Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2021
Accuracy of Vancomycin Dosing in the Emergency Department: Two Dosage Sizes do Not Fit All
Melissa Reeves DO1, Karina Gotliboym DO2, James Espinosa MD3*, Victor Scali DO4, Alan Lucerna DO5, Russell Mordecai DO3, Henry Schuitema DO6
1Department of Obstetrics and Gynecology, Inspira Medical Center, Vineland, NJ, 08360
2Department of Emergency Medicine, Kaiser Permanente Roseville Medical Center, Roseville, CA, USA
3Department of Emergency Medicine, Rowan University SOM/Jefferson - Stratford, NJ, USA
4Emergency Medicine Residency Academic Coordinator, Rowan University SOM/Jefferson - Stratford, NJ, USA
5Program Director, Emergency Medicine, Jefferson NJ/Rowan University SOM
6Chief, Department of Emergency Medicine, Jefferson, NJ
Received Date: March 22, 2021 Published Date: April 29, 2021
*Corresponding Author: James Espinosa, Department of Emergency Medicine,Rowan University, SOM/Jefferson - Stratford, NJ, USA, 18 East Laurel Road, Stratford, NJ 08084, E-mail: [email protected]
Copyright: Espinosa J, et al. © (2021).
Citation: Reeves M, Gotliboym K, Espinosa J, Scali V, Lucerna A, Mordecai R, et al. (2021). Accuracy of vancomycin dosing in the Emergency Department: Two dosage sizes do not fit all. Mathews J Emergency Med. 6(1):41.
ABSTRACT
Purpose of the study: The purpose of this study was to determine if vancomycin is dosed correctly---which was defined as dosing within +/- 10% of the Infectious Disease Society of America (ISDA) guidelines that recommend 15 mg/kg every 8-12 hours based on actual body weight for patients with normal renal function. A secondary goal was to determine if there is a difference in dosing compliance between attending physicians and residents. This information could then lead to a possible educational intervention to increase vancomycin dosing compliance. The model used in this study was cellulitis.
Materials and Methods:The setting was the three emergency departments of a community-based, university-affiliated hospital system.The study design was a retrospective chart review utilizing data from laboratory and emergency departments.
Results:The rate of dosing non-compliance in this study was 43.7%. The rate of compliance was 56.3%.The results show that 98.6% of the non-compliant cases were undertreated, relative to the 15 mg/kg (+/- 10%) IDSA Guidelines. Over-treatment occurred in only a single case of non-compliant treatment (1.4%). The difference between these two groups is highly statistically significant. (p=<0.001).
31% of the non-compliance derived from the Attending group and 27.9% of non-compliance was from the Resident group. The difference in performance (non-compliance) between Resident and Attending physician groups was not statistically significant. (p=0.563)Two doses (1000 mg and 1500 mg) comprised 94% of the total doses given. The 1000 mg dose was given in 84 cases (67%) and the 1500 mg dose was given in 34 cases (27%). Thus the two most common doses, given 94% of the time, generate a 43% rate of non-compliance with the correct dose target.
Conclusions: Compliance with ISDA guidelines was 56.3% with a 43.7% rate of noncompliance.The vast majority of the non-compliant cases involved under-dosing, which could lead to antibiotic resistance.
There was no statistical difference in antibiotic dosing compliance between resident and attendings physicians. The two most common doses given (1000 mg and 1500 mg) generated the 43% noncompliance. It would appear that a two dose sizes strategy, as it were, is in inadequate means to correct dosing—and that milligram per kilogram calculations with more exact dosing is needed to improve compliance. This data can be used as a baseline for improvement.Accurate dosing of vancomycin should be associated with the prevention of further antibiotic resistance.
KEYWORDS: Coagulation study utilization; Emergency medicine laboratory utilization; Choosing wisely in emergency medicine;Emergency medicine laboratory utilization economic modeling
INTRODUCTION
Antibiotic resistance is an ever increasing threat worldwide. The CDC estimates that in the United States alone, over 2 million people acquire antibiotic resistant bacterial infections and about 23,000 die per year because of them. One of the most important defenses against many antibiotic resistant bacteria such as methicillin-resistant Staphylococcus aureus(MRSA), penicillin-resistant Streptococcus pneumoniae, Clostridium difficile and multi-resistant Staphylococcus epidermidisis vancomycin. Vancomycin was developed in the 1950’s, but was not widely used for another 30 years. More recently, the rise in pseudomembranous enterocolitis and MRSA has prompted the increased use of Vancomycin [1].
Today, vancomycin is the first line drug against MRSA [2].However because of the wide and sometimes inappropriate use of the drug, there is an increase in vancomycin resistant bacteria [3]. The goal of this study was to determine if vancomycin is dosed correctly---which was defined as within +/- 10% of the IDSA guidelines that suggest 15 mg/kg every 8-12 hours based on actual body weight for patients with normal renal function or GFR of 60 mL/min per 1.73 m2 or higher [4,5]. An additional goal was to determine if there was a difference in dosing compliance between attending physicians and residents. This information can lead to a possible educational intervention to increase vancomycin dosing compliance. The model was cellulitis.
MATERIALS AND METHODS
The design was a retrospective, chart review, with data from Kennedy EDIS (ED Information System). The setting was the three campuses of the Kennedy Health System, Emergency Departments. A retrospective review of data was performed of 100 random charts pertaining to patients given vancomycin in the ED. 50 attending charts and 50 resident charts were reviewed.
The inclusion criteria were patients with cellulitis treated with intravenous vancomycin administered in the emergency department, 18 years of age or older with normal renal function. The exclusion criteria were patients less than 18 years of age or patients with abnormal renal function. Normal renal function for the purposes of this study was defined as a glomerular filtration rate (GFR) of 60 ml/min/1.73m2 or higher.
The charts were randomly selected using a random number generator. Charts were serially coded on entry into study and thus had no unique identifiers. Variables included: 1) Patient’s weight in kilograms. 2) The dose of vancomycin administered in milligrams and 3) whether the prescriber was a resident physician or an attending physician. Vancomycin doses within 10% outside (plus 10% to minus 10%) of the 15mg per kg were considered compliant. Doses falling outside plus 10% to minus 10% of 15 mg/kg were considered non-compliant. Descriptive statistical analysis was used. Tests of significance of differences between resident and attending accuracy were used.
RESULTS
What was the overall rate of compliance?
126 patients were studied.
There were 71 cases of non-compliance overall (56.3%) and 55 cases of compliance (43.7%).
Was there a difference in compliance, attending physician vs. Resident physician?
There were 71 cases of non-compliance overall (56.3% overall) with 31% of the non-compliance deriving from the Attending group and 27.9% of non-compliance from the Resident group.
The 95% confidence interval for the difference was (-0.1207, 0.0666).
The difference between the two groups was not statistically significant. (p=0.563)
This can be visualized as an individual value plot [Figure 1].
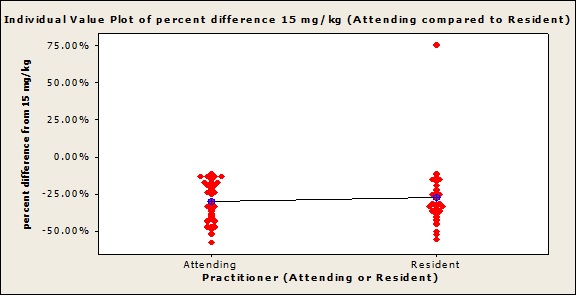
Figure 1: Individual value plot, difference between target dose of 15 mg/kg versus dose given, Attendings and Residents compared.
In non-compliant cases, was there a tendency for overtreatment or undertreatment?
98.6% of the noncompliant cases were undertreated, relative to the 15 mg per kg goal with the compliance definition as previously noted of 15 mg/kg +/- 10%.
Over-treatment occurred in only a single case. (1.4%) This is visualized in a pie chart [Figure 2]. The difference between these two percentages is highly statistically significant. (p=<0.001).
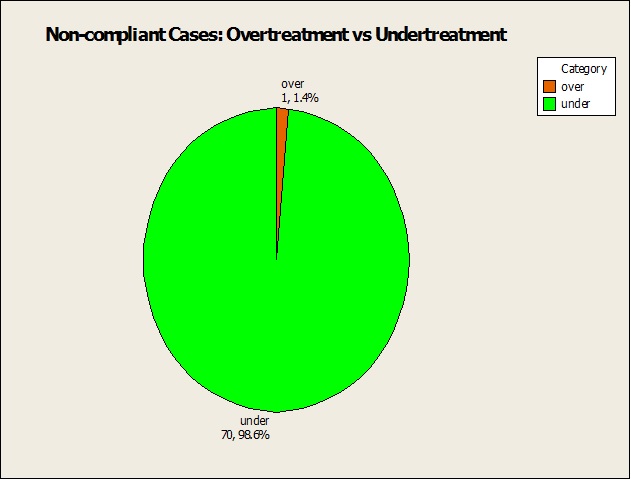
Figure 2: Pie chart, non-compliant cases, overtreatment versus undertreatment.
What were the most common doses administered?
Two doses comprise 94% of the total doses given. The two doses were a 1000 mg dose in 84 cases (67%) and a 1500 mg dose in 34 cases (27%). There were 4 cases of a 2000 mg dose (3%) and the remaining 4 cases were between 1200 mg and 1300 mg [Table 1].
A scatterplot of the mg/kg doses given versus actual weight shows two families of curves. The one curve represents the 1500 mg dose and the other the 2000 mg dose[Figure 3]. An individual value plot of the doses given visually demonstrates the overall use of two doses (1000 mg and 1500 mg) [Figure 4]. In visual contrast, a dot plot of mg/kg doses given fails to show a preponderance of dosing around 15 mg per kg [Figure 5]. Three of the four doses given in the 1200 to 1300 mg dose range were compliant (75%).
|
Dose in mg |
Count |
Percent |
|
1000 |
84 |
67% |
|
1200 |
1 |
1% |
|
1250 |
2 |
2% |
|
1300 |
1 |
1% |
|
1500 |
34 |
27% |
|
2000 |
4 |
3% |
|
Total |
126 |
100% |
Table 1: Doses given, in milligrams.
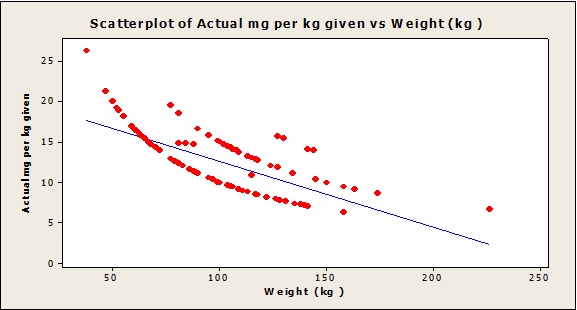
Figure 3: Scatterplot, actual mg/kg doses given in comparison to actual weight.
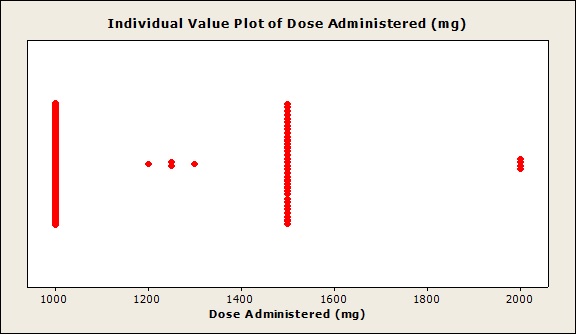
Figure 4: Individual value plot, doses administered in milligrams.

Figure 5: Dot plot, doses given in mg/kg.
DISCUSSION
The rate of non-compliance in this study (43.7%) is lower than that seen in the RosiniJM, et al. study (80%) [6]and in the study by Fuller BM, et al (78%) [7].
Thus, data from this study show a better overall compliance than in two published studies—but it would seem entirely reasonable to use this data as a baseline for improvement.
31% of the non-compliance derived from the Attending group and 27.9% of non-compliance was from the Resident group. The difference in performance (non-compliance) between Resident and Attending physician groups was not statistically significant (p=0.563). Thus, the data suggest that the non-compliance rate did not decrease as an effect of the level of experience. Thus, it would appear that training level was not a factor. It is also reasonable to conclude that educational and other components of efforts to improve compliance (and conversely, decrease non-compliance) should be directed at all emergency practitioners.
The results show that 98.6% of the non-compliant cases were undertreated, relative to the 15 mg/kg (+/- 10%) target. Over-treatment occurred in only a single case of non-compliant treatment. (1.4%)The difference between these two percentages is highly statistically significant. (p=<0.001) The rate of underdoing (undertreatment) was higher in our data (98.6%) in comparison to the study by Fuller et al, where 71% of patients were underdosed [7].This is of considerable concern, as under treatment may be related to antibiotic resistance [8].
Two doses (1000 mg and 1500 mg) comprised 94% of the total doses given. The 1000 mg dose was given in 84 cases (67%) and the 1500 mg dose was given in 34 cases (27%).
The predominant use of the 1000 mg dose was seen in the Fuller study, where 92.1% of patients received the 1000 mg dose. Thus the two most common doses, given 94% of the time, generate a 43% rate of non-compliance with the correct dose target. It would appear that a two dose sizes strategy, as it were, is in inadequate means to correct dosing—and that milligram per kilogram calculations with more exact dosing is needed to improve compliance. This data can be used as a baseline for improvement.Compliance should be associated with the prevention of further antibiotic resistance.
CONCLUSIONS
The rate of non-compliance in this study (43.7%) is lower than that seen in the RosiniJM, et al study (80%) [and in the study by Fuller BM, et al (78%). Thus, data from this study show a better overall compliance than in two published studies—but it would seem entirely reasonable to use this data as a baseline for improvement. 31% of the non-compliance derived from the Attending group and 27.9% of non-compliance was from the Resident group. The 95% confidence interval for the difference was (-0.1207, 0.0666). The difference in performance (non-compliance) between Resident and Attending physician groups was not statistically significant (p=0.563).
The data suggest that the non-compliance rate did not decrease as an effect of the level of experience. Thus, it would appear that training level was not a factor. It is also reasonable to conclude that educational components of efforts to improve compliance (and conversely, decrease non-compliance) should be directed at all emergency practitioners. The results show that 98.6% of the non-compliant cases were undertreated, relative to the 15 mg/kg (+/- 10%) target. Over-treatment occurred in only a single case of non-compliant treatment(1.4%). The difference between these two percentages is highly statistically significant(p=<0.001). The rate of underdosing (undertreatment) was higher in our data (98.6%) in comparison to the study by Fuller et al, where 71% of patients were underdosed. This is of considerable concern, as undertreatment may contribute to antibiotic resistance.
Two doses (1000 mg and 1500 mg) comprised 94% of the total doses given. The 1000 mg dose was given in 84 cases (67%) and the 1500 mg dose was given in 34 cases (27%). The predominant use of the 1000 mg dose was seen in the Fuller study, where 92.1% of patients received the 1000 mg dose. Thus the two most common doses, given 94% of the time, generate a 43% rate of non-compliance with the correct dose target. It would appear that a two dose sizes strategy, as it were, is in inadequate means to correct dosing—and that milligram per kilogram calculations with more exact dosing is needed to improve compliance. This data can be used as a baseline for improvement.Compliance should be associated with the prevention of further antibiotic resistance.
DISCLOSURE
None of the authors has any conflict of interest or financial issues to declare related to this publication. There was no funding for this study.
CONTRIBUTIONS
Design of study: all contributed
Data collection: Melissa Reeves DO, Karina Gotliboym DO, James Espinosa MD
Data analysis: James Espinosa MD
Manuscript preparation and editing: all contributed
REFERENCES
- Levine DP. (2006). Vancomycin: a history. Clin Infect Dis. 42(suppl 1):S5-12.
- Liu C, Bayer A,Cosgrove, Daum RS, Fridkin SK, et al. (2011). Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis.2011;52:e18-55.
- Limbago BM, Kallen AJ, Zhu W, Eggers P, McDougal LK, et al. (2014). Report of the 13thvancomycin-resistant Staphylococcus aureus isolate from the United States. J ClinMicrobiol. 52(3):998-1002.
- Center for Disease Control and Prevention. Antibiotic resistance threats in the United States. 2013. Available at: http://www.cdc.gov/drugresistance/threat-report-2013/pdf/ar-threats-2013-508.pdf#page=22.
- Rybak MJ, Lomaestro BM, Rotschafer JC, Moellering RC, Craig WA, et al. (2009). Vancomycin therapeutic guidelines: a summary of consensus recommendations from the Infectious Disease Society of America, the American Society of Health-system Pharmacists, and the Society of Infectious Diseases Pharmacists. Clin Infect Dis.49:325-7.
- Rosini JM, Grovola MR, Levine BJ, Jasani NB. (2013). Prescribing habits of vancomycin in the Emergency Department: are we dosing appropriately? J Emerg Med. 44(5):979-84.
- Fuller BM, Mohr N, Mueller K, McCammon C. (2013). Emergency Department vancomycin use: dosing practices and associated outcomes. J Emerg Med. 44(5):910-8.
- Sakoulas G, Moellering RC. (2006). Eliopoulos GM: Adaptation of methicillin-resistant staphylococcus aureus in the face of vancomycin therapy. Clinical Infectious Diseases. 42:40-50.