Previous Issues Volume 1, Issue 1 - 2016
Abdominal Circumference Correlates with Postural Sway of the Antero-Posterior Axis in Pregnant Women
Masanori Nagai1, Mitsuo Ishida1, 4, Junko Saitoh1, 5, Yoshie Hirata2, Hatsumi Natori2, Maki Wada3
1Department of Physiology, Yamanashi Institute of Environmental Sciences, Kenmarubi 5597-1, Fujiyoshida 4030005, Japan. 2Faculty of Nursing, Yamanashi Prefectural University, Ikeda 1-6-1, Kofu 4000062, Japan. 3College of Law, Nihon University, Misaki-cho 2-3-1, Chiyoda-ku 1018375, Japan. 4Department of Health Science, Shigakukan University, Natakayama 55, Daihu 4748651, Japan. 5Division of Homeostatic Development, National Institute for Physiology, Nishigonaka 38, Myodaiji, Okazaki 4448585, Japan.
Corresponding Author:Masanori Nagai, Department of Welfare and Psychology, Health Science University, Kodachi 7187, Fujikawaguchiko 4010380, Japan. Tel: +81-555-83-5244; Email: [email protected]
Received Date: 12 Mar 2016 Accepted Date: 15 Jun 2016 Published Date: 24 Jun 2016
Copyright © 2016 Nagai M
Citation: Nagai M, Ishida M, Saitoh J, Hirata Y, et al. (2016). Abdominal Circumference Correlates with Postural Sway of the Antero-Posterior Axis in Pregnant Women. Mathews J Gynecol Obstet. 1(1): 004.
ABSTRACT
The correlation between physical features and body sway on standing upright was explored in women before and after the delivery. Body sway during upright standing was recorded in 18 women in the third trimester and 1 month after delivery. Height, body weight, body mass index (BMI), and abdominal circumference were also registered twice. In women at the 38th week of gestation on standing upright, the abdominal circumference was positively correlated with the total path length (LNG) and enveloped area (ENV-AREA) of body sway. The path length of body sway in antero-posterior axis (Y-LNG) was also correlated with the abdominal circumference, but the path length in medio-lateral axis showed no such correlation. These correlations were not observed at 1 month after delivery. The body weight and BMI did not correlate with parameters of body sway either in the 3rd trimester or postpartum. Fast Fourier transform (FFT) analysis of body sway showed that the percentile power of the frequency band of 1.0-10.0 Hz, stabilized by the somatosensory inputs, was smaller in the 3rd trimester than that postpartum. It is hypothesized that the reliance on somatosensory information for maintaining standing posture increases as the abdominal circumference increases during pregnancy.
KEYWORDS
Pregnancy; Abdominal Circumference; Stance; Postural Sway.
INTRODUCTION
In pregnant women, standing posture changes as the fetus develops. Increasing load onto the lumbar spine and abdominal muscles causes a shift of the head position in the posterior direction and increases lumbar lordosis and anterior pelvic tilt [1, 2]. These changes in body alignment influence the stability of standing posture. Indeed, an intervention in the USA showed that almost 25% of employed women sustain a fall at work during pregnancy [3]. Stabilometric analyses of standing posture have coincidentally shown that the area of body sway increases during pregnancy [4-7]. The path length of antero-posterior body sway increases during pregnancy and decreases between late trimester and postpartum [5-8]. On the other hand, the path length of body sway in medio-lateral axis decreases or remains unchanged [5-8]. Therefore, the increase in sway area during pregnancy is mainly caused by the increase in the path length of antero-posterior body sway. We have previously shown that the power of 1.0-10.0 Hz band of body sway is smaller in pregnant women than that in nonpregnant controls [5]. Body sway of 1.0-10.0 Hz band is stabilized by somatosensory inputs [9]. Therefore, we thought that some changes in physical features during pregnancy would increase the reliance on somatosensory inputs and help to maintain the standing posture. Indeed, it has been reported that body weight positively correlates with the antero-posterior body sway in obese women on standing [10]. The body weight and fat mass increase as pregnancy proceeds [11]. The abdominal circumference also increases as the fetus develops. Therefore, in the present experiments, we explored the correlation between physical features such as body weight, body mass index (BMI) and abdominal circumference, and parameters of body sway during pregnancy employing a within-subject paradigm. Fast Fourier transform (FFT) analysis of body sway was also introduced in order to evaluate the rationale contribution of sensory inputs to maintain the standing posture, i.e., visual, somatosensory, and vestibular inputs. These sensory inputs with different modalities influence the power spectrum of body sway [9].
METHODS
Participants were 18 women who gave birth at Yamanashi Red Cross Hospital and Fujiyoshida Municipal Hospital, Yamanashi, Japan. Ten women were primiparous and 8 were multiparous. Data for the 3rd trimester were collected once after the obstetric examination on a weekly basis, and data postpartum at 1 month after delivery (Table 1).
Table 1:: Physical features of participants before and after delivery.
| Week of gestation (week) | Age (year) | Height (cm) | Body weight (kg) | BMI (kg/m2) | Abdominal circumference (cm) | |
|---|---|---|---|---|---|---|
| Before | 38.0±0.4 | 31.4±0.8 | 155.1±1.1 | 58.4*±1.0 | 24.3*±0.4 | 90.0*± 0.8 |
| After | ‡ | 31.4±0.8 | 155.1±1.1 | 51.4 ±1.0 | 21.4 ± 0.4 | 73.4 ± 1.3 |
Means and SEMs (n = 18) are shown. * Statistical significance between data (p < 0.05)‡ One month after delivery.
All experimental procedures were performed in accordance with the Ethics Committee of the Faculty of Nursing, Yamanashi Prefectural University on the basis of the Declaration of Helsinki, and informed consent of all participants was obtained in written form. Postural sway was recorded by detecting the body’s center of gravity continuously with a force platform equipped with a data processor (Gravicorder G-5500, Anima, Tokyo, Japan). Participants were requested to stand on the platform with their feet parallel, gazing at a target, a black circle with a diameter of 12 cm on a white background, fixed at a 1.5 m distance and at the height of the participant’s eyes. This arrangement of the visual target provided a visual angle of 4.58 degrees. The body sway of each participant was recorded for 1 min, first with the eyes open and next with the eyes closed. The area (ENV-AREA) and path length of body sway were registered. Spectrum analysis by fast Fourier transform (FFT) method of body sway in the medio-lateral and antero-posterior axes was performed. Power spectra of body sway were evaluated by comparing percentile powers of four frequency bands, i.e., 0.02-0.1, 0.1-0.5, 0.5-1.0, and 1.0-10.0 Hz. These four frequency bands were basically chosen according to Redfern et al. [9]. Body sway of 0.02-0.1 Hz is predominantly stabilized by visual inputs and vestibular inputs from the otoliths, and body sway of over 1.0 Hz is stabilized by somatosensory inputs from the ankles and feet. Vestibular inputs from semicircular canals exert stabilizing effects on body sway of 0.5-1.0 Hz. Differences in physical features in the 3rd trimester and after delivery were examined by Student’s t- test for paired samples. The significance of body sway parameters and power spectra was tested by one way-ANOVA. When statistical significances were confirmed, differences between mean values were further examined by Fisher’s PLSD. Correlations between physical features, i.e., body weight, BMI, and abdominal circumference and parameters of body sway were examined by Pearson’s test. The hypothesis rejection level was p < 0.05.
RESULTS
Correlations Between Physical Features and Body Sway
Between the 3rd trimester and postpartum, there were significant differences in the body weight, BMI, and abdominal circumference (Table 1). Parameters of body sway in the 3rd trimester and postpartum are shown in (Table 2).
Table 2:: Parameters of body sway before and after delivery.
| LNG (cm) | ENV-AREA (cm2) | X-LNG (cm) | Y-LNG (cm) | ||
|---|---|---|---|---|---|
| Before | Eyes open | 51.0±2.6 | 2.5±0.3 | 30.6±2.3 | 33.6±1.5 |
| Eyes closed | 63.6±4.4 | 2.5±0.3 | 34.3±3.8 | 45.4±2.8 | |
| After | Eyes open | 50.1±2.4 | 2.0±0.2 | 31.0±2.0 | 32.3±1.3 |
| Eyes closed | 61.3±3.1 | 2.4±0.3 | 35.2±2.3 | 42.1±2.4 | |
Means and SEMs (n = 18) are shown. LNG: total length of body sway, ENV-AREA: enveloped area of body sway, X-LNG: body sway in the mediolateral axis, Y-LNG: body sway in the antero-posterior axis.
Closing the eyes significantly increased LNG, X-LNG and Y-LNG before and after the delivery (F(1,17) = 36.8985, 11.117 and 42.059; p = 0.001, 0.004 and 0.000, respectively). Y-LNG tended to decrease after delivery (F(1,17) = 3.980, p = 0.062). Closing the eyes significantly increased the total path length (LNG) in the 3rd trimester and postpartum (F(1, 17) = 36.885, p = 0.000). ENV-AREA was not influenced by closing the eyes (F(1,17) = 1.621, p = 0.220). Closing the eyes significantly increased the path length in the medio-lateral (X-LNG) and antero-posterior (Y-LNG) axes (F(1,17) = 11.117 and 42.059, p = 0.004 and 0.000, respectively). There were no differences in LNG, ENV-AREA, and X-LNG between the 3rd trimester and postpartum (F(1.17) = 0.561, 1.661 and 0.092; p = 0.464, 0.215 and 0.765, respectively). Y-LNG showed a tendency to decrease after the delivery (F(1,17) = 3.980, p = 0.062).
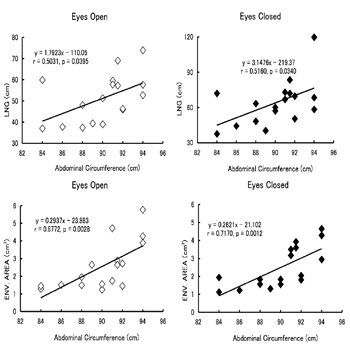
Figure 1: Correlation of the abdominal circumference and total path length (LNG) and enveloped area (ENV.AREA) of body sway in pregnant women at the third trimester.
Correlations were significant irrespective of whether the eyes were open (left half) or closed (right half). When the eyes were open, the abdominal circumference was positively correlated with LNG and ENV-AREA of body sway (r = 0.503 and 0.677, respectively). When the eyes were closed, significant correlations of the abdominal circumference with LNG and ENV-AREA were also confirmed (r = 0.519 and 0.717, respectively). At 1 month after delivery, the abdominal circumference did not significantly correlate with LNG and ENV-AREA (r = 0.030 and 0.096 while standing with the eyes open, and r = -0.087 and -0.049 with the eyes closed). The body weight and BMI significantly correlated with the abdominal circumference in the 3rd trimester (r = 0.810 and 0.692, respectively) and after delivery (r = 0.840 and 0.736, respectively). However, neither the body weight nor BMI correlated with parameters of body sway. The correlation of the abdominal circumference with X-LNG and Y-LNG was separately examined in the 3rd trimester (Figure. 2).
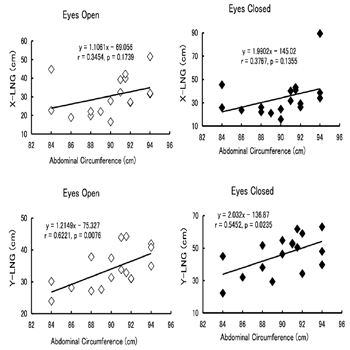
Figure 2: Correlation of the abdominal circumference and path length of body sway in the medio-lateral and antero-posterior axes (X-LNG and YLNG, respectively) in pregnant women at the third trimester.
In Y-LNG (lower panels), correlations were significant irrespective of whether the eyes were open (left half) or closed (right half). A positive correlation between the abdominal circumference and Y-LNG was confirmed (r = 0.622 with the eyes open and 0.545 with the eyes closed). However, there was no such correlation in X-LNG (r = 0.345 with the eyes open and 0.377 with the eyes closed).
Spectral Components of Body Sway
Percentile powers of 4 frequency bands, 0.02-0.1, 0.1-0.5, 0.5- 1.0, and 1.0-10.0 Hz, were compared between the 3rd trimester and postpartum. Regarding body sway in the medio-lateral axis (Figure 3), there were significant differences between the 3rd trimester and postpartum in the 0.02-0.1, 0.1-0.5 and 1.0- 10.0 Hz bands (F(1,17) = 4.406, p = 0.051; F = 5.124, p = 0.037; F = 6.314, p = 0.022, respectively). In participants standing with their eyes closed at the 3rd trimester, the percentile power of the 0.02-0.1 Hz band was greater and powers of 0.1-0.5 and 1.0-10.0 Hz bands were smaller than those postpartum (p = 0.008, 0.008 and 0.009, respectively). The effect of closing the eyes was significant in the 1.0-10.0 Hz band (F(1,17) = 9.728, p = 0.006), and the percentile power increased on closing the eyes postpartum (p = 0.005). There was no difference in the percentile power of the 0.5-1.0 Hz band between conditions.
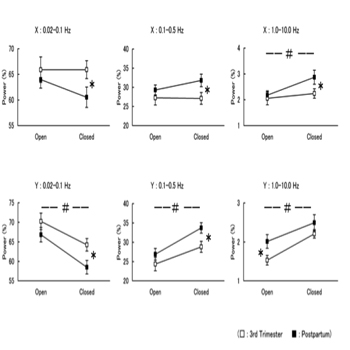
Figure 3: Percentile powers of different frequency bands of body sway in the medio-lateral (upper panels) and antero-posterior (lower panels) axes at the third trimester (open squares) and postpartum (closed squares). #: significant difference between conditions, eyes open and eyes closed. *: significant difference between the 3rd trimester and postpartum.
Regarding body sway in the antero-posterior axis (Figure 3), there were significant differences between the 3rd trimester and postpartum in the percentile powers of 0.02-0.1, 0.1-0.5 and 1.0-10.0 Hz bands (F(1,17) = 6.113, p = 0.024; F = 5.718, p = 0.029; F = 4.785, p = 0.043, respectively). For participants standing with their eyes closed in the 3rd trimester, the percentile power of the 0.02-0.1 Hz band was greater and the power of the 0.1-0.5 Hz band was smaller than those postpartum (p = 0.024, 0.029, respectively). The percentile power of the 1.0-10.0 Hz band in women standing with their eyes open was smaller in the 3rd trimester than that postpartum (p = 0.043). There was no difference in the percentile power of the 0.5-1.0 Hz band before and after delivery (F(1,17) = 0.063, p = 0.805). Concerning body sway in the antero-posterior axis, the effect of closing the eyes was significant in all frequency bands at the 3rd trimester and postpartum (F(1,17) = 8.408-23.786, p = 0.000-0.010).
DISCUSSION
For women in the 38th week of gestation, the total path length and enveloped area of body sway during upright standing were positively correlated with the abdominal circumference (Figure 1). In pregnant women standing upright, increases in the total path length and area of body sway have been previously reported [4-6]. It is possible that the increase in the antero-posterior body sway in correlation with the abdominal circumference (Figure 2) increases the total path length and area of body sway. A multiple regression analysis has shown that the contribution ratio of body weight in stabilizing the postural balance was greater than 50% in males [12]. In obese females on standing, a positive correlation between the body weight and antero-posterior body sway has been reported on one hand but an inverted correlation on the other hand [10, 13]. The latter is tentatively taken as a result of functional adaptation. In the present experiment, however, the body weight did not correlate with parameters of body sway. A preceding study has either reported no correlation between the antero-posterior body sway and weight gain in women at the last trimester [7]. Weight gain during pregnancy is more or less 10 kg [11]. In our experiment, weight gain was 7.0 kg, and BMI at the 3rd trimester did not exceed the normal range (Table 1). Unlike the case for obese population, weight gain is not a major cause for changes in sway parameters during pregnancy. Furthermore, a recent study showed that BMI does not correlate with sway parameters in pregnant women [14]. The center of mass shifts anterior to the hip and destabilizes the standing posture, although the lumbar lordosis is greater during pregnancy [2, 15]. Foot pressure increases in the anterior plantar in the late pregnancy [7]. We think that the increase in abdominal circumference, as a consequence of the fetal growth, forward sift of the center of mass and the increase in anterior plantar pressure, correlates with the antero-posterior body sway more prominently than body weight and BMI in pregnant women. It has been reported that antero-posterior body sway correlates with the feeling of balance impairment in pregnant women and decreases between the 3rd trimester and postpartum [8]. The feeling of a loss of balance may increase anxiety. We have shown that the increase in anxiety aggravates body sway in the antero-posterior axis in college students and recently in pregnant women [5, 16]. The influence of anxiety on anteroposterior body sway disappeared on closing the eyes [5, 16, 17]. However, the correlation between the abdominal circumference and antero-posterior body sway during pregnancy was observed irrespective of whether the eyes were open or closed (Figure 2). Therefore, the correlation between abdominal circumference and antero-posterior body sway reflects one facet of sensorimotor coordination independent of eye conditions. FFT analysis of body sway (Figure 3) showed that the percentile power of the frequency band of 1.0-10.0 Hz, stabilized by the somatosensory inputs, was smaller at the 3rd trimester than that postpartum. We have previously shown that the percentile power of 1.0-10.0 Hz band in the medio-lateral body sway is smaller in pregnant women in comparison to non-pregnant controls [5]. The present experiment employing a within-subject paradigm showed that the body sway of 1.0- 10.0 Hz band was smaller in both antero-posterior and medio- lateral axes during pregnancy. In the late pregnancy, the stance width is increased [18]. The increase in stance width mechanically fixes the knee joint and causes a coupling of ankle and hip movements to stabilize the medio-lateral motion by increasing proprioceptive sensitivity [19]. The total length and velocity of body sway are smaller in pregnant women at the 3rd trimester than those in non-pregnant controls while standing on a force platform with antero-posterior inclines [20]. This fact shows that sensorimotor responses induced by somatic stimulation, i.e. different angular positions of the ankle, greatly stabilize the antero-posterior body sway in the late trimester. These reports together with our result in FFT analysis suggest that the standing posture is maintained by increasing the reliance on somatosensory information during pregnancy.
CONCLUSION
Among physical features in women before and after the delivery, the abdominal circumference in the 3rd trimester positively correlates with antero-posterior body sway on standing upright. The increase in the abdominal circumference may cause the increased reliance on somatosensory information in maintaining standing posture also in the 3rd trimester. Physical features such as lumbar lordosis and pelvic tilt may also influence the reliance on somatosensory inputs in pregnant women, although we did not examine these features in the present experiment. However, the abdominal circumference is a simple measure to predict the stability of standing posture in pregnant women. Somatosensory activation by transcutaneous electrical stimulation (TENS) stabilizes the standing posture in young adults [21]. It is expected that increasing the reliance on somatosensory inputs decrease the fall in pregnant women and lead to the successful delivery.
ACKNOWLEDGEMENTS
We are very grateful to the obstetric wards staff of Yamanashi Red Cross Hospital and Fujiyoshida Municipal Hospital for allowing us to use their facilities.
REFERENCES
- Ireland ML and Ott SM. (2000). The effects of pregnancy on the musculoskeletal system. Clin Orthop. 372, 169-179.
- Franklin ME and Conner-Kerr T. (1998). An analysis of posture and back pain in the first and third trimesters of pregnancy. J Orthop Sports Phys Ther. 28(3), 133-138.
- Dunning K, LeMasters G, Levin L, Bhattacharya A, et al. (2003). Falls in workers during pregnancy: risk factors, job hazards, and high risk occupations. Am J Ind Med. 44(6), 664-672.
- Butler EE, Colon I, Druzin ML and Rose J. (2006). Postural equilibrium during pregnancy: decreased stability with an increased reliance on visual cues. Am J Obstet Gynecol 195(4), 1104-1108.
- Nagai M, Ishida M, Saitoh J, Hirata Y, et al. (2009). Characteristics of the control of standing posture during pregnancy. Neurosci Lett. 462(2), 130-134.
- Oliveira LF, Viera TM, Macedo AR, Simpson DM, et al. (2009). Postural sway changes during pregnancy: a descriptive study using stabilometry. Eur J Obstet Gynecol Reprod Biol. 147(1), 25-28.
- Karadag-Sayge E, Unlu-Ozkan F and Bagul A. (2010). Plantar pressure and foot pain in the last trimester of pregnancy. Foot Ankle Int. 31(2), 153-157.
- Jang J, Hsiao KT and Hsiao-Wecksler ET. (2008). Balance (perceived and actual) and preferred stance width during pregnancy. Clin Biomech Bristol, Avon. 23(4), 468-479.
- Menegoni F, Galli M, Tacchini E, Vismara L, et al. (2009). Gender-specific effect of obesity on balance. Obesity (Silver Spring). 17(10), 1951-1956.
- Soltani H and Fraser RB. (2000). A longitudinal study of maternal anthropometric changes in normal weight, overweight and obese women during pregnancy and postpartum. Brit J Nutr. 84(1). 95-101.
- Redfern MS, Yardley L and Bronstein M. (2001). Visual influences on balance. J Anxiety. 15(1-2), 81-94.
- Hue O, Simoneau M, Marcotte J, Berrigan F, et al. (2007). Body weight is a strong predictor of postural stability. Gait Posture. 26(1), 32-38.
- Blaszczyk JW, Cieslinska-Swider J, Plewa M, Zahorska-Markiewicz B, et al. (2009). Effects of excessive body weight on postural control. J Biomech. 42(9), 1295-1300.
- Whitcome KK, Shapiro LJ and Lieberman DE. (2007). Fetal load and the evolution of lumbar lordosis in bipedal hominius. Nature. 450(7172), 1075-1078.
- Opala-Berdzik A, Blaszczyk JW, Bacik B, Swider JC, et al. (2015). Static postural stability in women during and after pregnancy: a prospective longitudinal study. PLos One. 10(6), e0124207.
- Ohno H, Wada M, Saitoh J, Sunaga N, et al. (2004). The effects of anxiety on postural control in humans depends on visual information processing. Neurosci Lett. 364(1), 37-39.
- Wada M, Sunaga N and Nagai M. (2001). Anxiety affects the postural sway of the antero-posterior axis in college students. Neurosci Lett. 302(2-3), 157-159.
- Lymbery JK and Gilleard W. (2005). The stance of walking during late pregnancy: temporospatial and ground reaction force variables. J Amer Podiatr Med Assoc. 95(3), 247-253.
- Day BL, Steiger MJ, Thompson PD, Marsden CR, et al. (1993). Effect of vision and stance width on human body motion when standing: implications for afferent control of lateral sway. J Physiol. 469, 479-499.
- McCrory JL, Chambers AJ and Redfern MS. (2010). Dynamic postural stability during advancing pregnancy. J Biomech. 43(12), 2434-2439.
- Dickstein R, Laufer Y and Katz M. (2006). TENS to the posterior aspect of the legs decreases postural sway during stance. Neurosci Lett. 393(1), 51-55.