].
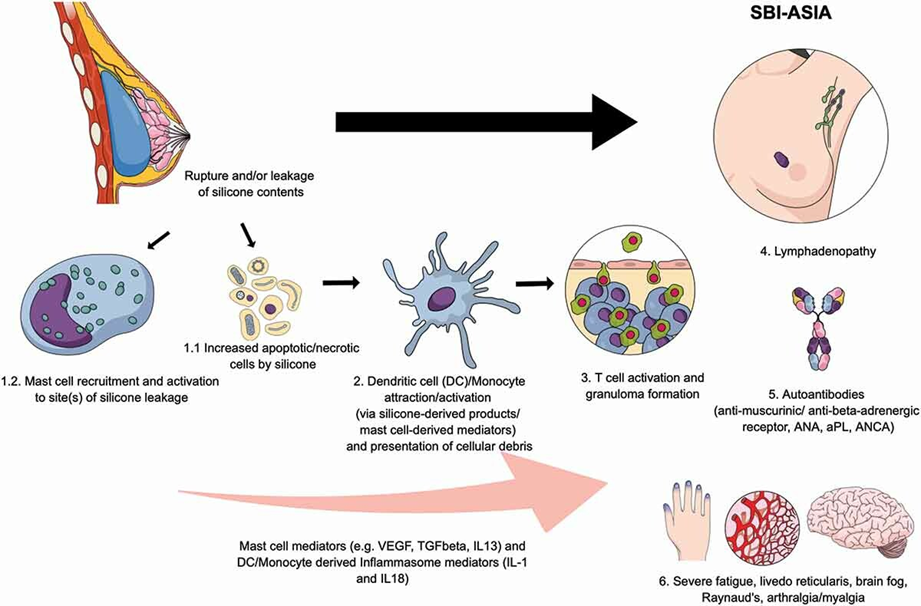
Figure 2. Pathophysiology of ASIA syndrome associated with breast implants
CASE REPORT
JKT 36-year-old woman, with a history of hypertensive mother, surgery for right ovarian tumor due to endometrioma; menarche at 9 years old, last menstruation February 7, 2023, regular rhythm with dysmenorrhea, cyclical mastalgia, pregnancies 7 spontaneous abortions 5 cesarean sections 2, one pregnancy obtained by assisted reproduction technique, lactation for 3 to 6 months in each pregnancy; adequate cervical cancer screening; She began her current condition since November 2022 with the detection of a breast tumor that was performed with an excisional breast biopsy with a report of multifocal lobular carcinoma of 5cm and another of 3cm; grade 2 infiltrating ductal carcinoma without specific pattern measuring 20x14mm with comedo-type and solid ductal component in situ, without lymphovascular invasion and non-assessable margins (Figure 3). Estrogen receptors 70% and progesterone 5% HER-2neu negative, ki67 20%; According to the molecular classification, it is luminal type; with extension and bilateral studies (mammography, ultrasound of the breast, liver and magnetic resonance imaging of the breast without involvement, a negative sentinel lymph node biopsy Figure 4, was performed and a skin and areola-conserving mastectomy Figures 5 & 6) was proposed with immediate reconstruction with implant with a breast prosthesis; the diagnosis of grade 2 infiltrating ductal breast cancer of luminal type pT1c pN0 due to negative M0 sentinel lymph node by imaging, pathology report without evidence of infiltrating neoplasia in the mammary gland, only hyalinized breast fibroadenoma, adenosis, metaplasia, ectasia, granulomatous mastitis without microorganisms; he evaluation together with radio oncology and medical oncology for adjuvant management, only required hormotherapy with tamoxifen; during follow-up; the patient presented dehiscence of the surgical wound and the margins widened (Figures 7 & 8) with a pathology report without lesion on the resected skin. Continues with fatigue, sleep disorders, pain in the arm, depression, and alterations in the skin of the affected breast, without signs of infection. As it does not respond to conservative management, it is decided to remove the prosthesis and resection of the capsule and skin, with the suspicion of ASIA syndrome, as there is no involvement or persistence of breast cancer; with immediate (Figure 9) but irregular improvement (Figure 10).
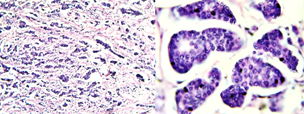
Figure 3. Tumor size: 2.0 x 1.1cm, hispathological type: Invasive ductal carcinoma (NOS), grade 2, moderately differentiated with SBR sum: 7 or Grade 3 ductal differentiation.
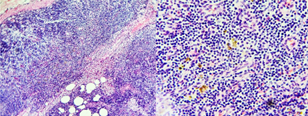
Figure 4. Histopathological study of the sentinel node biopsy negative for macrometastasis, with paracortical hyperplasia and data of dermatopathic lymphadenopathy.

Figure 5. macroscopic mammary gland, con chronic granulomatous mastitis.

Figure 6. immediate post-surgical skin-sparing mastectomy with prosthesis.

Figure 7. inflammation and wound dehiscence 15 days after prosthesis.

Figure 8. preoperative inflammatory disease of prosthesis removal.

Figure 9. Adequate healing 6 months after surgery.

Figure 10. Reactivation of granulomatous mastitis at 7 months.
ASIA SYNDROME DUE TO MEDICAL IMPLANTS
After the description of ASIA Syndrome in 2011 [1], the expansion and recognition of this syndrome by different countries began, providing the clinical and experimental bases to support the existence of ASIA. More than a decade has passed since the initial description of ASIA syndrome and new cases of ASIA have been described and new adjuvants added, they may be associated with the development of ASIA syndrome after the injection of bioimplants for aesthetic purposes, such as hyaluronic acid, methacrylate, polyacrylamide, polyalkylimide and metals in implants as used in orthopedic surgery and/or in contraceptive devices [11-15]. Supporting evidence from the literature underlines the development of ASIA in susceptible patients after breast or testicular implants, rhinoplasty, polypropylene mesh implantation for hernia repair or for reinforcement of pelvic floor dysfunction, band implantation tension-free vaginal for stress urinary incontinence, sterilizations with Essure, implantation of prosthetic materials for arthroplasty, and/or metal implants in orthopedic surgery [2,8,15,19] (Figure 11).
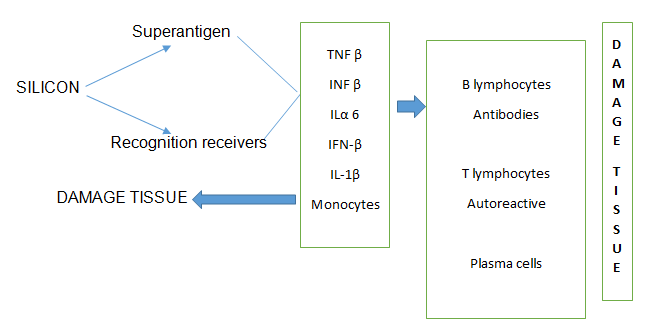
Figure 11. Mechanism by which ASIA Syndrome develops, associated with a silicone implant or prosthesis: the presence of silicone, coupled to antibodies through receptors, triggers the release of cytosines, which cause tissue damage that, in turn, cells of the endothelial reticulum increase the damage.
The susceptibility for the development of ASIA after medical device implantation has not been elucidated [2]. Patients with a history of allergy are at increased risk of developing ASIA after implantation or established autoimmune disease or familial predisposition or autoimmune disease are at risk of developing symptoms after silicone breast implantation (SBI). It is important to take into account the interaction between immunogenetic factors; HLA, as well as environmental factors such as smoking and obesity in the development of medical device-induced ASIA.
In general, biomaterials used for implantation are non-immunogenic and non-toxic, implanted biomaterials trigger foreign body reaction (FBR) resulting in granulomatous inflammation [16]. Immediately after implantation of a biomaterial, a layer of host proteins is absorbed, resulting in the attraction of phagocytes (predominantly macrophages of the proinflammatory M1 subtype) [17]. Such a process depends on the presence of activated mast cells and histamine, which plays a fundamental role in the pain, sometimes severe, at the implantation site secondary to sensitization of the transient reporter potential V1 (TRPV1) channel, a nociceptor ending in the cells that detect pain sensations and transmit them to other areas of the central nervous system [18], microbial biofilms form on implants [15,16] and contribute to the chronic inflammatory response. It is important to highlight that the biomaterial delivers a danger signal to the immune system and gives rise to a greater immune response; biomaterials act as an adjuvant in the development of an adaptive immune response to an antigen [2].
The susceptibility for the development of ASIA after medical device implantation has not been elucidated [2]. Patients with a history of allergy are at increased risk of developing ASIA after implantation or established autoimmune disease or familial predisposition or autoimmune disease are at risk of developing symptoms after silicone breast implantation (SBI). It is important to take into account the interaction between immunogenetic factors; HLA, as well as environmental factors such as smoking and obesity in the development of medical device-induced ASIA.
In general, biomaterials used for implantation are non-immunogenic and non-toxic, implanted biomaterials trigger foreign body reaction (FBR) resulting in granulomatous inflammation [16]. Immediately after implantation of a biomaterial, a layer of host proteins is absorbed, resulting in the attraction of phagocytes (predominantly macrophages of the proinflammatory M1 subtype) [17]. Such a process depends on the presence of activated mast cells and histamine, which plays a fundamental role in the pain, sometimes severe, at the implantation site secondary to sensitization of the transient reporter potential V1 (TRPV1) channel, a nociceptor ending in the cells that detect pain sensations and transmit them to other areas of the central nervous system [18], microbial biofilms form on implants [17,18] and contribute to the chronic inflammatory response. It is important to highlight that the biomaterial delivers a danger signal to the immune system and gives rise to a greater immune response; biomaterials act as an adjuvant in the development of an adaptive immune response to an antigen [2].
An important major criterion of ASIA includes improvement of symptoms and signs that occurred after explantation (such as chronic fatigue or widespread pain) after explantation, which is the technique of removing the Implants within the capsule that surround them, completely eliminating all tissue associated with the Implants, and avoiding contamination in the event of rupture, silicone spillage or presence of liquid inside the capsules (Figure 7) The cessation or reduction of symptoms after removal (also called dechallenge or interruption of procedures or administration of medications due to adverse events) is an extremely important observation in the diagnosis of ASIA, as well as in determining causality. Such improvement has been documented in patients with silicone breast implants [25-28], mesh implants [8]. Contraceptive devices such as Essure [11], arthroplasty [19] and/or metal implants; symptoms after SBI explantation [18]; 75% experience general improvement [17,18,20-29], improvement of symptoms in 50-98% of patients and a significant improvement occurred in 30% of patients undergoing explantation, compared to patients without excision only 12% reported improvement significant (OR = 2.86; CI 1.31–6.24) [29].
In one report, 60% of their patients did not want to undergo an explantation. The most common reasons for this were costs (64%) and/or cosmetic reasons (30%); not all patients with SBI benefit from explantation; Several factors influence, for example, implant characteristics, disease characteristics, duration, surgery, post-explantation reconstruction and/or other factors. Breast implants may have a different filling material (silicone, hydrocellulose or saline), a different external silicone shell that has a smooth surface or a textured surface and different shape (round or anatomical) [25]. Not much is known about these characteristics and the outcome after explantation. capsular inflammation was more present in silicone gel-filled implants compared to saline implants, while capsular inflammation was more severe in implants with a textured surface compared to smooth implant patients [22], patients with contracture capsular implants had a significantly better result than without it, the improvement is similar in symptoms between the extraction of implants filled with saline solution and silicone gel [21].
An important major criterion of ASIA includes improvement of symptoms and signs that occurred after explantation (such as chronic fatigue or widespread pain) after explantation, which is the technique of removing the Implants within the capsule that surround them, completely eliminating all tissue associated with the Implants, and avoiding contamination in the event of rupture, silicone spillage or presence of liquid inside the capsules (Figure 11) The cessation or reduction of symptoms after removal (also called dechallenge or interruption of procedures or administration of medications due to adverse events) is an extremely important observation in the diagnosis of ASIA, as well as in determining causality. Such improvement has been documented in patients with silicone breast implants [17,18,20-29], mesh implants [8]. Contraceptive devices such as Essure [11], arthroplasty [19] and/or metal implants; symptoms after SBI explantation [17]; 75% experience general improvement [18-29], improvement of symptoms in 50-98% of patients and a significant improvement occurred in 30% of patients undergoing explantation, compared to patients without excision only 12% reported improvement significant (OR = 2.86; CI 1.31–6.24) [29].
In one report, 60% of their patients did not want to undergo an explantation. The most common reasons for this were costs (64%) and/or cosmetic reasons (30%); not all patients with SBI benefit from explantation; Several factors influence, for example, implant characteristics, disease characteristics, duration, surgery, post-explantation reconstruction and/or other factors. Breast implants may have a different filling material (silicone, hydrocellulose or saline), a different external silicone shell that has a smooth surface or a textured surface and different shape (round or anatomical) [25]. Not much is known about these characteristics and the outcome after explantation. capsular inflammation was more present in silicone gel-filled implants compared to saline implants, while capsular inflammation was more severe in implants with a textured surface compared to smooth implant patients [22], patients with contracture capsular implants had a significantly better result than without it, the improvement is similar in symptoms between the extraction of implants filled with saline solution and silicone gel [21].
Some patients with SBI develop autoimmune diseases such as Sjogren's syndrome, sarcoidosis, systemic sclerosis, rheumatoid arthritis, systemic lupus erythematosus, antiphospholipid syndrome, eosinophilic granulomatosis with polyangiitis and/or other different forms of vasculitis [20]. Women with breast implants had a 45% higher risk of being diagnosed with at least one autoimmune/rheumatic disorder, compared to those without breast implants [30]. In patients with medical implant-induced ASIA with a systemic autoimmune disease, recovery after explantation is often not complete and they require immunomodulators [17]. Although improvement in systemic symptoms occurred with increasing implantation time, it decreased with the duration of exposure to SBI [29]. 59% of women who removed their implants within 10 years after implantation showed significant improvement, only 33% with more than 10 years.
There is controversy about whether SBI explantation should be accompanied by a scapustomy [27,28] with or without this, the symptoms improved in both groups. The improvement was more pronounced with capsulectomy and almost all improved after explantation [21-23]. After explantation, a new implant (saline, hydrocellulose, or silicone gel filling) may be placed, reconstruction may be performed with autologous material, or no reconstruction may be performed. Initial improvement was 72% for women without reconstruction, 68% for women with a new implant versus 72% for women with autologous reconstruction. Relapses occurred frequently (47%) with a new implant, a low relapse rate if no reconstruction was performed and a high relapse rate when new implants (saline) were placed (46% relapse). Many other factors such as smoking, age, body mass index (BMI), and/or comorbidities affect outcomes after explantation; in obese patients resulted in greater improvement [21], since obesity is a pro-inflammatory condition.
Women who developed symptoms after breast implantation have significant improvement in symptoms and quality of life when their breast implants are removed. Improvement in ASIA syndrome symptoms (fatigue, arthralgia, muscle pain and weakness, cognitive impairment, alopecia, generalized pain, and allergies) after breast implant removal; There is evidence that ASIA syndrome in patients with a medical device such as implants is caused by them [31]. The association with autoantibodies directed against receptors of the autonomic nervous system. Silicone can cause autonomic manifestations and leads to a condition of autoimmune dysautonomia in genetically predisposed subjects [32,33]. Silicone breast implant incompatibility syndrome (SIIS) is a classic example of dysautonomia condition induced by ASIA syndrome in genetically predisposed subjects [34]. Silicone adjuvant can cause chronic stimulation of both the innate and adaptive immune systems, resulting in the production of classical autoantibodies and, occasionally, the development of a rare type of T-cell lymphoma [35]. A significant increase in the development of various autoimmune and rheumatic diseases was demonstrated in women with silicone breast implants (SBI) [30]. Women with SBI may suffer from a wide variety of autonomic manifestations, such as palpitations, dry eyes and mouth, depression, chronic fatigue, generalized pain, cognitive impairment, hearing loss, etc. [2,32]. Unfortunately, most doctors ignore these subjective symptoms; with normal laboratory tests, significant changes have been observed in the circulating level of non-classical autoantibodies directed against G protein-coupled receptors (GPCRs) of the autonomic nervous system (such as: anti-β1 adrenergic, anti-endothelin type A receptor and anti-angiotensin II type 1 receptor) in symptomatic women with SBI compared to healthy women [32,36,37], dysregulation in the level and function of these anti-GPCR autoantibodies explains some of the subjective/autonomic manifestations reported by women with SBI. It is noteworthy that the elimination of SBI in these symptomatic subjects, as one of the main criteria of ASIA syndrome [1], leads to a clear improvement, strengthening the introduction of SIIS as a classic example of ASIA syndrome [34].
Women who developed symptoms after breast implantation have significant improvement in symptoms and quality of life when their breast implants are removed. Improvement in ASIA syndrome symptoms (fatigue, arthralgia, muscle pain and weakness, cognitive impairment, alopecia, generalized pain, and allergies) after breast implant removal; There is evidence that ASIA syndrome in patients with a medical device such as implants is caused by them [31]. The association with autoantibodies directed against receptors of the autonomic nervous system. Silicone can cause autonomic manifestations and leads to a condition of autoimmune dysautonomia in genetically predisposed subjects [32,33]. Silicone breast implant incompatibility syndrome (SIIS) is a classic example of dysautonomia condition induced by ASIA syndrome in genetically predisposed subjects [34]. Silicone adjuvant can cause chronic stimulation of both the innate and adaptive immune systems, resulting in the production of classical autoantibodies and, occasionally, the development of a rare type of T-cell lymphoma [35]. A significant increase in the development of various autoimmune and rheumatic diseases was demonstrated in women with silicone breast implants (SBI) [30]. Women with SBI may suffer from a wide variety of autonomic manifestations, such as palpitations, dry eyes and mouth, depression, chronic fatigue, generalized pain, cognitive impairment, hearing loss, etc. [2,32]. Unfortunately, most doctors ignore these subjective symptoms; with normal laboratory tests, significant changes have been observed in the circulating level of non-classical autoantibodies directed against G protein-coupled receptors (GPCRs) of the autonomic nervous system (such as: anti-β1 adrenergic, anti-endothelin type A receptor and anti-angiotensin II type 1 receptor) in symptomatic women with SBI compared to healthy women [32,36,37], dysregulation in the level and function of these anti-GPCR autoantibodies explains some of the subjective/autonomic manifestations reported by women with SBI. It is noteworthy that the elimination of SBI in these symptomatic subjects, as one of the main criteria of ASIA syndrome, leads to a clear improvement, strengthening the introduction of SIIS as a classic example of ASIA syndrome [34].
DISCUSSION
Since 1899, the use of paraffin as a prosthesis and treatment of conditions such as cleft lip and palate demonstrated the appearance of granulomatous and fibrous reactions in response to contact with said substance. Subsequently, starting in 1940 with the growth of aesthetic medicine and widespread use of liquid silicone as a modeling substance, led to the appearance of responses similar to those reported with the use of paraffin, the incidence of cases of autoimmune diseases increased. After the description of the ASIA Syndrome in 2011 [1,38-45], the expansion and recognition of this syndrome by different countries began, providing the clinical and experimental bases to support the existence of ASIA. More than a decade has passed since the initial description of ASIA syndrome and new cases of ASIA have been described and new adjuvants added, they may be associated with the development of ASIA syndrome after the injection of bioimplants for aesthetic purposes, such as hyaluronic acid, methacrylate, polyacrylamide, polyalkylimide and metals in implants as used in orthopedic surgery and/or in metallic contraceptive devices [11].
Nonspecific systemic manifestations, the term siliconosis was coined, is characterized by a spectrum of diseases that can affect several organs. It is a musculoskeletal pain syndrome characterized by overwhelming fatigue, arthralgias and myalgias, silicone implant syndrome; little recognized condition in emerging countries with increased prevalence, this disorder was described in various ways, the clinical syndrome associated with patients receiving silicone gel in liquid or encapsulated form; The term siliconosis includes symptomatic women who were exposed to silicone gel through injection or implant placement [46-48].
Silicone develops an inflammatory response in the host, conditioning the formation of a reaction against a foreign body and immunomodulation that ends in specific manifestations. The clinical picture is characterized by peripheral, non-erosive arthralgias, myalgias, chronic fatigue, development of granulomatous lesions at the inoculated site, formation of silicone tumors with an inflammatory response in distant sites, changes in the patient's anatomy and neurological manifestations that they range from cognitive impairment to symptoms of focus and loss of consciousness.
Since its description, ASIA syndrome has been widely and recognized; have been associated with new adjuvants (for example, polypropylene meshes). New subtypes of ASIA syndrome have been introduced, related to exposure to different types of vaccines (e.g., human papillomavirus and COVID vaccines) in genetically predisposed individuals, i.e., HLA DRB1 haplotypes. Recent evidence describing a clear association between removal of a specific adjuvant (e.g., silicone implants, mesh, Essure sterilization devices, metal implants, or even porcelain-fused-to-metal dental crowns) followed by relief/disappearance of symptoms in patients with ASIA syndrome, strengthens some of the criteria for ASIA syndrome.
The treatment of ASIA is based on the elimination of the external stimulus (for example, silicone implants). In most cases, a favorable long-term response is observed without the need to start immunomodulatory treatment. Evolution to autoimmune/autoinflammatory diseases requires starting treatment. immunomodulator; its long-term prognosis of patients diagnosed with ASIA has not been evaluated; It is recommended to avoid re-exposure to the adjuvant involved due to the theoretical risk of re-triggering or exacerbating the immune response [19].
CONCLUSION
The concept of ASIA syndrome is recent, it is evolving, with a greater incidence when silicone is used in prostheses; now it is more frequent and makes it necessary to investigate the biological mechanisms, diagnostic criteria to identify risk factors for its prevention.
REFERENCES
- Shoenfeld Y, Agmon-Levin N. (2011). 'ASIA'-autoimmune/inflammatory syndrome induced by adjuvants. J Autoimmun. 36(1):4-8.
- Caldeira M, Caldeira Ferreira A. (2012). Siliconosis: Autoinmune /inflamatory syndrome induced by adjuvants (ASIA). ISR Med Assoc J. 14(2):137-138.
- Torres-Ruíz JJ, Martín NE, López-Íñiguez A, et al. (2016). Sindrome Autoinmune/auntoinflamatorio inducido por adyuvantes (ASIA). Rev Med MD. 7(3):170-181.
- Cordel E, Reix N, Mathelin C. (2020). Le syndrome ASIA associé aux implants mammaires: lien de causalité ou association fortuite ? [ASIA syndrome associated with breast implants: Fortuitous link or association?]. Gynecol Obstet Fertil Senol. 48(10):754-762.
- Cohen Tervaert JW. (2018). Autoinflammatory/autoimmunity syndrome induced by adjuvants (ASIA; Shoenfeld’s syndrome): a new flame. Autoimmun Rev. 17(12):1259-1264.
- Segal Y, Dahan S, Sharif K, Bragazzi NL, Watad A, Amital H. (2018). The value of Autoimmune Syndrome Induced by Adjuvant (ASIA)-Shedding light on orphan diseases in autoimmunity. Autoimmun Rev. 17(5):440-448.
- See FDA report on Breast Implant Special Topics from Advisory Panel, March 25th and 26th (2019). https://www.fda.gov/media/122956/download.
- Cohen Tervaert JW. (2018). Autoinflammatory/autoimmunity syndrome induced by adjuvants (Shoenfeld’s syndrome) in patients after a polypropylene mesh implantation. Best Pract Res Clin Rheumatol. 32(4):511-520.
- Colaris MJL, Cohen Tervaert JW, Ponds RWHM, Wilmink J, van der Hulst RRWJ. (2021). Subjective Cognitive Functioning in Silicone Breast Implant Patients: A Cohort Study. Plast Reconstr Surg Glob Open. 9(2):e3394.
- Watad A, Quaresma M, Brown S, Cohen Tervaert JW, Rodríguez-Pint I, Cervera R, et al. (2017). Autoimmune/inflammatory syndrome induced by adjuvants (Shoenfeld's syndrome)-An update. Lupus. 26(7):675-681.
- Vaz R, Xavier P, Brito S, Dantas J, Duque S, Consciência JG, et al. (2019). Metallosis: A New Form of Autoimmune/Autoinflammatory Syndrome Induced by Adjuvants Syndrome (ASIA)? Eur J Case Rep Intern Med. 6(3):001034.
- Major MR, Wong VW, Nelson ER, Longaker MT, Gurtner GC. (2015). The foreign body response: at the interface of surgery and bioengineering. Plast Reconstr Surg. 135(5):1489-1498.
- Langbach O, Kristoffersen AK, Abesha-Belay E, Enersen M, Røkke O, Olsen I. (2016). Oral, intestinal, and skin bacteria in ventral hernia mesh implants. J Oral Microbiol. 8:31854.
- Lee M, Ponraja G, McLeod K, Chong S. (2020). Breast Implant Illness: A Biofilm Hypothesis. Plast Reconstr Surg Glob Open. 8(4):e2755.
- Nolfi AL, Brown BN, Liang R, Palcsey SL, Bonidie MJ, Abramowitch SD, Moalli PA. (2016). Host response to synthetic mesh in women with mesh complications. Am J Obstet Gynecol. 215(2):206.e1-8.
- Wouters MM, Balemans D, Van Wanrooy S, Dooley J, Cibert-Goton V, Alpizar YA, et al. (2016). Histamine Receptor H1-Mediated Sensitization of TRPV1 Mediates Visceral Hypersensitivity and Symptoms in Patients With Irritable Bowel Syndrome. Gastroenterology. 150(4):875-887.
- Deva AK, Cuss A, Magnusson M, Cooter R. (2019). The “Game of Implants”: a perspective on the crisis-prone history of breast implants. Aesth Surg J. 39(S1):S55–S65.
- Dowling JK, Mansell A. (2016). Toll-like receptors: the swiss army knife of immunity and vaccine development. Clin Transl Immunology. 5(5):e85.
- Cohen Tervaert JW, Mohazab N, Redmond D, van Eeden C, Osman M. (2022). Breast implant illness: scientific evidence of its existence. Expert Rev Clin Immunol. 18(1):15-29.
- Grammatopoulos G, Munemoto M, Inagaki Y, Tanaka Y, Athanasou NA. (2016). The Diagnosis of Infection in Metal-on-Metal Hip Arthroplasties. J Arthroplasty. 31(11):2569-2573.
- Todorov TI, de Bakker E, Smith D, Langenberg LC, Murakata LA, Kramer MHH, et al. (2021). A Case of Silicone and Sarcoid Granulomas in a Patient with "Highly Cohesive" Silicone Breast Implants: A Histopathologic and Laser Raman Microprobe Analysis. Int J Environ Res Public Health. 18(9):4526.
- Castro C, Fernandes D, Mendonça M, Roveda Junior D, Badan G, Fleury EFC. (2020). Silicone-induced granuloma of breast implant capsule mimicking anaplastic large cell lymphoma. Breast J. 26(5):1028-1030.
- Dijkman HBPM, Slaats I, Bult P. (2021). Assessment of Silicone Particle Migration Among Women Undergoing Removal or Revision of Silicone Breast Implants in the Netherlands. JAMA Netw Open. 4(9):e2125381.
- Wee CE, Younis J, Isbester K, Smith A, Wangler B, Sarode AL, et al. (2020). Understanding Breast Implant Illness, Before and After Explantation: A Patient-Reported Outcomes Study. Ann Plast Surg. 85(S1 Suppl 1):S82-S86.
- Katsnelson JY, Spaniol JR, Buinewicz JC, Ramsey FV, Buinewicz BR. (2021). Outcomes of Implant Removal and Capsulectomy for Breast Implant Illness in 248 Patients. Plast Reconstr Surg Glob Open. 9(9):e3813.
- De Miranda RE. (2020). En bloc explant of silicone breast prostheses and quality of life and evolution of ASIA syndrome symptoms. Rev Bras Cir Plast. 35(4):427-431.
- Magno-Padron DA, Luo J, Jessop TC, Garlick JW, Manum JS, Carter GC, et al. (2021). A population-based study of breast implant illness. Arch Plast Surg. 48(4):353-360.
- Valente DS, Itikawa WM, Catherino F, Votto R, Groth A. (2022). Breast silicone explant: a multicenter longitudinal study. Rev Bras Cir Plást. 37(2):154-162.
- Onnekink C, Kappel RM, Boelens WC, Pruijn GJM. (2020). Low molecular weight silicones induce cell death in cultured cells. Sci Rep. 10(1):9558.
- Glicksman C, McGuire P, Kadin M, Lawrence M, Haws M, Newby J, et al. (2022). Impact of Capsulectomy Type on Post-Explantation Systemic Symptom Improvement: Findings From the ASERF Systemic Symptoms in Women-Biospecimen Analysis Study: Part 1. Aesthet Surg J. 42(7):809-819.
- Bird GR, Niessen FB. (2022). The effect of explantation on systemic disease symptoms and quality of life in patients with breast implant illness: a prospective cohort study. Sci Rep. 12(1):210.
- Watad A, Rosenberg V, Tiosano S, Cohen Tervaert JW, Yavne Y, Shoenfeld Y, et al. (2018). Silicone breast implants and the risk of autoimmune/rheumatic disorders: a real-world analysis. Int J Epidemiol. Dec 1;47(6):1846-1854.
- Jara LJ, Vera-Lastra O, Mahroum N, Pineda C, Shoenfeld Y. (2022). Autoimmune post-COVID vaccine syndromes: does the spectrum of autoimmune/inflammatory syndrome expand? Clin Rheumatol. 41(5):1603-1609.
- Halpert G, Watad A, Tsur AM, Dotan A, Quiros-Lim HE, Heidecke H, et al. (2021). Autoimmune dysautonomia in women with silicone breast implants. J Autoimmun. 120:102631.
- Halpert G, Amital H, Shoenfeld Y. (2022). Silicone Breast Illness as a Classical Example of Autoimmune/Inflammatory Syndrome Induced by Adjuvant (ASIA). Isr Med Assoc J. 24(6):357-359.
- Watad A, Bragazzi NL, Amital H, Shoenfeld Y. (2019). Hyperstimulation of Adaptive Immunity as the Common Pathway for Silicone Breast Implants, Autoimmunity, and Lymphoma of the Breast. Isr Med Assoc J. 21(8):517-519.
- Cabral-Marques O, Riemekasten G. Functional autoantibodies targeting G protein-coupled receptors in rheumatic diseases. Nat Rev Rheumatol. 2017 Nov;13(11):648-656.
- Cabral-Marques O, Marques A, Giil LM, De Vito R, Rademacher J, Günther J, et al. (2018). GPCR-specific autoantibody signatures are associated with physiological and pathological immune homeostasis. Nat Commun. 9(1):5224.
- Shoenfeld Y, Ryabkova VA, Scheibenbogen C, Brinth L, Martinez-Lavin M, Ikeda S, et al. (2020). Complex syndromes of chronic pain, fatigue and cognitive impairment linked to autoimmune dysautonomia and small fiber neuropathy. Clin Immunol. 214:108384.
- Wallukat G, Hohberger B, Wenzel K, Fürst J, Schulze-Rothe S, Wallukat A, et al. (2021). Functional autoantibodies against G-protein coupled receptors in patients with persistent Long-COVID-19 symptoms. J Transl Autoimmun. 4:100100.
- Cabral-Marques O, Halpert G, Schimke LF, Ostrinski Y, Vojdani A, Baiocchi GC, et al. (2022). Autoantibodies targeting GPCRs and RAS-related molecules associate with COVID-19 severity. Nat Commun. 13(1):1220.
- Goebel A, Krock E, Gentry C, Israel MR, Jurczak A, Urbina CM, et al. (2021). Passive transfer of fibromyalgia symptoms from patients to mice. J Clin Invest. 131(13):e144201.
- Scheibenbogen C, Loebel M, Freitag H, Krueger A, Bauer S, Antelmann M, et al. (2018). Immunoadsorption to remove ß2 adrenergic receptor antibodies in Chronic Fatigue Syndrome CFS/ME. PLoS One. 13(3):e0193672.
- Basantsova NY, Starshinova AA, Dori A, Zinchenko YS, Yablonskiy PK, Shoenfeld Y. (2019). Small-fiber neuropathy definition, diagnosis, and treatment. Neurol Sci. 40(7):1343-1350.
- Gavrilova N, Starshinova A, Zinchenko Y, Kudlay D, Shapkina V, Malkova A, et al. (2021 ). Small Fiber Neuropathy in Sarcoidosis. Pathophysiology. 28(4):544-550.
- Muramatsu Y, Fukushima U, Kudo S, Akatsuka T, Ono K, Hirao H. (2021). Silicone allergy associated with intraocular silicone ball prosthesis in a dog. Can Vet J. 62(11):1185-1189.
- Hoeijmakers JGJ, Merkies ISJ, Faber CG. (2022). Small fiber neuropathies: expanding their etiologies. Curr Opin Neurol. 35(5):545-552.
- Soriano A, Nesher G, Shoenfeld Y. (2015). Predicting post-vaccination autoimmunity: who might be at risk? Pharmacol Res. 92:18-22.
- Arango MT, Perricone C, Kivity S, Cipriano E, Ceccarelli F, Valesini G, Shoenfeld Y. (2017). HLA-DRB1 the notorious gene in the mosaic of autoimmunity. Immunol Res. 65(1):82-98.