Information Links
Related Conferences
Previous Issues Volume 9, Issue 2 - 2025
An Observational Study Related to Health Related Quality of Life in Women Suffering from PCOS
Jalak Shaileshbhai Gajera, Megha Harshadbhai Patel*, Nensi Pravinbhai Patel, Nahid MO Shakil Saiyed
Doctor of Pharmacy, Gujarat Technological University, Gujarat, India
*Corresponding author: Miss. Megha Patel, Doctor of Pharmacy, Gujarat Technological University, Surdas Chowk, Bochasan, Near Bank of India, Ta: Borsad, Dist: Anand, Gujarat, India, Phone: 9327366588, E-mail: [email protected]
Received Date: March 18, 2025
Published Date: May 13, 2025
Citation: Gajera JS, et al. (2025). An Observational Study Related to Health Related Quality of Life in Women Suffering from PCOS. Mathews J Gynecol Obstet. 9(2):46.
Copyrights: Gajera JS, et al. © (2025).
ABSTRACT
Aim: An observational study related to heath related quality of life in women suffering from PCOS. Objectives: To assess Quality of Life & the impact of symptoms in women Suffering from PCOS. Methodology: This study was initiated after getting the approval from college research committee & Institute Ethics Committee. All patients age between 18-45 years old with PCOS attending to the OPD of our study site, during the study period of 4 months will be including in the study after taking information consent. All the demographic and clinical detail of the patient will be filled in a predesign case report form. To assess quality of life and to assess psychological burden “PCOSQoL 45-57 was used and score of above mention scale is calculated and recorded. Result and Discussion: In our study, we had evaluated each question result from the scale. Each question has the multiple options such as Agree, Highly Agree, Disagree and we had calculated the number of patients and number of percentage form each options of individual question. In overall 6 factors the more agree responses were found in hair and acne disorder (21%) whereas, less number of responses were found in body images (11%) & the highly agree responses were found in Physiological and emotional status (21%) whereas, less number of responses were found in body images (9%) & the more disagree responses were found in obesity and menstrual disorder and (23%) whereas, less number of responses were found in body images (8%). Conclusion: We studied the Quality of Life of PCOS patients. Investigation of the scale of PCOSQoL 45-57 showed that PCOS had impact on their emotions self-embarrassment, self-esteem, feelings of sadness, self-confidences, overall emotional stability. In our study we collect the data of 127 participants in which 102 females were married & 25 females were unmarried, from these we concluded that PCOS is more affected in married females & lesser affected in unmarried females. As per our study we include 6 factors such as, Physiological & Emotional status, Menstrual Irregularities and Infertility, Body Images, Hair Disorder and Acne, Fertility and Sexual life, Obesity and Menstrual Disorder and we found that Hair disorder and Acne is more affecting factor in PCOS Women & in contrast Body image is lesser affecting factor in PCOS women, we concluded it from PCOSQoL 45- 57 Scale.
INTRODUCTION
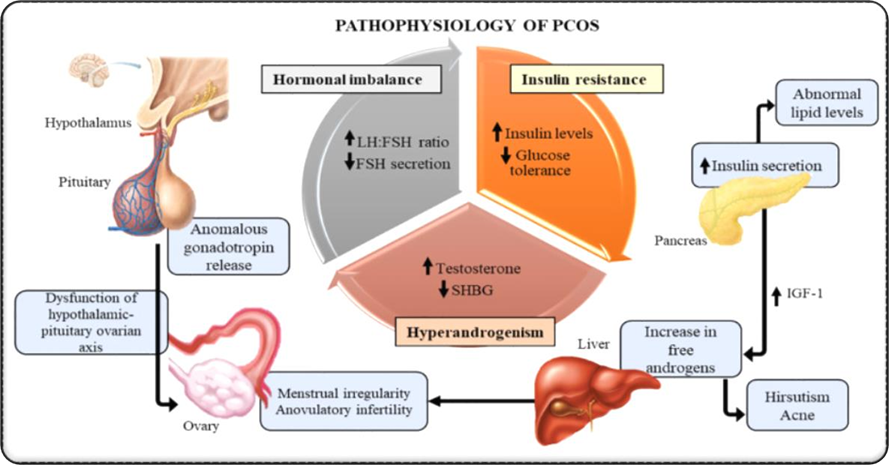
Polycystic ovary syndrome (PCOS) is a Heterogeneous disorder, as PCOS is a hormonal imbalance brought on by an excess of hormones produced by the ovaries, the organ that produces and releases eggs. Ovaries release androgen hormones in abnormally high amounts if you have PCOS [1].
.png)
Figure 1. PCOS [2].
In PCOS reproductive hormones will be imbalance as a result. Consequently, irregular menstrual cycles, Irregular menstruation, and uncertain ovulation are common in PCOS patients. Due to anovulation, or absence of ovulation, small follicular cysts—fluid-filled sacs containing immature eggs may be seen in the ovaries on ultrasonography. One of the most frequent reasons for infertility in women and those who were Assigned Female at Birth (AFAB) is PCOS. Additionally, it may make you more susceptible to other illnesses [1].
The possible effects of PCOS on the quality of life of affected women. In general, health- related quality of life (HRQoL) is a measurement of the portion of an individual's happiness that is influenced by their health, and it is estimated through the use of specially created questionnaires. The impact of PCOS on HRQoL has only been directly measured in one study to date. Still, a number of research have provided a qualitative description of the impact of PCOS, and other studies are intended to look into the impacts of various PCOS symptoms individually on HRQoL.
According to specialized society recommendations, PCOS must be diagnosed based on the presence of two out of the three criteria listed below: polycystic ovaries, clinical or biological hyperandrogenism, and chronic anovulation. Since it's an exclusion diagnosis, conditions that resemble PCOS's clinical characteristics must be ruled out. These include non-classical congenital adrenal hyperplasia, hyperprolactinemia, and thyroid disease.
Sign and Symptoms
Some women start developed symptoms around the time of first period. Others only discover they have PCOS after they’ve gained a lot of weight or they’ve had trouble Conceive pregnant.
Among the most typical signs of PCOS are:
Abnormal Uterine Bleeding (Irregular periods)
Missing periods or having no periods at all are examples of abnormal Amenstruation. It might also result in Menorrhagia. The regular eliminating of the uterine lining is complicated by non-ovulation. Less than eight periods or none at all are experienced by some PCOS-affected women [1,3].
.png)
Figure 2. Abnormal uterine bleeding [4].
Hirsutism (Abnormal hair growth)
A medical condition linked to the hormones known as androgens is hirsutism. The most prevalent cause of hirsutism is polycystic ovarian syndrome (PCOS), which affects up to 10% of women and is characterized by the ovaries producing excessive levels of androgens [1,3].
.png)
Figure 3. Hirsutism [7].
Acne
PCOS and other hormonal conditions that can lead too much testosterone in the body & can increase sebum and skin cell production, leading to acne. Particularly on the back, chest, and face, acne can be caused due to PCOS. Acne can persist well into adolescence and can be challenging to cure [1,3].
.png)
Figure 4. Acne [6].
Obesity
Between 40 and 80 percent of PCOS patients are obese and struggle to maintain a healthy weight. Insulin resistance may develop as a result of the body's cells being less sensitive to insulin in PCOS. In order to make up for this, the pancreas produces more insulin. Because elevated insulin promotes fat accumulation, increases appetite, and inhibits the breakdown of stored fat, it can all lead to weight gain [1,3].
.png)
Figure 5. Obesity [7].
Acanthosis nigricans (Darkening of the skin):
PCOS may develop dark spots on your skin, particularly in the groin, armpits, and neck folds [1,3].
.png)
Figure 6. Acanthosis nigricans [8].
Menorrhagia (Heavy bleeding): If you do experience periods, they may be thicker than usual since the uterine lining thickens over an extended period of time [1,3].

Alopecia: Scalp hair thins and may eventually fall out [1,3].
Headaches: PCOS increases the chance of depression and obesity, two conditions that increase the risk of migraine headaches [1,3].

Etiology:
The exact cause of PCOS is unknown, but some possible contributing factors are as follows
Insulin resistance
Low-grade inflammation Heredity
Excess androgen
Epidemiology:
As previously stated, depending on the diagnostic criteria, PCOS affects 5% to 15% of girls in the reproductive age range around the world, making it the most prevalent 98(%) endocrine disorders. Relative to the 1990 National Institute of Health standards, the Rotterdam standards include a wider range of prevalence. It is estimated that around 5 million females in the United States who are of reproductive age suffer with PCOS, according to the NIH 2012 workshop report. The cost to the healthcare system for identifying and treating PCOS is roughly $4 billion yearly, not considering the expense of major comorbidities associated with PCOS [9].
Numerous conditions have been linked to PCOS, such as infertility, metabolic syndrome, obesity, impaired glucose tolerance, diabetes mellitus (DM-2), cardiovascular risk, depression, OSA, endometrial cancer, and NAFLD/NASH. Additionally, there is evidence of a higher prevalence in first-degree relatives with PCOS, prepubertal obesity, congenital virilizing disorders, above-average or low birth weight for gestational age, premature adrenarche, and use of valproic acid as an antiepileptic medication.
Pathophysiology
Diagnosis
The accurate diagnosis of polycystic ovarian syndrome (PCOS) lacks a single test. Physician will probably observe about symptoms, prescription drugs, and any other illnesses that women have. Physician might also inquire about any changes in weight and menstrual cycles. During a physical examination, symptoms of acne, insulin resistance, and excessive hair growth are observed.
Pelvic Examination: Physician might examine reproductive organs during a pelvic examination for detection lumps, growths, or other abnormalities.
Blood Tests: Hormone levels can be measured by blood testing. With this testing, any causes of irregular periods or androgen excess that resemble PCOS may be ruled out. Additional blood tests, such fasting cholesterol and triglyceride measurements, may be performed on patient. Body's reaction to sugar (glucose) may be measured using a glucose tolerance test.
Ultrasound: ovaries may appear and the thickness of uterine lining may both be examined using an ultrasound. Vagina route is used to insert a transducer, which resembles a wand Sound waves are emitted by the transducer and are converted into visuals on a computer screen & PCOS is diagnosed. physician may suggest further testing to look for issues.
Treatment
Lifestyle Modification
Exercise and calorie-restrictive diets are the most effective first-line therapies for weight reduction and IGT in overweight and obese PCOS women and adolescents. Numerous studies have demonstrated that hirsutism can enhance ovulation and menstrual cycle management. In an attempt to better address hyperinsulinism, low-carb diets have been employed; however, research has not revealed any differences in the results obtained from these diets.
Hormonal Contraceptive
Hormonal contraceptives, such as oral, patch, or vaginal rings, are the first line of therapy for irregular menstruation, hirsutism, and acne. The Endocrine Society is not biased toward any one option. By lowering LH levels, the progestin component increases sex hormone-binding globulin and indirectly reduces the generation of androgen in the ovaries [9].
Furthermore, it has been demonstrated that certain progestins directly block 5 alpha- reductase activity, preventing free testosterone from being converted to 5 alpha- dihydrotestosterone, which is a more powerful form. These progestins have been proven to have direct antiandrogenic characteristics. They are therefore quite successful in reducing hyperandrogenism symptoms and regulating the menstrual cycle.
Every patient should have their hormonal contraceptive contraindication screened. Absolute contraindications include women 35 years of age or older who smoke more than 15 cigarettes a day, have uncontrolled hypertension higher than 160/100, uncontrolled diabetes, and severe peripheral vascular disease. When there are several comorbidities, the US Medical Eligibility Criteria for Contraceptive Use are a useful resource [9].
Hormonal contraceptives are not contraindicated for patients with diabetes who do not have vascular problems.
In terms of how hormonal contraceptives affect metabolism, increased estrogen activity raises HDL cholesterol and lowers LDL cholesterol. No difference in body weight or distribution of fat between women with PCOS and those without.
Initial oral contraceptive dosage of 20 mcg of ethinyl estradiol in combination with a progestin that either has neutral effects, like norehindrone acetate, or antiandrogenic qualities, such desogestrel and drospirenone. It has been demonstrated that progestins with antiandrogenic qualities increase the incidence of venous thromboembolism (VTE). If this initial dose of ethinyl estradiol does not entirely manage hyperandrogenic symptoms, it is possible to raise the dosage to 30 to 35 mcg.
METHODOLOGY
Study Site
This study was conducted at Akanksha Hospital & Research Institute Anand.
Source of Data
Patient demographics, present complaints, past history, medical history, medication history, family history, PCOSQOL 45-57 form was filled through patient counseling who visited the OPD of our study site.
Related Approval:
All the clinical data of patient between 18-45 years of age and clinically diagnosed with PCOS.
Duration of Study
The study was conducted for the duration of 6 months after getting ethical approval from the Institutional Ethics Committee Charusat.
Study Design
Observational Study.
NO. OF SAMPLES COLLECTED: 127 approx
By using solvin formula:
n = N/1+N (e2)
n = Minimal number of sample size
N = Total number of population
E = Margin of error (assume to be worth 8%)
n = 1000/1+1000 (0.08)2
n = 1000/1+6.4
n = 1000/7.4
n= 135
Materials Required
Patient Information Sheet
Informed consent form
Case report form
PCOSQOL scale 45-57
Study Criteria
This participants selection based on the inclusion and exclusion criteria.
Inclusion Criteria
Women at reproductive age (18-45 years)
Menstrual Irregularities
Other co-morbid conditions
Exclusion Criteria
Women older than 45 years
Amenorrhea of menopause
Materials Required:
- Data Collection form
- Patient Information Sheet
- Informed consent form
Method Of Study
This study was initiated after getting the approval from IRB & Institute Ethics Committee.
All patients age between 18-45 years old with PCOS attending to the OPD of our study site, during the study period of 4 months will be including in the study after taking information consent.
All the demographic and clinical detail of the patient will be filled in a predesign case report form.
To assess quality of life and to assess psychological burden “PCOSQOL 45-57” scale was used and score of above mention scale is calculated and recorded.
Statistical Analysis
All collected data were recorded into Microsoft excel After checking, appropriate coding of the data was done All the recorded data was analyzed using Microsoft excel All the quantitative data were represented in percentage (%) and mean + standard deviation.
Graphical representative was used for better understanding of data.
RESULTS
We collect the data from trial site Akanksha Hospital Anand (2nd September 2023 to 2nd march 2024).
Total one hundred twenty -seven patients of PCOS were enrolled in our study, out of them married total female patients of PCOS is more as compared to unmarried female patients.
Table 1. Detail about marital status
|
Married |
Unmarried |
|
102 |
25 |
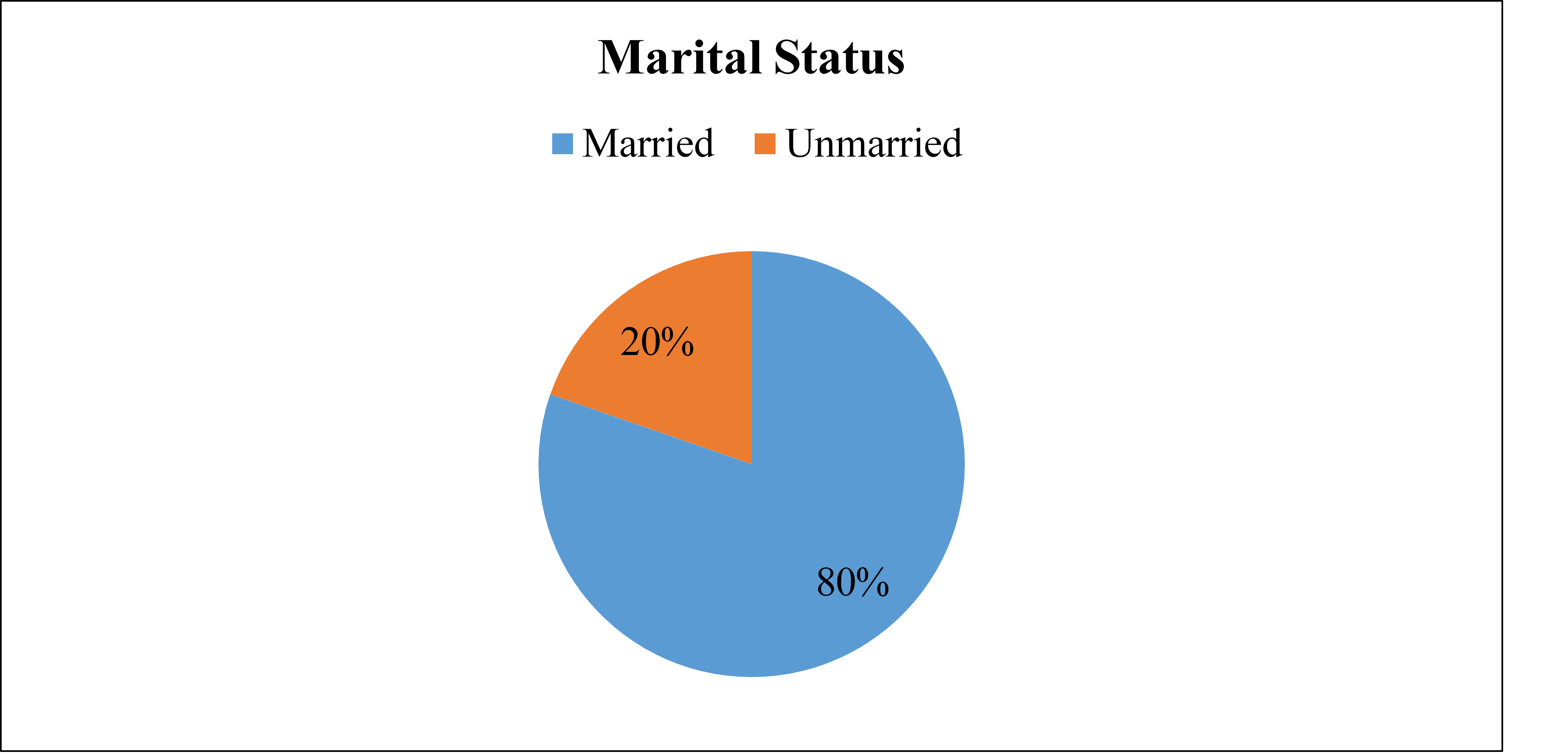
Pie Chart 1. Marital status distribution in PCOS.
Total one hundred twenty -seven patients of PCOS from which one hundred two female patients were married and twenty-five patients were unmarried and according to percentage 80% percentage were married female patients and20% were unmarried female patients this data shown on pie chart 1 & Table 1.
We had included only age between 18 to 45; patients of age below18 or above 45 were excluded. In which the maximum number of patients were found in the age group of 31- 35 year and total number of this age were 40, then in age of 18-25 age group we found 29 patients; in the age of 26 – 30 age group we found 33; in age of 36-40 age group we found 21 patients; and least number of patients had the age of 41-45 year and total number of this age were 4. This data is shown on graph 2 & Table 2.
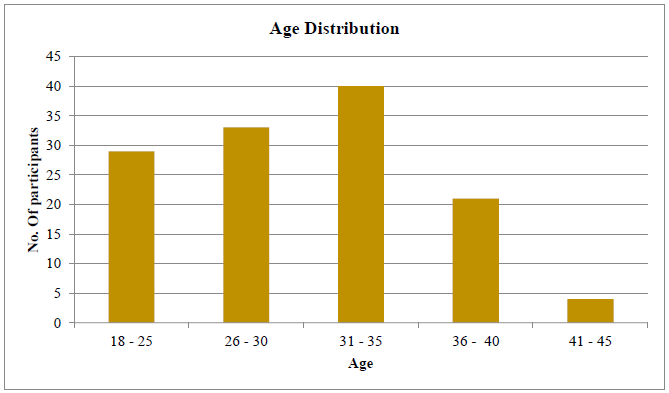
Graph 2. Age distribution in PCOS.
In our study out of 127 patients,17 patients were found underweight BMI (>18.5), 23 patients were found normal BMI (18.5-24.9), 66 patients were found over weight BMI (25 – 29.9) & 20 patients were found obese (>30). In our study, Patients who more affected to the PCOS.
Were profession of Job and number of this 38 (29.92%), house wife’ s also affected by the PCOS (N=66, 51.96%) and other 23 students were also affected by the PCOS (18.11%).
Table 2. Variables and characteristics of participants
|
Variables |
Characteristics |
Participants |
% |
|
Age (Year) |
18 - 25 |
29 |
22.83% |
|
26 - 30 |
33 |
25.98% |
|
|
31 - 35 |
40 |
31.49% |
|
|
36 - 40 |
21 |
16.53% |
|
|
41 - 45 |
4 |
3.14% |
|
|
Marital Status |
Married |
102 |
80.31% |
|
Unmarried |
25 |
19.68% |
|
|
BMI |
Under Weight (<18.5) |
17 |
13.38% |
|
Normal (18.5 - 24.9) |
23 |
18.11% |
|
|
Over Weight (25 - 29.9) |
67 |
52.75% |
|
|
Obese (>30) |
20 |
15.74% |
|
|
Occupation |
Student |
23 |
18.11% |
|
Job |
38 |
29.92% |
|
|
Housewife |
66 |
51.96% |
|
|
Family History |
Present |
57 |
44.88% |
|
Absent |
70 |
55.11% |
|
|
Medication History |
Yes |
42 |
33.07% |
|
No |
85 |
66.92% |
Total 127 patients, in which patients not taking any type of medication for PCOS were more (N=85, 66.92%) as compared to the patients taking medication (N=42, 33.07%) for the PCOS.
In Physiological and emotional status, the agree, highly agree and Disagree responses of number of participant were given in the below graph.
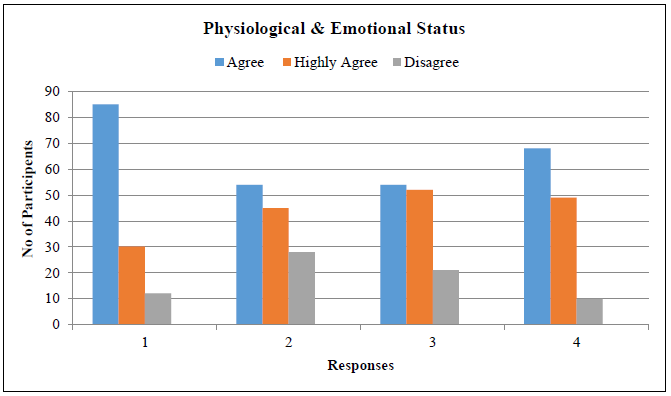
Chart 3. Physiological & Emotional status in PCOS.
Table 3. Physiological & Emotional status
|
Physiological & Emotional Status |
Agree |
|
Highly Agree |
Disagree |
|
1 |
85 |
|
30 |
12 |
|
2 |
54 |
|
45 |
28 |
|
3 |
54 |
|
52 |
21 |
|
4 |
68 |
|
49 |
10 |
|
QUESTIONS |
|
|
1 |
Suffered from bad mood due to PCOS? |
|
2 |
Suffered from low self-esteem due to PCOS? |
|
3 |
Felt easily tired & fear of diseases such as diabetes, hypertension & heart diseases? |
|
4 |
Felt of lack of family support and acceptance of disease? |
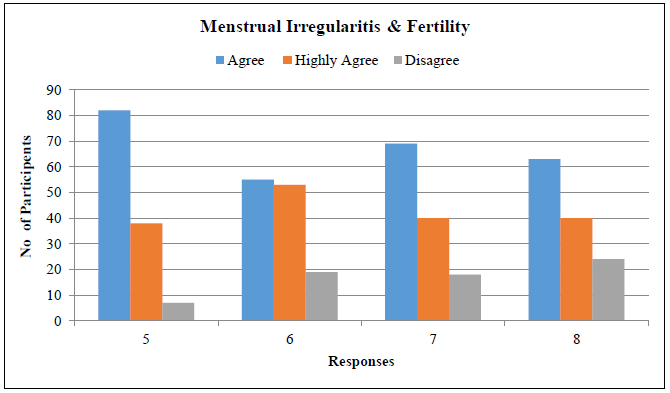
Chart 4. Menstrual irregularities & Fertility in PCOS.
Table 5. Menstrual irregularities status
|
Menstrual Irregularities & Fertilities |
Agree |
Highly Agree |
Disagree |
|
5 |
82 |
38 |
7 |
|
6 |
55 |
53 |
19 |
|
7 |
69 |
40 |
18 |
|
8 |
63 |
40 |
24 |
|
QUESTIONS |
|
|
5 |
Felt concerned about menstruation at long intervals? |
|
6 |
Felt concerned about cessation of menstruation? |
|
7 |
Felt the regular need for oral contraceptive pills to control PCOS? |
|
8 |
Felt the need to decrease your weight to control PCOS? |
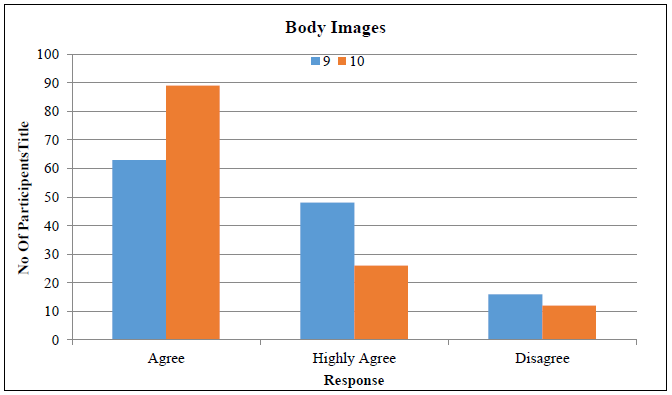
Chart 5. Body Image in PCOS.
Table 7. Body Image status
|
Body Image |
Agree |
Highly Agree |
Disagree |
|
9 |
63 |
48 |
16 |
|
10 |
89 |
26 |
12 |
|
QUESTIONS |
|
|
9 |
Dissatisfied with some aspects of your appearance? |
|
10 |
Felt others are speaking negatively about your appearance? |
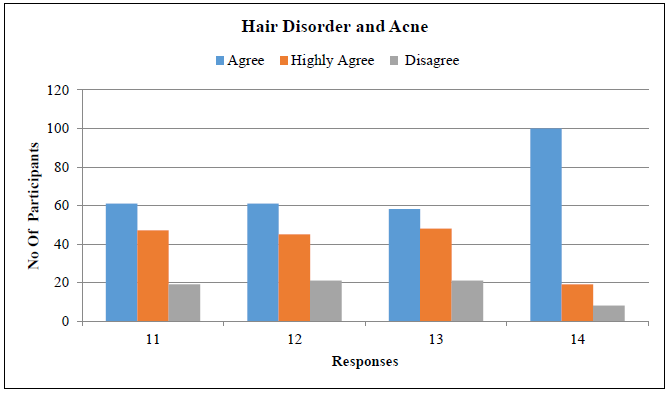
Chart 6. Hair disorder & Acne in PCOS.
Table 9. Hair disorder & Acne status
|
Hair disorder and acne |
Agree |
Highly Agree |
Disagree |
|
11 |
61 |
47 |
19 |
|
12 |
61 |
45 |
21 |
|
13 |
58 |
48 |
21 |
|
14 |
100 |
19 |
8 |
|
QUESTIONS |
|
|
11 |
Felt embarrassed about having excess facial and body hair (Hirsutism)? |
|
12 |
Felt concerned about rapid regrowth of unwanted hair after its remove? |
|
13 |
Felt that acne is affecting your appearance? |
|
14 |
Felt that alopecia is affecting your appearance? |
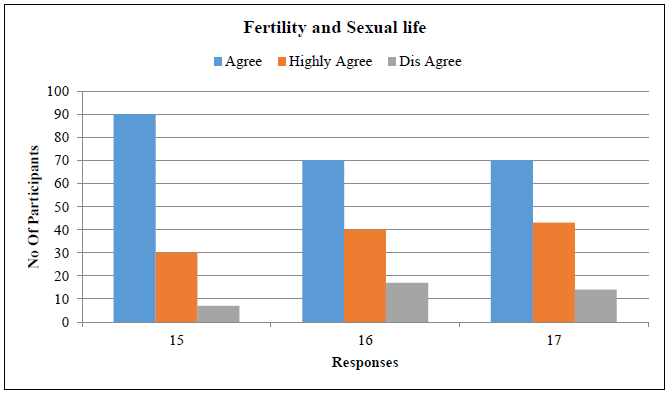
Chart 7. Fertility & Sexual life in PCOS.
Table 11. Fertility and Sexual life status
|
Fertility and Sexual life |
Agree |
Highly Agree |
Disagree |
|
15 |
90 |
30 |
7 |
|
16 |
70 |
40 |
17 |
|
17 |
70 |
43 |
14 |
|
QUESTIONS |
|
|
15 |
Felt a lack of sexual desire/ unsatisfied with sexual life? |
|
16 |
Felt sad seeing pregnant women & children? |
|
17 |
Felt fear of abortion? |
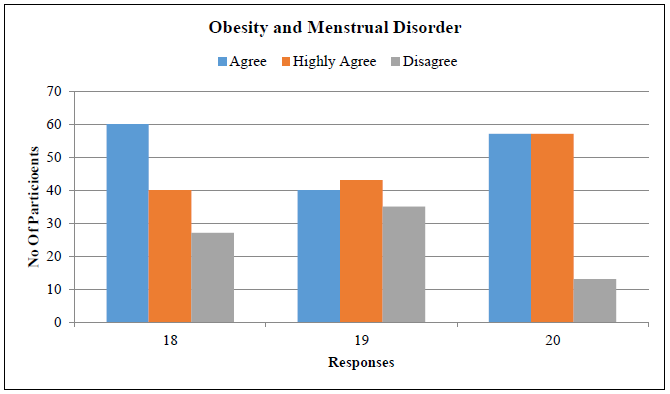
Chart 8. Obesity & Menstrual disorder in PCOS.
Table 13. Obesity & Menstrual disorder status
|
Hair disorder and acne |
Agree |
Highly Agree |
Disagree |
|
18 |
60 |
40 |
27 |
|
19 |
40 |
43 |
35 |
|
20 |
57 |
57 |
13 |
|
QUESTIONS |
|
|
18 |
Felt concerned about being overweight? |
|
19 |
Felt concerned about a fast return to your previous weight after any weight loss? |
|
20 |
Felt for life style modification to minimize and control PCOS? |
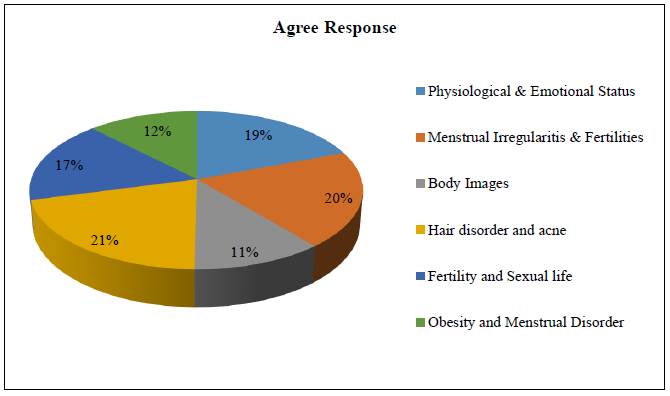
Chart 9. Agree response of participants.
Table 15. Agree factors
|
Agree Factors |
|
|
Factors |
Response |
|
Physiological & Emotional Status |
261 |
|
Menstrual Irregularities & Fertilities |
269 |
|
Body Images |
152 |
|
Hair disorder and acne |
280 |
|
Fertility and Sexual life |
230 |
|
Obesity and Menstrual Disorder |
166 |
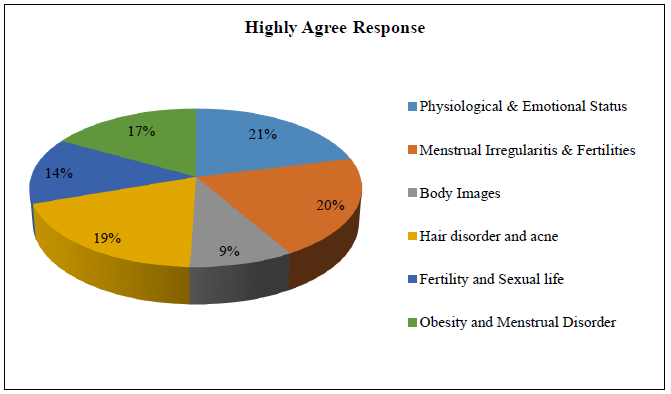
Chart 10. Highly Agree response of participants.
Table 16. Highly agree factors
|
Highly Agree Factors |
|
|
Factors |
Response |
|
Physiological & Emotional Status |
176 |
|
Menstrual Irregularities & Fertilities |
171 |
|
Body Images |
74 |
|
Hair disorder and acne |
159 |
|
Fertility and Sexual life |
113 |
|
Obesity and Menstrual Disorder |
140 |
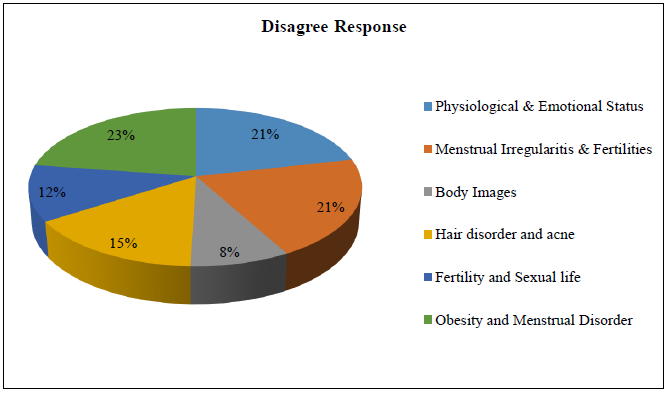
Chart 11. Disagree response of participants.
Table 17. Disagree factors
|
Disagree Factors |
|
|
Factors |
Response |
|
Physiological & Emotional Status |
71 |
|
Menstrual Irregularitis & Fertilities |
68 |
|
Body Images |
28 |
|
Hair disorder and acne |
51 |
|
Fertility and Sexual life |
38 |
|
Obesity and Menstrual Disorder |
75 |
|
Sr. No. |
Questionnaire |
Response (N= 127) |
||
|
Agree |
Highly Agree |
Disagree |
||
|
1 |
Suffered from bad mood due to PCOS? |
85 |
30 |
12 |
|
2 |
Suffered from low self-esteem due to PCOS? |
54 |
45 |
28 |
|
3 |
Felt easily tired & fear of diseases such as diabetes, hypertension & heart diseases? |
54 |
52 |
21 |
|
4 |
Felt of lack of family support and acceptance of disease? |
68 |
49 |
10 |
|
5 |
Felt concerned about menstruation at long intervals? |
82 |
38 |
7 |
|
6 |
Felt concerned about cessation of menstruation? |
55 |
53 |
19 |
|
7 |
Felt the regular need for oral contraceptive pills to control PCOS? |
69 |
40 |
18 |
|
8 |
Felt the need to decrease your weight to control PCOS? |
63 |
40 |
24 |
|
9 |
Dissatisfied with some aspects of your appearance? |
63 |
48 |
16 |
|
10 |
Felt others are speaking negatively about your appearance? |
89 |
26 |
12 |
|
11 |
Felt embarrassed about having excess facial and body hair (Hirsutism)? |
61 |
47 |
19 |
|
12 |
Felt concerned about rapid regrowth of unwanted hair after its remove? |
61 |
45 |
21 |
|
13 |
Felt that acne is affecting your appearance? |
58 |
48 |
21 |
|
14 |
Felt that alopecia is affecting your appearance? |
100 |
19 |
8 |
|
15 |
Felt a lack of sexual desire/ unsatisfied with sexual life? |
90 |
30 |
7 |
|
16 |
Felt sad seeing pregnant women & children? |
70 |
40 |
17 |
|
17 |
Felt fear of abortion? |
70 |
43 |
14 |
|
18 |
Felt concerned about being overweight? |
68 |
40 |
27 |
|
19 |
Felt concerned about a fast return to your previous weight after any weight loss? |
49 |
43 |
35 |
|
20 |
Felt for life style modification to minimize and control PCOS? |
57 |
57 |
13 |
Table 19. Statistical analysis of responses
|
Domain |
Response |
Mean |
SD |
% |
|
Physiological & Emotional Status |
Agree |
65.25 |
14.72 |
51.37% |
|
Highly Agree |
44 |
9.76 |
34.64% |
|
|
Disagree |
17.75 |
8.34 |
13.97% |
|
|
Menstrual Irregularitis & Fertilities |
Agree |
67.25 |
11.38 |
52.95% |
|
Highly Agree |
42.75 |
6.89 |
33.66% |
|
|
Disagree |
17 |
6.22 |
13.38% |
|
|
Body Images |
Agree |
76 |
18.38 |
59.84% |
|
Highly Agree |
37 |
15.55 |
29.13% |
|
|
Disagree |
14 |
2.82 |
11.02% |
|
|
Hair disorder and acne |
Agree |
70 |
20.04 |
55.11% |
|
Highly Agree |
39.75 |
60.88 |
31.29% |
|
|
Disagree |
17.25 |
6.23 |
13.58% |
|
|
Fertility and Sexual life |
Agree |
76.66 |
11.54 |
60.36% |
|
Highly Agree |
37.66 |
6.8 |
29.65% |
|
|
|
Disagree |
12.66 |
5.13 |
9.97% |
|
|
Agree |
58 |
9.53 |
45.66% |
|
Obesity and Menstrual Disorder |
Highly Agree |
46.66 |
9.07 |
36.74% |
|
|
Disagree |
25 |
11.13 |
19.68% |
One of the major diseases that mostly affect the quality of patient’s life is PCOS. The main factors of PCOS is Physiological & Emotional Status, Menstrual Irregularities & Fertilities, Body Images, Hair disorder and acne, Fertility and Sexual life and Obesity and Menstrual Disorder. There are many factors that affected to the confidence level of persons about her physical appearance.
The main aim of our study is to assess the quality of life in PCOS patients.
Assessment of quality of life
Quality of life it is defined as the feeling of joy and satisfaction with life. Quality of life (QOL), self-confidences and self-esteem in patients with PCOS diseases have not sufficiently been attended to. Since PCOS diseases affect wellbeing, general health, function, and social adaptation of the individual, they can decrease self-confidence of the patient and definitely disrupt self-image or body image, mental health, and quality of her life.
A. PCOSQoL 45-57
The aim of this questionnaire is to assess how much your PCOS problem has affected in life.
B. Uses of PCOSQoL 45-57
The PCOSQoL 45-57 questionnaire is designed for use in women. patients over the age of 18. It is self-explanatory and can be simply handed to the patient who is asked to fill it in without the need for detailed explanation. It is usually completed in one or two minutes.
Assessment of Psychological burden
In our study we had used PCOSQoL 45-57 scale for assess the psychological burden in patients with PCOS. It is a widely used instrument for assessing the symptoms of depression. It is used in many studies of depression and its treatment. The scale is designed to be applied by clinicians after structured or unstructured interview of patient to find out their symptoms of depression.
The scale is designed to assess depression by examine mood, feelings of sadness, low swelf esteem, fear of other disease symptoms.
The reason behind the use of this scale in our study is, this scale is easy to interpret without the help of any physician or doctor. Also, we assessed the depression instead of anxiety because the many studies show that PCOS patients are more suffer with depression than the anxiety.
In our study, we had evaluated each question result from the scale. Each question has the multiple options such as Agree, Highly Agree, Disagree, and we had calculated the number of patients and number of percentage form each option of individual question.
In overall 6 factors the more agree responses were found in hair and acne disorder (21%) whereas, less number of responses were found in body images (11%). Similarly, the highly agree responses were found in Physiological and emotional status (21%) whereas, less number of responses were found in body images (9%) and the more disagree responses were found in obesity and menstrual disorder and (23%) whereas, less number of responses were found in body images (8%) [10-29].
CONCLUSION
We studied the Quality of Life of PCOS patients. Investigation of the scale of PCOSQoL 45-57 showed that PCOS had impact on their emotions (self-embarrassment, self-esteem, feelings of sadness, self-confidences, overall emotional stability. In our study we collect the data of 127 participants in which 102 females were married & 25 females were unmarried, from these we concluded that PCOS is more affected in married females & lesser affected in unmarried females. As per our study we include 6 factors such as Physiological & Emotional status, Menstrual Irregularities and Infertility, Body Images, Hair Disorder and Acne, Fertility and Sexual life, Obesity and Menstrual Disorder and we found that Hair disorder and Acne is more affecting factor in PCOS Women & in contrast Body images is lesser affecting factor in PCOS women, we concluded it from PCOSQoL 45-57 Scale [30-38].
LIMITATIONS OF STUDY
- Lack of information in some case sheets
- Time constraints
- Patients not providing the proper information regarding their addictions
ACKNOWLEDGEMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
REFERENCES
- PCOS (polycystic ovary syndrome): Symptoms & treatment [Internet]. (2024). Cleveland Clinic. Available at: https://my.clevelandclinic.org/health/diseases/8316-polycystic-ovary-syndrome-pcos
- https://images.app.goo.gl/puQCqRiuFRAyThoE6
- Odhaib SA, Altemimi MT, Imran HJ. (2022). Development of the First Health-Related Quality of Life Questionnaires in Arabic for Women With Polycystic Ovary Syndrome (Part III): Scoring System Interpretation. Cureus. 14(12):e32166.
- https://images.app.goo.gl/88FW1pkguAE253TJ6
- https://images.app.goo.gl/j1JUzQEx2XBxzZd49
- https://images.app.goo.gl/YJiRbFncs3BxqqVJA
- https://images.app.goo.gl/RL7TNAZKXbyeYbzu7
- https://images.app.goo.gl/VchYnXmi2VX6oTdr9
- Rasquin LI, Anastasopoulou C, Mayrin JV. (2022). Polycystic Ovarian Disease. StatPearls Publishing. Available at: https://www.ncbi.nlm.nih.gov/books/NBK459251/
- Coffey S, Mason H. (2003). The effect of polycystic ovary syndrome on health-related quality of life. Gynecol Endocrinol. 17(5):379-386.
- Polycystic ovary syndrome (PCOS). (2022). Mayo Clinic. Available at: https://www.mayoclinic.org/diseases-conditions/pcos/symptoms- causes/syc-20353439
- Polycystic ovary syndrome (PCOS). (2022). Mayoclinic.org. Available at: https://www.mayoclinic.org/diseases-conditions/pcos/diagnosis- treatment/drc-20353443
- https://images.app.goo.gl/6bZv3RDp73H2cH1A9
- https://images.app.goo.gl/iDCj2KZuWfLcE7vg6
- https://images.app.goo.gl/Ff2h4cmAt7F3AX5c9
- https://images.app.goo.gl/FAXWzGLuXA9r6GY59
- Hahn S, Janssen OE, Tan S, Pleger K, Mann K, Schedlowski M, et al. (2005). Clinical and psychological correlates of quality-of-life in polycystic ovary syndrome. Eur J Endocrinol. 153(6):853-860.
- Bazarganipour F, Ziaei S, Montazeri A, Foroozanfard F, Kazemnejad A, Faghihzadeh S. (2014). Health-related quality of life in patients with polycystic ovary syndrome (PCOS): a model-based study of predictive factors. J Sex Med. 11(4):1023-1032.
- Kumarapeli V, Seneviratne Rde A, Wijeyaratne C. (2011). Health-related quality of life and psychological distress in polycystic ovary syndrome: a hidden facet in South Asian women. BJOG. 118(3):319-328.
- Dokras A, Sarwer DB, Allison KC, Milman L, Kris-Etherton PM, Kunselman AR, et al. (2016). Weight Loss and Lowering Androgens Predict Improvements in Health-Related Quality of Life in Women With PCOS. J Clin Endocrinol Metab. 101(8):2966-2974.
- Bazarganipour F, Ziaei S, Montazeri A, Foroozanfard F, Faghihzadeh S. (2013). Health-related quality of life and its relationship with clinical symptoms among Iranian patients with polycystic ovarian syndrome. Iran J Reprod Med. 11(5):371-378.
- Behboodi Moghadam Z, Fereidooni B, Saffari M, Montazeri A. (2018). Measures of health-related quality of life in PCOS women: a systematic review. Int J Womens Health. 10:397-408.
- Bahadori F, Jahanian Sadatmahalleh S, Montazeri A, Nasiri M. (2022). Sexuality and psychological well-being in different polycystic ovary syndrome phenotypes compared with healthy controls: a cross-sectional study. BMC Womens Health. 22(1):390.
- Bazarganipour F, Ziaei S, Montazeri A, Foroozanfard F, Kazemnejad A, Faghihzadeh S. (2013). Psychological investigation in patients with polycystic ovary syndrome. Health Qual Life Outcomes. 11:141.
- Azizi M, Elyasi F. (2017). Psychosomatic aspects of polycystic ovarian syndrome: a review. Iranian Journal of Psychiatry and Behavioral Sciences. 11(2).
- Sheikh J, Khalil H, Shaikh S, Hebbar M, Zia N, Wicks S, et al. (2023). Emotional and psychosexual well-being is influenced by ethnicity and birthplace in women and individuals with polycystic ovary syndrome in the UK and India. BJOG. 130(8):978-986.
- Chaudhari AP, Mazumdar K, Mehta PD. (2018). Anxiety, Depression, and Quality of Life in Women with Polycystic Ovarian Syndrome. Indian J Psychol Med. 40(3):239-246.
- Cronin L, Guyatt G, Griffith L, Wong E, Azziz R, Futterweit W, et al. (1998). Development of a health-related quality-of-life questionnaire (PCOSQ) for women with polycystic ovary syndrome (PCOS). J Clin Endocrinol Metab. 83(6):1976-1987.
- Bazarganipour F, Taghavi SA, Montazeri A, Ahmadi F, Chaman R, Khosravi A. (2015). The impact of polycystic ovary syndrome on the health-related quality of life: A systematic review and meta-analysis. Iran J Reprod Med. 13(2):61-70.
- McCook JG, Reame NE, Thatcher SS. (2005). Health-related quality of life issues in women with polycystic ovary syndrome. J Obstet Gynecol Neonatal Nurs. 34(1):12-20.
- Panico A, Messina G, Lupoli GA, Lupoli R, Cacciapuoti M, Moscatelli F, et al. (2017). Quality of life in overweight (obese) and normal-weight women with polycystic ovary syndrome. Patient Prefer Adherence. 11:423-429.
- Scaruffi E, Franzoi IG, Civilotti C, Guglielmucci F, La Marca L, Tomelini M, et al. (2019). Body image, personality profiles and alexithymia in patients with polycystic ovary syndrome (PCOS). J Psychosom Obstet Gynaecol. 40(4):294-303.
- Shafti V, Shahbazi S. (2016). Comparing Sexual Function and Quality of Life in Polycystic Ovary Syndrome and Healthy Women. J Family Reprod Health. 10(2):92-98.
- Wright PJ, Dawson RM, Corbett CF. (2020). Social construction of biopsychosocial and medical experiences of women with polycystic ovary syndrome. J Adv Nurs. 76(7):1728-1736.
- Rofey DL, Szigethy EM, Noll RB, Dahl RE, Lobst E, Arslanian SA. (2009). Cognitive-behavioral therapy for physical and emotional disturbances in adolescents with polycystic ovary syndrome: a pilot study. J Pediatr Psychol. 34(2):156-163.
- Patten RK, Pascoe MC, Moreno-Asso A, Boyle RA, Stepto NK, Parker AG. (2021). Effectiveness of exercise interventions on mental health and health-related quality of life in women with polycystic ovary syndrome: a systematic review. BMC Public Health. 21(1):2310.
- Odhaib SA, Altemimi MT, Imran HJ. (2022). Development of the First Health-Related Quality of Life Questionnaires in Arabic for Women With Polycystic Ovary Syndrome (Part III): Scoring System Interpretation. Cureus. 14(12):e32166.
- Watson S. (2021). Polycystic Ovary Syndrome. Available at: https://www.healthline.com/health/polycystic-ovary-disease#medical-treatment