Information Links
Related Conferences
Previous Issues Volume 5, Issue 1 - 2020
Appropriateness of Indications of Caesarean Sections in a District Setting of Cameroon
Ascensius A. Mforteh1*, Sama Dohbit2, Collince Tchakounte3, Bernard Nsah4, Pascal Foumane2, Robinson E. Mbu2
1Regional hospital of Bamenda, Cameroon 2Department of Obstetrics and Gynecology, University of Yaoundé 1, Yaoundé, Cameroon 3Hopital saint Jean de Malte, Njombe, Cameroon 4Kumbo West District Health Service, Cameroon
*Corresponding author: Ascensius Achuo Mforteh, Regional hospital of Bamenda, Cameroon, E-mail: [email protected]
Received Date: July 08, 2020 Published Date: August 31, 2020 Copyright: Mforteh AA, et al. ©2020 Citation: Mforteh AA. (2020). Appropriateness of Indications of Caesarean Sections in a District Setting of Cameroon. Mathews J Gynecol Obstet. (5)1: 18.
ABSTRACT Introduction: Compared to vaginal birth, caesarean delivery without medical indication has higher odds for severe adverse maternal outcomes during antepartum and intrapartum. The aim of this study was to determine the appropriateness of indications of caesarean section (CS) in a rural district hospital. Methodology: Across sectional analytical study of cases of CS from the 1st of January 2018 to the 31st of December 2018 at the district hospital of Njombe-Penja Health district. The appropriateness of each CS indication was evaluated by two independent obstetricians; a third opinion was sought in case of a tie. Results: The CS rate was 26.2%. The most common indications in decreasing order were: previous scar, dystocia and foetal distress. Overall proportion of inappropriately indicated cases was 12.7%; GPs had the highest rate (25.4%) with a 12 fold increased risk of an inappropriate indication. Referred patients were more likely to have an appropriate indication (OR: 2.92, CI: 0,984–8,561, p value: 0,045). There was no difference in the proportion of inappropriately indicated CS between emergencies and elective CS (OR: 1,098 CI: 0,469–2,572; p Value: 0,829). Nulliparity was significantly associated with a 3.5 increased risk for inappropriate indication. Dystocia and abnormal pelvis recorded the highest proportion of inappropriately indicated CS. Scarred uterus was seven times more likely to have an appropriate indication. Conclusion: The most common indications for caesarean section in our study were previous scar, dystocia and foetal distress. The CS rate obtained was 26.2% which could be partly explained by increased number of referrals and a high rate of repeat caesarean sections. If we must reduce the CS rate, CS indications for dystocia or in nulliparous women have to be double checked to avoid inappropriate indicated CS which are common in these groups, and General practitioners have to be continuously recycled on indications of CS.
Keywords: Caesarean Section, Indications, Appropriateness, District
INTRODUCTION According to Betran AP, et al. [1], there have been a global progressive increase over the last decades in the rate of deliveries by caesarean section (CS) although the reasons for such a trend are not completely understood. Based on data from 121 countries, the trend analysis showed between 1990 and 2014, the global average CS rate increased from 6.7% to 19.1%. Several studies done in some resource limited countries such as Nigeria, Ethiopia, and Uganda [2-5], showed CS rates that vary from 11.3 to 35.5% which are generally above the WHO recommended range. According to the Cameroon Demographic and Health Survey of 2011 [6], the CS rate was estimated at 3.8% although individual health facilities have shown increasing trends in CS rates. For example, considering two hospitals in Yaounde [7-9], the CS rate at the Central Hospital of Yaounde was 18.64% in 2012 and 29.3% in 2018 and that of the Yaounde Gynaeco-Obstetric Hospital was 19.7% in 2012 and 34.2% in 2018. As shown by Souza JP, et al. [10], caesarean delivery without medical indication has higher odds for severe maternal adverse outcomes when compared to vaginal delivery during antepartum (OR: 5.93; 95% CI 3.88-9.05) and intrapartum (OR: 14.29 95% CI: 10.91-18.72). In a Ugandan study [11], only 46% of the indications of caesarean sections were considered to be appropriate. In another study in Tanzania [12], up to 30.1% of CS indications were judged to be substandard indications thus leaving a high proportion of inappropriately indicated CS which increases maternal and neonatal morbidity and mortality. Kamgang MM [9], working on the pertinence of indications of elective CS in three reference hospitals in Yaounde-Cameroon, found that of the 158 cases, 48.7% (77 cases) had pertinent indications, 45.6% had non pertinent indications but which could be justified and 5.7% (9 cases) had non pertinent indications which could not be justified. The appropriateness of CS has not been evaluated in a district level. The aim of this study was thus to evaluate the appropriateness of caesarean section indications in a district hospital of Cameroon.
METHODOLOGY We carried out a cross sectional analytical study from January 1st, 2018 to December 31st, 2018 at the Hospital Saint Jean de Malt of Njombe which serves as the District hospital of the Njombe-Penja Health District of the Littoral region of Cameroon. The study site was chosen for convenience because medical records and theatre registers are available. The maternity is headed by an obstetrician and has a general practitioner posted in the service. Other general practitioners take turns at the maternity during call duty. Senior residents in obstetrics sometimes do their postings at this hospital. Women in labour are received by an attending midwife and an assessment is done by the resident or general practitioner on call. If need be, the obstetrician’s opinion is sought. The women in labour are monitored and followed up using partograms and a cardiotograph. There is no CT scan machine for pelvimetry. All cases of caesarean sections carried out during the study period were included and cases with incomplete medical records were excluded. However, the excluded cases were taken into consideration in the calculation of the prevalence of caesarean sections. The sample size was calculated using the Lorenz formula n = z2pq/e2 Where Z = 1.96, e = 0.05, p = 22% representing a previous CS rate at the district hospital and q = 1-p. Data were collected from patients’ medical files on a daily basis using pretested form. A photocopy of each partogram was made for subsequent use during determination of appropriateness of the various indications. Codes were used to replace names to ensure anonymity. Data collected included; age, parity, gestational age, number of previous caesarean section, referral status, indication for caesarean section and elements for the indication of the CS. Cases were classified into two groups by two independent Obstetricians based on whether the indication was appropriately indicated and non-appropriately indicated. Where there was a discrepancy, a third opinion was sought and the case discussed by all three Obstetrician to have a single answer. Diagnostic criteria for the various indications were considered as follows; Foetal distress was considered appropriate if one of the elements of category III of the Tiered system recommended by ACOG [13], was present. Dystocia (Failure to progress and CPD) was diagnosed using the recommendations from the obstetric care onsensus No.1 on Safe prevention of the primary cesarean delivery by ACOG [14], which recommended that protraction or arrest should not be diagnosed before 6cm dilatation and that active labour arrest should only be considered after 4 hours of adequate contractions or 6hours of inadequate contractions despite oxytocin infusion. Using the ACOG recommendations [14], arrest of labour in second stage was diagnosed only after two hours of pushing in multiparous women or 3 hours of pushing in nulliparous women so long as maternal and foetal parameters permitted. Foetal parameters that could permit an immediate decision for CS were an increasing caput succedaneum or abnormal foetal heart tracings. Maternal parameters included, cervical and or vulva oedema, haematuria or reduced or loss of function of lower limbs while waiting to exhaust the recommended time frames. Conditions associated with a previous scar that were acceptable as appropriate for indicating a CS included; big or macrosomic babies, breech, twin gestation, multiple scar, unknown scar and a clinical pelvimetry with obstetric conjugate less than 10.5cm. Fetal macrosomia was assumed appropriate for estimated foetal weights of over 4000g. Clinical estimation using Symphysio-fundal height (Kongnyuy and Mbu’s formula) and or ultrasound estimated foetal weights at term were acceptable. Breech in nulliparous women or with suspected macrosomia, transverse lies, and face presentations with occiput anterior were accepted as appropriate. Placenta praevia was considered appropriately indicated in the case of active bleeding with threat to maternal life in emergency. In an elective context, it was accepted as appropriate if there was a notion of per vaginal bleeding with confirmation of placenta praevia by ultrasound. Placenta abruption was accepted in presence of per vaginal bleeding with viable foetus with notion of trauma or ultrasound findings or signs of uterine muscle infiltration (Board like rigidity of the uterus). Twin gestation was considered appropriate if first twin was in breech. Preeclampsia was accepted if there were signs of severity with a very poor Bishop score. Pelvic fracture or congenital deformity was considered as appropriate indications. Abnormal clinical pelvimetry with obstetrical conjugate less than 10.5cm in healthy pregnant women without a trial of labour was not considered as appropriate. Data was analysed using SPSS version 23 software by calculating proportions and frequencies and use of Chi-square test to compare proportions between the two groups. A p - value of less than 0.05 was taken as statistically significant. Ethical clearance was obtained from the ethical committee of the hospital all participants signed a consent form. RESULTS A total number of 273 cases of caesarean sections were recruited for a total of 1,042 deliveries (caesarean rate: 26.2). Of the 273 cases, 267 cases were retained for analysis. The mean age was 28.2 ± 6.1 years with a range of 15 to 45. There were 94 (35.2%) nulliparous women. There were 72 (27%) women with a previous scar of which 48 (18% of total participants) had a single scar, 19 (7.1% of total population) had a double scar and 5 (1.9% of total population) had a tripplescar. There were 70 (26.2%) cases of referals from different health facilities. 78% of cases were done in emergency. A greater majority of the study population were at term (82%) while 11.6% were preterm and 6.4% were post-term. Caesarean sections were indicated in 44.2% of cases by GPs, in 34.5% of cases by Residents and in 21.3% of cases by an Obstetrician. Previous scar, Dystocia (Cephalopelvic disproportion and failure to progress) and acute fetal distress were the main indications for caesarean sections as shown in figure 1. Over all, 34 (12.7%) cases out of the 267 cases were inappropriately indicated. The distribution of the appropriateness of CS indications with respect to various variables is shown in table II. The risk of an inappropriate indication was 12 times higher when the indication was made by a General practitioner (1/0.081). Nulliparous women were 3.5 times more likely to have an inappropriate indication. Referred patient were about three times higher to get an appropriate diagnosis than non-referred patients. There was no significant difference in the number of inappropriately indicated caesarean sections between the group of emergency and that of elective caesarean sections. Dystocia (CPD and failure to progress) and abnormal clinical pelvimetry recorded the highest amounts of inappropriately indicated caesarean sections. Unlike CPD, Abnormal clinical pelvimetry was associated with a highly significant risk of inappropriate caesarean section indications. Scarred uterus on the contrary was seven times more likely to have an appropriate indication.
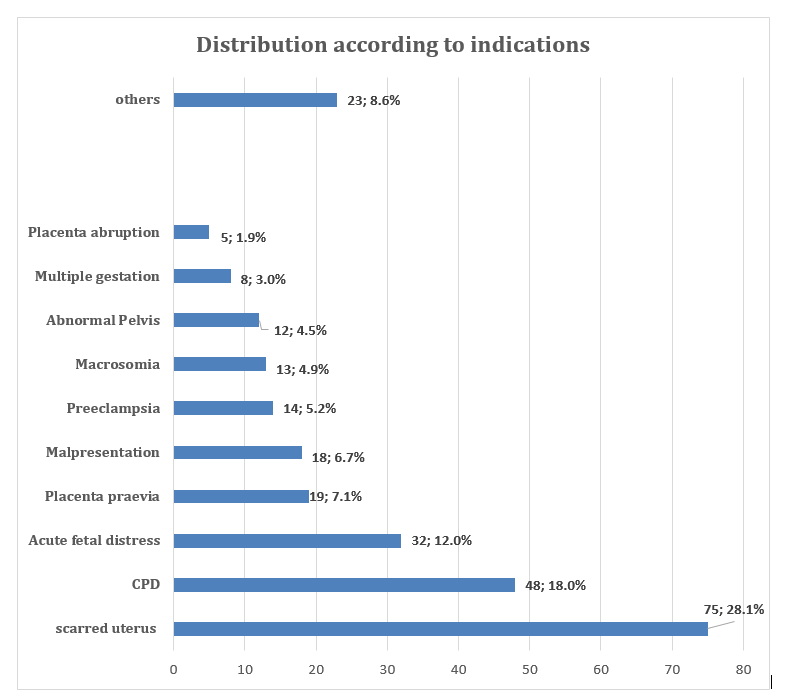 Figure 1: Distribution of Caesarean sections according to indications.
Figure 1: Distribution of Caesarean sections according to indications.
|
Indication |
Frequency |
Percentage (%) |
|
Failed induction |
4 |
17.4 |
|
Genital tract infection (Active herpes, vulvo-vaginal condylomata) |
4 |
17.4 |
|
Cordprolapse |
3 |
13.0 |
|
Genital tract obstruction (myomapraevia, vaginal septum) |
3 |
13.0 |
|
IUGR |
2 |
8.7 |
|
Fetal malformation |
2 |
8.7 |
|
Premature rupture of membranes |
2 |
8.7 |
|
Precious baby |
2 |
8.7 |
|
Non descent |
1 |
4.3 |
Table 1: Other indications of caesarean.
|
|
|
Appropriate n (%) |
Non Appropriate n (%) |
Total n (%) |
Odds Ratio |
CI 95% |
P Value |
|
Person who made indication |
Obstetrician |
55 (96,5) |
2 (3,5) |
57 (100) |
4,844 |
1,944 – 21,292 |
0,018 |
|
Resident |
90 (97,8) |
2 (2,2) |
92 (100) |
10,070 |
2,356 – 43,045 |
< 0,001 |
|
|
Gen. Pract. |
88 (74,6) |
30 (25,4) |
118 (100) |
0,081 |
0,028 –0,854 |
< 0,001 |
|
|
|
|||||||
|
Parity |
Nulliaprous |
73 (77,7) |
21 (22,3) |
94 (100) |
0,282 |
0,134 - 0,595 |
0,001 |
|
Primiparous |
50 (87,7) |
7 (12,3) |
57 (100) |
1,054 |
0,434 - 2,562 |
0,908 |
|
|
multiparous |
110 (94,8) |
6 (5,2) |
116 (100) |
4,173 |
1,666 - 10,456 |
0,001 |
|
|
|
|||||||
|
Referral status |
Referred |
65 (94,2) |
4 (5,8) |
69 (100,0) |
2.92 |
0,984 – 8,561 |
0,045 |
|
Non referred |
168 (84,8) |
30 (15,8) |
198(100,0) |
||||
|
|
|||||||
|
Degree of urgency |
Emergency |
182 (87,5) |
26 (12,5) |
208 (100,0) |
1,098 |
0,469 – 2,572 |
0,829 |
|
Elective |
51 (86,4) |
8 (13,6) |
59 (100,0) |
||||
|
|
|
|
|
|
|
|
|
Table II: Appropriateness of CS indications with respect to various variables.
|
|
Appropriate n (%) |
Inappropriate n (%) |
Total n (%) |
Odds Ratio |
CI 95% |
p - Value |
|
Scarred uterus |
73 (97,3) |
2 (2,7) |
75 (100,0) |
7,300 |
1,704 – 31,281 |
0,001 |
|
Dystocia |
38 (79,2) |
10 (20,8) |
48 (100,0) |
0,468 |
0,207 – 1,057 |
0,063 |
|
Malpresentation |
17 (94,4) |
1 (5,6) |
18 (100,0) |
2,597 |
0,334 – 20,171 |
0,485 |
|
Acute foetal distress
|
29 (90,6) |
3 (9,4) |
32 (100,0) |
1,469 |
0,422 – 5,113 |
0,778 |
|
Placenta previa |
19 (100,0) |
0 (0,0) |
19 (100,0) |
NA |
NA |
0,145 |
|
Placenta abruptio
|
5 (100,0) |
0 (0,0) |
5 (100,0) |
NA |
NA |
1,000 |
|
Preeclampsia |
13 (92,9) |
1 (7,1) |
14 (100,0) |
1,950 |
0,247 – 15,401 |
1,000 |
|
Abnormal clinical pelvimetry |
1 (8,3) |
11 (91,7) |
12 (100,0) |
0,009 |
0,001 – 0,073 |
< 0,001 |
|
Macrosomia |
13 (100,0) |
0 (0,0) |
13 (100,0) |
NA |
NA |
0,384 |
|
Multiple gestation
|
6 (75,0) |
2 (25,0) |
8 (100,0) |
0,423 |
0,082 – 2,186 |
0,270 |
|
Others |
19 (82,6) |
4 (17,4) |
23 (100,0) |
0,666 |
0,212 – 2,90 |
0,333 |
Table III: Distribution of appropriateness of CS indications with respect to indication of surgery.
|
Indication |
Reason why indication not appropriate |
|
Abnormal pelvis |
|
|
Dystocia |
|
|
Breech |
|
|
Acute fetal distress |
|
|
Pre-eclampsia |
|
|
Multiple gestation |
|
|
Failed induction |
|
|
Premature rupture of membranes |
|
Table IV: Reasons why some indications were considered in appropriate.
DISCUSSION The caesarean section rate in our study was 26.2% which is higher than the WHO [15] recommended rate of 5-15%. This finding is similar to that of other studies done in other parts of Africa and in Cameroon [3,9], for which the authors proposed that the high rate of CS could be explained by high rates of referred cases received. In addition to the high amount of referred cases (26.0% in our study we observed a high rate of repeat CS (27.0% in our study). The high proportions of referred patients and repeat CS could partly explain the high rate of CS rate in our study population. The most common indication of CS was a previous scar (28.1%) (Figure 1). Our finding is similar to that of Mdegela HM, et al. [12] who reported a 30.2% rate for repeat CS. Our finding is however not consistent with that of other studies [11,16,17] in which dystocia (CPD and failure to progress) was the most common indication. The high proportion of CS due to previous scar could be explained by the fact that there is a wide range of locally acceptable conditions which when associated with a previous scar gives an appropriate indication. These conditions include amongst others big or macrosomic babies, twin gestation, breech, unknown location of previous scar etc. However, the best possible way of reducing CS due to previous scar would be to avoid an evitable scar in the first place. Other common indications in our study included; Dystocia ( CPD and failure to progress) and Acute foetal distress which are amongst the most common indications in other studies [11,16]. Overall, 34 out of the 267 (12.7%) cases were judged inappropriate. In the study in Tanzania [11], about one third (30.1%) of the study population had substandard decisions for CS. In another study in Uganda [12], only 46% of the cases of CS were judged to have appropriate indications. The low rate of inappropriately indicated caesarean sections could be explained by the fact that more than half of the indications of caesarean sections were made by an obstetrician or by senior residents in Obstetrics. The proportion of inappropriately indicated CS by General practitioner was obtained at 25.4%. This proportion is similar to the 30.1% obtained in Tanzania by Mdegela and collaborators. Another study in rural Tanzania [18]found a proportion of 26% for substandard CS indications. The high rate of inappropriately indicated CS implies an increase economic burden which could even be felt more in a low resource country like Cameroon. Jonathan[11]proposed that the high number of unnecessary caesareans appear to be related to lack of knowledge and inexperience of staff and despite attempts to address the situation through teaching, the scope of the problem seems too large that it needs a fundamental change in the healthcare system in terms of resources, education, continuing professional development and clinical governance. To Mdegela HM, et al. [12], there is a need to improve quality of assessment and decision before performing a CS. The high rate of inappropriately indicated CS for general practitioner perhaps would have been lowered safely if regular auditing and feedback could be implemented. As such a majority of the 25.4% of inappropriately indicated CS of general practitioner should have been prevented if appropriate audit measures were in place since elsewhere [19], the effectiveness of such methods in reducing substandard CS decisions have been demonstrated. Nulliparous women in the current study were found to have more inappropriately indications for CS (21 out of 34; 87.5%) compared to their primiparous and multiparous counterparts with 20.6% and 17.6% respectively. With over one third (94 out of 267; 35.2%)of all CS done on nulliparous women and the fact that most of the inappropriately indicated CS was in this group, there is perhaps a reason to explain the rising trends in CS rates especially as in our current study, the most common indication was previous scar. This finding further underscores the importance of preventing unnecessary primary CS as a cornerstone in reversing the present and future rates of CS shown in previous studies [19, 20]. Amongst the ten most common indications of CS, Dystocia and abnormal bony pelvis had the highest proportion of inappropriately indicated CS. This is contrary to results of some studies [12,21] in which foetal distress was the most inappropriately diagnosed. In one of such studies [21], foetal distress accounted for 84% of the total misdiagnosed cases. In our study, a more objective method of cardiotography was used and meconium stained amniotic fluid without fetal cardiac anomalies was not considered as fetal distress which was the case in the other studies. As seen in table III, abnormal clinical pelvimetry had the highest proportion of inappropriate indications with a significant difference between appropriately indicted and inappropriately indicated CS. The majority of such inappropriate indications were indicated for clinical borderline pelvis. Following the WHO recommendations on clinical pelvimetry on admission [22], routine clinical pelvimetry on admission in labour is not recommended for healthy pregnant women as there is currently no evidence that this practice improves outcome. In fact, routine clinical pelvimetry would increase the number of caesarean sections without any benefits. The benefits of clinical pelvimetry have been highlighted by findings of some observational studies [23,24] and are limited to help predict CPD among nulliparous women in some low-resource settings with limited access to CS and a need for timely referral to a higher-level facility. Scarred uterus appeared to be significantly associated with an appropriate indication with a 7-fold chance of an appropriate indication as shown on table III. As previously discussed, this could be due to the wide range of locally acceptable conditions which when associated with a previous scar are acceptable indications for a CS thus allowing more women to have anelective caesarean delivery than a trial of labour after caesarean. Randomized control trials are therefore needed in this context to ascertain local factors leading to successful vaginal birth after CS in order to reduce the high proportion of repeat CS. CONCLUSION The most common indications for caesarean section in our study were previous scar, dystocia and fetal distress. The CS rate obtained was 26.2% which could be partly explained by increased number of referrals and a high rate of repeat caesarean sections. If we must reduce the CS rate, CS indications for dystocia or in nulliparous women have to be double checked to avoid inappropriate indicated CS which are common in these groups, and General practitioners have to be continuously recycled on indications of CS. CONSENT Written informed consent was obtained from all participants. CONFLICTS OF INTEREST The authors declare that they have no conflicts of interest. AUTHORS’ CONTRIBUTIONS Ascensius Achuo Mforteh and Bernard Nsahproposed the topic. Ascensius Achuo Mforteh and Collince Tchakounte collected data. Ascensius Achuo Mforteh wrote the initial draft. Sama Dohbit, Pascal Foumane and Robinson Enow Mbu revised the draft. All authors read and approved the final manuscript. ACKNOWLEDGMENTS The authors want to thank the entire staff of the Hopital Saint Jean de Malte, Njombe, especially the Director of the Hospital, the maternity and the theatre staff. The authors also want to thank all the participants of this study for accepting to take part. REFERENCES 1. Betran AP, Ye J, Moller AB, Zhang J, Gulmezoglu AM, et al. (2016). The increasing trend in caesarean section rates: Global, regional and national estimates: 1990-2014. PLoS ONE. 11(2):e0148343. 2. Adekanle DA, Adeyemi AS, Fasanu AO. (2003). Caesarean section at a tertiary institution in South-western Nigeria-A 6-year audit. Open J of Obstetrics and Gynecology. 03:351-61. 3. Abebe FE, Gebeyehu AW, Kidane AN, Eyassu GA. (2016) Factors leading to cesarean section delivery at Felegehiwo treferral hospital, Northwest Ethiopia: a retrospective record review. Reproductive Health. 13:6. 4. Nelson JP. (2016). Can the presence of an additional senior doctor reduce the caesarean rate at a regional referral hospital in western Uganda? Poster session presented at: The 18th Annual British Maternal and Fetal Medicine Society Conference. Birmingham. 21-22. 5. Onoh RC, Eze JN, Ezeonu PO, Lawani LO, Iyoke CA, et al. (2015). A 10-year appraisal of cesarean delivery and the associated fetal and maternal outcomes at a teaching hospital in southeast Nigeria. International Journal of Women’s Health. 7:531-8. 6. Institute National de la statistique. Enquete Demographique et de Sante et a Indicateurs Multiples du Cameroun. 2011. [Available at www.statistics-cameroun.org]. 7. Foumane P, Mve K, Ze MJ, Njofang N, Dohbit JS, et al. (2014). Facteurs de risque et pronostic des cesareannes d'urgence a l'hopital gyneco-obstetrique et pediatrique de Yaounde (Cameroun). Med Sante Trop. 24(1):89-93. 8. Kemfang JD, Ngassam A, Fouogue JT, Metogo J, Medou A, et al. (2015). Complications maternelle precoces de la cesarienne: a propos de 460 cas dans deux hopitaux universitaires de Yaounde, Cameroun. Pan Afr Med J. 21(265):67-9. 9. Kamgang MM. (2018). Analyse de la pertinence des indications de cesarienne programmee a terme dans trois hopitaux de reference de Yaounde: Universite de Montagnes, Bagangte-Cameroun. Unpublished Thesis. 10. Souza JP, Gulmezoglu A, Lumbiganon P, Laopaiboon M, Carroli G, et al. (2010). Caesarean section without medical indications is associated with an increased risk of adverse shortterm maternal outcomes: the 2004-2008 WHO Global Survey on Maternal and Perinatal Health. BMC Med. 8:71. 11. Jonathan PN. (2017). Indications and appropriateness of caesarean sections performed in a tertiary referral centre in Uganda: a retrospective descriptive study. Pan African Medical Journal. 26:24. available online at http://www.panafrican-med-journal.com/content/article/6/64/. 12. Mdegela HM, Muganyizi SP, Pembe BA, Simba OD, Roosmalen VJ. (2012). How rational are indications for emergency caesarean section in a tertiary hospital in Tanzania? Tanzania Journal of Health Research. 14(4):6. Doi: http://dx.doi.org/10.4314/thrb.v14i4.1. 13. Management of intrapartum fetal heart rate tracings. (2010). American College of Obstetricians and Gynecologists Practice Bulletin No. 116. Obstet Gynecol. 116:1232-40. 14. American College of Obstetricians and Gynecologists. (2014). Safe prevention of the primary cesarean delivery. Obstetric care onsensus No. 1. Obstet Gynecol. 123:693-711. 15. Betran AP, Torloni MR, Zhang JJ, Gülmezoglu AM. (2016). For the WHO Working Group on Caesarean Section. WHO Statement on Caesarean Section Rates. BJOG. 2016;123(5):667-70. 16. Tita Alan TN. (2012). When Is Primary Cesarean Appropriate: Maternal and Obstetrical Indications. Semin Perinatol. 36:324-327. 17. Al-Mulhim A, Abu-Heija TA, Ali HA, Bahnasty A. (2001). Factors affecting the rate and indications of primary caesarean. Bahrain Medical Bulletin. 23(4):160-2. 18. Maaloe N, Bygbjerg IC, Onesmo R, Secher NJ, Sorensen BL. (2012). Disclosing doubtful indications for emergency caesarean section in rural hospitals in Tanzania: a retrospective criterion- based audit. Acta Obs Gynecol Scandinavica. 91:1069-76. 19. Scarella A, Chamy V, Sepulveda M, Belizan JM. (2011). Medical audit using the Ten Group Classification System and its impact on the cesarean section rate. Eur J Obstet Gynecol Reprod Biol. 154:136-40. 20. Gibbons L, Belizan JM, Lauer JA, Betran AP, Merialdi M, Althabe F. (2012). Inequities in the use of cesarean section deliveries in the world. Am J Obstet Gynecol. 206:e331-19 21. Maaloe N, Sorensen BL, Onesmo R, Secher NJ, Bygbjerg IC. (2012). Prolonged labour as an indication for emergency caesarean section: a quality assurance analysis by criterion based audit at two Tanzania rural hospitals. British Journal of Obstetrics & Gynecology. 119:605-13. 22. WHO Reproductive Health Library. (2018). WHO recommendations on clinical pelvimetry on admission. The WHO Reproductive Health Library; Geneva: World Health Organisation. 23. Rozenholc AT, Ako SN, Leke RJ, Boulvain M. (2007). The diagnostic accuracy of external pelvimetry and maternal height to predict dystocia in nulliparous women: a study in Cameroon. BJOG. 114:630-5. 24. Liselele HB, Boulvain M, Tshibangu KC, Meuris S. (2000). Maternal height and external pelvimetry to predict cephalopelvic disproportion in nulliparous African women: a cohort study. BJOG. 107:947-52.