Information Links
Related Conferences
Previous Issues Volume 3, Issue 1 - 2023
A Systematic Review of Randomized Control Trials to Assess Exercise Prescription Practice in Tennis Elbow
Jayanti Rai1,*, Turgut E2, Ivemey E3, Towey D4, Richardson T5, Coulthard C6, Khaiyat O7, Mohammed J8
1European Society for Shoulder and Elbow Rehabilitation, Kent Community Health NHS Foundation Trust, United Kingdom
2European Society for Shoulder and Elbow Rehabilitation, United Kingdom
3,4,5Lincolnshire Community Health Services, Lincolnshire, United Kingdom
6European Society for Shoulder and Elbow Rehabilitation, Ashford and St Peters Hospital, United Kingdom
7European Society for Shoulder and Elbow Rehabilitation, Liverpool Hope University, Liverpool, United Kingdom
8European Society for Shoulder and Elbow Rehabilitation, Lincolnshire Community Health Services, Lincolnshire, United Kingdom
*Corresponding author: Jayanti Rai, PT, MSc, European Society for Shoulder and Elbow Rehabilitation, Kent Community Health NHS Foundation Trust, United Kingdom; E-mail: [email protected].
Received Date: February 03, 2023
Published Date: March 13, 2023
Citation: Jayanti R, et al. (2023). A Systematic Review of Randomized Control Trials to Assess Exercise Prescription Practice in Tennis Elbow. Mathews J Sports Med. 3(1):07.
Copyrights: Jayanti R, et al. © (2023).
ABSTRACT
Context: There are concerns about the appropriate integration of underpinning scientific rationale and methodology when designing exercise programmes for Tennis Elbow (TE) rehabilitation. Objective: To systematically review the exercise prescription practices in the management of TE. Data Source: A systematic search of MEDLINE, EMBASE, AMED, and SCOPUS (2015-2021). Study Selection: A comprehensive literature search was conducted applying recommended methods and Boolean logic with the following terms: physiotherapy; physical therapy; rehabilitation; exercise; tennis elbow; lateral epicondylitis; and lateral elbow tendinopathy. Out of the total of 848 articles that were identified from the initial search, 21 RCTs were shortlisted for the current systematic review. Study Design: Systematic Review. Level of Evidence: Level 4. Data Extraction: The Preferred Reporting Items for Systematic Reviews (PRISMA) was used to guide the search and report the process of synthesizing the results. The quality of the RCTs was assessed using The Physiotherapy Evidence Database (PEDro) scale. Information regarding the exercise prescription practice and study characteristics were extracted from the included articles. Results: On the PEDro scale, 2 RCTs were scored excellent, 11 good, 7 fair and 1 poor. The majority of the studies failed to provide sufficient scientific justification for either the exercises chosen, or the progressions implemented in order to achieve optimal results. Conclusions: There is clearly a paucity of high-quality evidence to guide physiotherapists in designing and progressing exercise programmes for patients with TE. Further research in the field of exercise prescription and related progression is required to provide more robust evidence in prescribing exercise-based interventions for the management of TE in clinical practice.
Keywords: Tennis Elbow, Exercise Dosage, Exercise Prescription, Physiotherapy.
INTRODUCTION
The term “the lawn tennis arm” from the 1880s, and today's Tennis Elbow (TE) also known as lateral epicondylitis and lateral elbow tendinopathy has been a topic of interest for decades among both sports and non-sports-related health care providers due to its impact on patients in terms of pain severity, functional limitations, and health-related quality of life [1,2]. The publication by Dr. Ferdinand Runge is widely regarded as the first to describe the symptoms, pathology, and treatment of lateral epicondylitis (tennis elbow). However, the primary objective of his work was to provide insight into the causes and treatments of writer's cramp, elegantly illustrated by four case reports. He described lateral humeral condylar tenderness and difficulty in writing [3]. In 1882, Morris coined the term “lawn tennis elbow” as he found the condition was associated with the tennis backhand stroke [4]. TE accounts for two-thirds of cases seen in general practice, with the population prevalence estimated up to 3% and an incidence of 4–7 per 1000 individuals a year [5]. While the exact underlying pathophysiological mechanism remains unclear, a multifactorial aetiology is proposed to lead to the development of TE [6].
A spectrum of clinical trials and an article have attempted to address the management of TE over the years in relation to with arguments for and against conservative and operative management, interventions [7-9]. Some studies have even suggested no intervention to be as effective as conservative or surgical management [10,11]. The physiotherapy (PT) management of TE has largely consisted of a combination of different interventions including but not limited to exercise modalities, manual therapy (joint mobilisations, soft tissue massage, trigger point, and transverse frictions), acupuncture, injections, electrotherapy modalities (therapeutic ultrasound, laser, extracorporeal shockwave therapy), splinting, bracing, taping, and nerve stimulation [12-15]. Although there is no universal gold standard interventional approach or general consensus among healthcare professionals for the optimal management of TE, potentially due to multifactorial underlying etiology exercise prescription has been broadly considered and implemented as the core component of conservative management [6]. Furthermore, the National Institute for Health and Care Excellence (NICE) guidelines recommend stretching and strengthening exercises along with eccentric loading of the wrist extensor muscles for the management of TE (NICE 2020) [16]. This has led to a considerable number of research outputs in relation to wide-ranging exercise modalities [17,18]. Amongst exercise-based protocols, eccentric exercise prescription has been suggested by a number of studies to be superior in reducing pain and improving function in tendinopathies including TE when compared to taping, ultrasound therapy, ice, heat, stretches, concentric strengthening, and friction massage [19,20]. It has been proposed that eccentric exercises positively influence tendon remodeling by means of structural adaptations, tendon length changes, reduced nerve ingrowth, and enhanced tenocyte activity [21,22]. In addition to eccentric exercises there have been an increasing number of studies investigating other potential exercise modalities and protocols such as 4-stage progressive tendon loading exercises (PTLE) and scapular muscle exercises, considering shoulder girdle weakness in patients with TE, with preliminary positive results in managing pain and function in TE [23-25]. Although exercise-based interventions are broadly practiced by healthcare professionals in various musculoskeletal settings for the management of TE and despite growing number of related studies, there remains major uncertainties in relation to underpinning scientific rationale, optimal exercise specifications and implementation methods, and appropriate outcome assessments [26,27]. A systematic review of 30 RCTs covering a total of 2123 participants reported a very low evidence in relation to the effectiveness of exercise prescription compared with passive interventions with or without invasive treatment [28]. Furthermore, while it has been reported that eccentric exercise has more efficacy in improving pain, there is no convincing evidence to support its superiority on muscle strength and function compared with concentric or isotonic exercises. This could potentially be contributed to the heterogeneity of studies, inconsistent exercise specifications and parameters, and diverse range of implementation methods [29]. Addressing these requires systematic evaluation of the literature to provide further insights into what constitutes an evidence-based exercise treatment programme particularly in relation to the exercise modality and applied dosage (i.e. the intensity, duration, frequency, and progression) of existing exercise prescription practices.
Therefore, this study aimed to systematically review common exercise prescription practices applied for the management of TE in order to underpin level of existing evidence and highlight potential future research avenues.
METHODS
A structured approach underpinned by well-established guidelines for systematic reviews was employed to ensure appropriateness of the literature search [30]. The database included PUBMED, MEDLINE, EMBASE, AMED and SCOPUS. An electronic search was undertaken to cover the period between 2015 to 2021 using Boolean logic using the following terms: physiotherapy; physical therapy; rehabilitation; exercise; tennis elbow; lateral epicondylitis; and lateral elbow tendinopathy. Text word and thesaurus searches were used to minimize chances of missing relevant articles. Identified articles were manually searched for additional references. Inclusion and exclusion criteria are summarized in Table 1. The study was registered to PROSPERO (CRD42021281976) For the benefit of the readers, Preferred Reporting Items for Systematic Reviews and Meta- Analyses (PRISMA) has been utilized to describe the search and process of elimination. (Figure 1).
Table 1. Study inclusion and exclusion criteria.
|
Inclusion |
Exclusion |
|
|
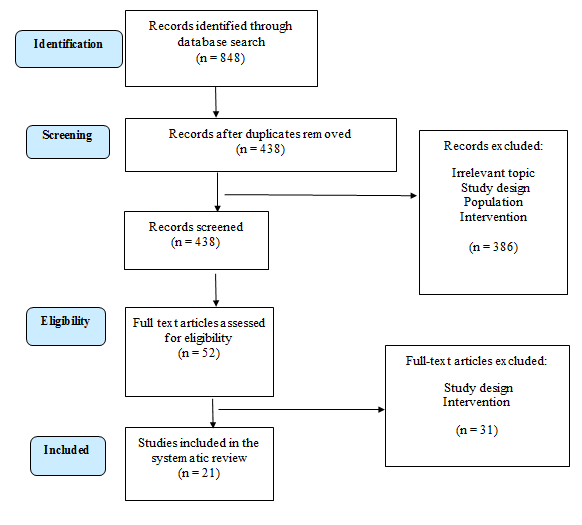
Figure 1. PRISMA flow chart.
Articles that did not meet eligibility criteria were identified from abstracts and disregarded. Full texts were obtained for remaining articles and information was extracted with regard to the Population, Intervention, Comparison, Outcome (PICO) as outlined in Table 2.
Table 2. Population, Intervention, Comparison, Outcome (PICO).
|
Parameter |
Evaluation |
Explanation |
|
Population |
Male and female patients diagnosed with TE |
Both acute and chronic TE with no surgical intervention |
|
Intervention |
Strength exercises, endurance exercises, virtual exercising tools, combination of exercise interventions |
Any intervention involving exercise and stretching |
|
Comparison |
Comparison of various exercise models and their outcomes |
E.g. exercises specifically designed as per individual patient capability and medical condition versus generalized exercises |
|
Outcomes |
|
And other relevant outcome measures found via search |
Notes: TE; Tennis Elbow, ADL; Activities of Daily Living.
RESULTS
A total of 848 articles were identified and after screening for the titles, abstracts and full text articles 21 RCTs were shortlisted for the present systematic review. The age of the participants varied between 24 to 65 years. The interventions covered across the 21 studies were stretching exercises, strengthening exercises, ultrasound therapy, transverse friction massage, splinting, continuous shortwave diathermy, gyroscopic device, isometric exercises, corticosteroid injection, joint manipulation, kinesiology taping, elbow band, functional task exercises, iontophoresis, cyriax exercises, eccentric control exercises, wait and see, and deep friction massage.
The Physiotherapy Evidence Database (PEDro) scale was used to score the quality of studies [31]. The PEDro scale was developed to help PEDro users rapidly identify the trials that are likely to be internally valid and have sufficient statistical information to guide clinical decision making. The PEDro score ranges from 0 to 10. The agreement between the two reviewers was 93.3 %. Disagreement was solved in a consensus meeting. The RCTs were scored 0 to 3 (poor), 4 to 5 (fair), 6 to 8 (good), and 9 to 10 (excellent) [32]. Out of the 21 articles 2 [33,34] scored as excellent, 11 [35-45] as good, 7 [46-52] as fair and 1 [53] as poor. Table 3 summarizes the PEDro Score for the included studies. Furthermore, the authors appraised the questions to help understand the exercise prescription practices in this patient group (Table 4). Characteristics of the studies presented in Table 5.
Table 3. The Physiotherapy Evidence Database (PEDro) score for the RCTs included in the systematic review.
|
Articles |
PEDro Score |
Total Score/10 |
||||||||||
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
8 |
9 |
10 |
11 |
||
|
Fathy 2015 [47] |
yes |
yes |
no |
yes |
no |
no |
no |
yes |
no |
yes |
yes |
5 |
|
Murtezani 2015 [50] |
yes |
yes |
no |
yes |
no |
no |
yes |
no |
no |
yes |
yes |
5 |
|
Olaussen 2015 [40] |
yes |
yes |
yes |
yes |
no |
no |
no |
yes |
yes |
yes |
yes |
7 |
|
Sevier 2015 [42] |
yes |
yes |
no |
yes |
no |
no |
yes |
no |
yes |
yes |
yes |
6 |
|
Coombes 2016 [34] |
yes |
yes |
yes |
yes |
yes |
no |
yes |
yes |
yes |
yes |
yes |
9 |
|
Hassan 2016 [48] |
yes |
no |
no |
no |
no |
no |
no |
yes |
yes |
yes |
yes |
4 |
|
Wegener 2016 [45] |
yes |
yes |
yes |
yes |
no |
no |
no |
yes |
yes |
yes |
yes |
7 |
|
Nishizuka 2017 [39] |
yes |
yes |
no |
yes |
no |
no |
no |
yes |
yes |
yes |
yes |
6 |
|
Stasinopoulos 2017 [43] |
yes |
yes |
no |
yes |
no |
no |
yes |
yes |
no |
yes |
yes |
6 |
|
Upadhyay 2017 [52] |
yes |
yes |
no |
no |
no |
no |
no |
yes |
yes |
no |
yes |
4 |
|
Babaei-Mobarakeh 2018 [35] |
yes |
yes |
no |
yes |
no |
no |
yes |
yes |
yes |
yes |
yes |
7 |
|
Basak 2018 [46] |
yes |
yes |
no |
no |
no |
no |
no |
yes |
yes |
yes |
no |
4 |
|
Lee 2018 [38] |
yes |
yes |
no |
yes |
no |
no |
no |
yes |
yes |
yes |
yes |
6 |
|
Tiwari 2018 [51] |
yes |
yes |
no |
yes |
no |
no |
no |
no |
no |
yes |
yes |
4 |
|
Giray 2019 [36] |
yes |
yes |
yes |
yes |
no |
no |
yes |
yes |
no |
yes |
yes |
7 |
|
Kachanathu 2019 [37] |
yes |
yes |
yes |
yes |
no |
no |
yes |
yes |
no |
yes |
yes |
7 |
|
Babaei-Ghazani 2020 [33] |
yes |
yes |
yes |
yes |
yes |
no |
yes |
yes |
yes |
yes |
yes |
9 |
|
Deshak 2020 [53] |
yes |
no |
no |
no |
no |
no |
no |
yes |
yes |
yes |
no |
3 |
|
Ramteke 2020 [41] |
no |
yes |
no |
yes |
no |
no |
no |
yes |
yes |
yes |
yes |
6 |
|
Vuvan 2020 [44] |
yes |
yes |
yes |
yes |
no |
no |
yes |
yes |
yes |
yes |
yes |
8 |
|
Muralidharagopalan 2021 [49] |
yes |
yes |
no |
yes |
no |
no |
no |
yes |
yes |
no |
yes |
5 |
|
Articles |
How were the exercises chosen? |
Did the author follow any scientific basis or school of thought when designing an exercise program? |
Did the authors provide any justification for the set number of repetitions, sets, intensity? |
Was there a clear progression to exercises and was it appropriately designed to achieve the strength/endurance goal (considering the muscle physiology)? |
How was the baseline for the exercises calculated? |
|
Fathy, 2015 [47] |
Cyriax-type exercises adapted but no other reason provided. |
No details provided.
|
No details provided.
|
No real progression mentioned. |
No details provided. |
|
Murtenzani, 2015 [50] |
Citations were provided that stretching can reduce pain in lateral epicondyle patients. |
Only the frequency with which they were done. |
Only the frequency of exercises was provided. |
Not clearly provided. |
No details provided. |
|
Olaussen, 2015 [40] |
Yes, based on a single citation. |
Yes, minimal information provided. |
No details provided. |
No, kept the same throughout study period. |
No details provided. |
|
Sevier, 2015 [42] |
Yes. Good reasoning and citations to substantiate their use of eccentrics as gold-standard Rx for LE. |
Yes. |
Yes. Taken from a previous paper and duration of exercise exposure in order to gain effective outcomes also cited. |
Yes. Strengthening exercises were progressed as tolerated, with either sets or TheraBand resistance, or both. |
Entirely at the participant’s discretion and judgement. |
|
Coombes 2016 [34] |
Yes, concentric and eccentric wrist extension exercises, motor control retraining and global upper body strengthening exercises were prescribed based on the author’s previous study. |
No details provided.
|
No details provided.
|
No details provided.
|
No details provided. |
|
Hassan, 2016 [48] |
Citations were provided that stretching can reduce pain in lateral epicondyle patients, but only from studies which also provided strengthening as part of the intervention. |
No details provided. |
Not clearly provided. |
Not clearly provided. |
No details provided. |
|
Wegener, 2016 [45]
|
Eccentric loading was chosen on the basis of research supporting its efficacy in improving tensile strength through collagen realignment and cross-linkage formation. |
No justification for choice of reps and sets or specific exercises chosen, other than that they were eccentric. Makes reference to 2 previous studies as their justification but no other details provided.
|
Progression (consisting of increased weight - no figures of incremental progression) was instigated when patient could perform 3 sets of 15 reps without difficulty” |
No. Indication of how baseline of “500g-1 kg” was calculated or justified. |
Outcomes were pain-free grip strength tested with dynamometer and various patient questionnaires; PRTEE, SF-36 & Occupational self-assessment. Exercises designed to increase strength and were performed into some discomfort, so unclear why only pain-free strength was measured rather than MVC? |
|
Nishizuka, 2017 [39] |
No details provided. |
No details provided. |
Not clearly provided. |
Not clearly provided. |
No details provided. |
|
Stasinopoulos, 2017 [43] |
Citations were provided regarding eccentric training, an eccentric-concentric training, and an eccentric-concentric training combined with isometric contraction for tendinopathy. |
No details provided. |
Yes, 3 sets of 15 repetitions were performed. |
Based on pain experience. |
No details provided. |
|
Upadhyay, 2017 [52] |
No details provided. |
No justification provided. |
No baseline- all patients apparently performed the same exercises regardless of their baseline presentation etc. |
4 “steps” in the programme: Step 1: Isometrics (not really clear) Step 2: Resistance dynamic (presumably ecc/conc or both Step 3: As above but adding ulna deviation/radial deviation Step 4: “Occupational Training”: 4 functional tasks not related to patient’s occupation, eg. Twisting a towel and picking up buttons. It appears that all steps were introduced from the start, so not really a progression? |
No details provided. |
|
Babaei-Mobarakeh, 2018 [35] |
Based on literature showing positive effect of vibrating tools (such as the gyroscopic device) on muscle strength, range of motion, pain and health quality of people with tennis elbow injury, when compared with, for example, dumbbell exercise. Loading the muscles of the wrist, elbow, and shoulder, as extrinsic and intrinsic, “gyroscopic device” exercise has been shown to be an effective exercise therapy in the chronic phase of tennis elbow.
|
No details provided. |
No details provided. |
No progressions given – strict and same protocol used for the whole duration. Intensity changed based on patients’ characteristics only. |
No details provided. |
|
Basak, 2018 [46] |
No details provided. |
No details provided. |
Both types were evidenced from old material, latter from 1996 – however no justification as to chosen reps, sets and intensity or the prescription in general. |
No details provided. |
No details provided. |
|
Lee, 2018 [38] |
Yes. Referenced the benefits of using eccentric exercises for tendon rehabilitation. |
No details provided. |
No. Kept the same throughout study period. |
No details provided. |
No details provided. |
|
Tiwari, 2018 [51] |
No details provided. |
No details provided. |
Intensity was increased by giving the patient a thicker flex bar.
|
No details provided. |
No details provided. |
|
Giray, 2019 [36] |
Yes. Reasoning provided for why strengthening and stretching were used. |
Yes. |
Three sets of 10 repetitions were performed during each treatment, with a 1-min rest interval between each set. The eccentric exercises consisted of the following: three sets of 10 repetitions for wrist and elbow flexion; two sets of 10 repetitions for wrist extension strengthening, starting with 50% of maximum strength and density and increasing the resistance each week; and two sets of 10 repetitions for the wrist flexor and extensor muscle groups composed of 20 s of stretching and 10 s of relaxing using the unaffected hand”
|
Yes. Strengthening exercises were progressed weekly. Progression was given if the patient could withstand the pain during initial exercises. |
Calculated based on participant’s repetition. numbers to fatigue. |
|
Kachanathu, 2019 [37] |
No details provided. |
No details provided. |
Not clearly provided. |
No. Kept the same throughout study period.
|
No details provided. |
|
Babaei-Ghazani, 2020 [33] |
No mention of how they were chosen. |
No details provided. |
Stretching exercises to the wrist extensors for 30 s, 5 to 10 repetitions a day while elbow extended, wrist lift (flexion and extension) with the elbow in flexion and then progressed into elbow in extension, wrist turns (protonation and supination) with progressive resistance and grip strengthening. Progression into eccentric contractions was introduced to the patients by using the Thera band exercises after the first few sessions – no justification given for choosing these exercises. |
The level of the intensity of the exercises was individualized for each patient and variations in the repetition and the resistance were applied. Patients were encouraged to perform the exercises according to the instructions to the point that did not exacerbate discomfort. Progression of exercise type and intensity mentioned – but no details of what they were – other than type. |
No details provided. |
|
Deshak, 2020 [53] |
No details provided. |
No details provided. |
No, although parameters were stated. |
No, Kept the same throughout study period. |
No details provided. |
|
Ramteke, 2020 [41] |
No details provided. |
No details provided. |
No details provided. |
No, Kept the same throughout study period. |
No details provided. |
|
Vuvan, 2020 [44] |
Isometric exercise vs. wait-and-see chosen due to no previous research specifically testing this. |
Standardized progression provided for load (MVC) and time under tension (TUT). However, no justification (scientific/research or theoretical) for program starting level or progression speed was offered. Used guidelines from “Toigo and Boutellier - mechanobiological exercise descriptors and internationally endorsed Consensus on Exercise Reporting Template”.
|
Baseline calculated as 20% MVC against unaffected arm using a digital force gauge. |
No details provided. |
Study compared progressive isometric exercise of wrist extensors (N=21) Vs wait and see (N=19). 8 week programme starting at 20% MVC of unaffected limb, progressing by 5% MVC every 2 weeks with standardised sets. Patient tolerance and response to progression were monitored but no record that individualised amendments were made to standardised progression. No scientific basis for program design was offered, other than a the starting MVC was lowered to 20% due to the author’s previous trial finding that an MVC of 38% or 55% led to an acute increase in pain after isometric exercise. |
|
Muralidharagopalan, 2021 [49] |
No details provided. |
Eccentrics used but not referenced. |
No details provided. |
No, kept the same throughout study period. |
No details provided. |
Table 5. Characteristics of the studies.
|
Articles |
Participants |
Intervention |
Outcome Measures |
Results |
|
|
Fathy, 2015 [47] |
Total participants n = 22 (Not clear how many in control and intervention group) |
All patients - stretching exercises for extensors muscles of the wrist with holding 20 seconds at maximum range of stretching according to the patient’s tolerance + application of deep pulsed US 1.1 W/cm2 for 5 min on the most painful area of the elbow, repeated six times over two weeks. “Group A” - iontophoresis of 0.4% dexamethasone six times over the two weeks. “Group B” - 10 min application of Cyrix-type exercises of the affected tendon.
|
Hand grip strength using a CAiRY-100 handgrip Dynamometer, Visual analogue scale (VAS), The Oxford elbow score. |
No significant differences between Iontophoresis of 0.4% dexamethasone and Cyriax-type exercises. |
|
|
Murtenzani, 2015 [50] |
Exercise group n = 25
Control group n = 24 |
Exercise group: Ultrasound and exercise. |
Control group: Local infiltration of 1mL triamcinolone acetonide (10mg/mL) and 1mL lidocaine 2%. |
Pain intensity, measured with a Visual Analogue Scale (VAS), Functional disability, measured with the Patient-Rated Tennis Elbow Evaluation (PRTEE) questionnaire, Pain free grip strength. |
The exercise group reported a significantly greater increase in all variables at 12 weeks than did the control group (p<0.001). |
|
Olaussen, 2015 [40] |
N = 157 |
Physiotherapy with two corticosteroid injections and naproxen orally, Physiotherapy with two placebo injections and naproxen, Wait-and-see treatment with naproxen. |
Six-point Likert scale, Pain on 100 mm Visual Analogue Scale (VAS) Grip strength was registered with a hand-held, analogue dynamometer Pain on resisted dorsiflexion of the wrist and third finger registered on a three-point scale Pain on eight every-day activities using the Pain Free Function Index. |
Physiotherapy with deep transverse friction massage, Mills manipulation, stretching, and eccentric exercises showed no clear benefit, and corticosteroid injection gave no added effect. |
|
|
Sevier et al. 2015 [42] |
Total participants n = 107 (113 Elbows) Astym treatment (57 elbows) or eccentric exercise (56 elbows). |
Exercise Group Stretching and eccentrically focused strengthening exercises at home expanding on the program suggested by Nirschl & Kraushaar (1996), performed three times daily and eccentrically focused strengthening exercises were performed twice weekly. |
Astym treatment group were seen in a physical therapy clinic two times weekly for four weeks. At least two days were given between sessions to allow for adequate response to the theorized regenerative stimulation from Astym treatment. |
DASH, Pain with activity, Maximum grip strength and function. |
The results show that subjects who received Astym treatment reported greater reductions in disability (DASH) and greater gains in maximum grip strength than EE subjects. |
|
Coombes, 2016 [34] |
Total participants n = 24
|
Participants performed 3 experimental tasks completed in a randomized order on separate days: control (no exercise) and isometric wrist extension (10×15 s) at load 20% below (infrathreshold), and 20% above (suprathreshold) an individual’s pain threshold. |
Patient-Rated Tennis Elbow Evaluation (PRTEE) Visual analogue scale to measure the pain severity, Tampa Scale of Kinesiophobia (TSK-11). |
Increased pain intensity after an acute bout of isometric exercise performed at an intensity above, but not below, their individual pain threshold. |
|
|
Hassan, 2016 [48] |
Total participants n = 40 (Not clear how many in control and intervention group). |
Group A: Deep friction massage (5 minutes at the site of upper attachment of the common extensors of the wrist), 2) Ultrasonic therapy (3 minutes, 1.5 w/sec2 in continuous mode), 3) Using of wrist splint - 3 sessions per week for 6 weeks. Group B: Exercise in the form of stretching of wrist extensors (5 repetitions, 30 seconds in position of stretching, 30 seconds in position of release (no stretching), with elbow extended), 2) Ultrasonic therapy (3 minutes, 1.5 w/sec2 in continuous mode), 3) Using of wrist splint - 3 sessions per week for 6 weeks. |
Universal goniometer to measure ROM of wrist extension and flexion, Visual analogue scale to measure the pain severity, Squeezing sphygmomanometer to test the power of hand grip. |
Significant improvement in Group A regarding pain, ROM of wrist flexion and extension, and handgrip force. |
|
|
Wegener, 2016 [45] |
Elastic therapeutic tape and eccentric exercises Group n = 14 Sham tape and eccentric exercises Group n = 13 Eccentric exercises alone Group n = 13 |
The same home exercise program was given to each group. Sham group: Taped the same way as the intervention group; however, the tape was applied with no tension. Intervention group: Participants were shown how to apply the tape, monitor for side effects, and wearing regime was identical. Control group: Participants in this group received no taping and were provided with the structured exercise program and advice on activity modification only.
|
Patient-Rated Tennis Elbow Evaluation (PRTEE), Pain-free grip strength assessments using a calibrated Jamar dynamometer, Short Form 36 (SF-36), Occupational Self-Assessment (OSA v 2.2). |
No statistically significant differences between groups. |
|
|
Nishizuka, 2017 [39] |
Band Group n = 55
Non-band Group n = 55. |
Patients in both groups were instructed to perform wrist extensor stretching exercises for 30 s, 3 times daily, for 6 months. Band group were instructed to wear a forearm band for more than 6 h daily for at least 6 months. |
Hand10 score, Pain score (11-point numeric scale), Assessment of tenderness, Thomsen test and middle finger extension test. |
The results of the current study suggest that a forearm band may have no more than a placebo effect, and do not support the use of a forearm band based on its effectiveness. |
|
|
Stasinopoulos, 2017 [43] |
Eccentric training group n = 11 Eccentric - concentric training group n = 12 Eccentric - concentric training with isometrics group n = 11
|
Eccentric training for wrist extensors Eccentric - concentric training for wrist extensors Eccentric - concentric training with isometrics for wrist extensors with 45 second hold. In all groups, 3 sets of 15 repetitions of slow progressive exercises (eccentric, concentric, and isometric, respectively) of the wrist extensors at each treatment session were performed, with 1-minute rest interval between each set. Static stretching exercises of the wrist extensors were performed in all treatment groups. The static stretching exercises were repeated 6 times at each treatment session, 3 times before and 3 times after the exercises, with a 30-second rest interval between each repetition. 5 times a week for 4 weeks
|
Visual analogue scale (VAS) for pain and function,
Pain-free grip strength.
|
The eccentric-concentric training combined with isomentric contractions produced the largest effect in the reduction of pain and improvement of function at the end of the treatment and at any of the follow-up time points.
|
|
|
Upadhyay, 2017 [52] |
Control group n = 15 Intervention group n = 15. |
Experimental group: Progressive Strengthening Exercises and conventional therapy (i.e. Ultrasound + Deep transverse friction massage + stretching exercises). |
Control group: Conventional therapy (i.e. Ultrasound + Deep transverse friction massage + stretching exercises). |
Visual analogue scale (VAS), Patient rated tennis elbow evaluation (PRTEE) questionnaire, Pain under strain during testing of muscle strength, Isometric grip strength measured with Jamar Hydraulic Hand Dynamometer. |
Progressive strengthening exercises programme along with conventional physical therapy intervention is more effective in relieving pain, improving functional disability and improving pain free maximal isometric grip strength than conventional physical therapy alone. |
|
Babaei-Mobarakeh, 2018 [35] |
2 experimental groups n =15 in impingement syndrome group and n = 15 in tennis elbow, and one control group n =8 with impingement syndrome and n = 7 with tennis elbow. |
A resistance training program was designed using a “gyroscopic device”. The training was performed over eight weeks, three sessions a week and 30 min a session. The “Gyroscopic device” training intensity was determined by rounds per minute according to the subject's tolerance, from 2000 up to 10,000 rounds per minutes. |
Shoulder intrinsic internal and external rotators strength using Isokinetic machine, Grip strength using digital handgrip dynamometer. Isokinetic Device Pro 3 was used to measure wrist extension and shoulder strength, and shoulder and wrist proprioception. The upper quarter Y-balance test (UQYBT). |
No significant difference between two experimental groups in post-test, but between group 1 and control group, and between group 2 and control group the difference was significant. |
|
|
Basak, 2018 [46] |
Total participants n = 90 (Not clear how many in control and intervention group). |
Wrist Manipulation was performed 15 times for 20 sets, twice weekly for total 6 weeks duration.
Progressive resisted exercises performed 4-6 times a day at home. Each exercise included 10 repetitions in 2-3 sets. |
Pain Rating scale (101 NPRS), Grip strength using Jamar Handheld dynamometer, Patient Related Tennis Elbow Evaluation (PRTEE). |
Combination of wrist manipulation and progressive exercises were effective in improving elbow pain and functional disability related to Tennis Elbow. No statistically significant improvement in the Grip strength was found among the three groups. |
|
|
Lee et al., 2018 [38] |
Wrist extensor Exercise Group n = 9 Shoulder stabilization Exercise Group n = 9. |
Pre-exercises, Both groups underwent basic hyperthermia for 20 min, transcutaneous nerve simulation treatment for 15 min, and massage and stretching for 5 min. The wrist extensor eccentric strengthening exercise group performed wrist muscle eccentric contraction exercises using Thera bands. The exercise performed 15 times was equivalent to one set, and five sets were performed with a break of 1 min after each set. The shoulder stabilization exercise group performed the push-up plus exercise using slings. he exercise performed five times was equivalent to one set, and five sets were performed with a break of 1 min after each set. These interventions were conducted three times a week for three weeks for both groups. |
Pain was measured using the visual analogue scale, Digital sense of pain using in units of N/cm2 using a digital algometer, Grip strength was measured using digital grip dynamometer. |
Both groups showed a significant decrease in pain level and a significant increase in the measurement of the tenderness thresholds of the upper trapezius muscle, lateral epicondyle, and grip strength. |
|
|
Tiwari, 2018 [51] |
Group 1 n = 20 Group 2 n = 20 |
Group-1: Subjects were received treatment comprised of eccentric strengthening exercise by using a Flexbar (FBE) along with Therapeutic Ultrasound (pulse mode). |
Group 2: Subjects were received progressive eccentric and concentric resistance exercises (PRE) along with Therapeutic Ultrasound (Pulse mode). |
The patient-rated tennis elbow evaluation (PRTEE), Pain visual analogue scale (VAS), Pain free grip strength
|
Both type of exercises are effective in the relief of Pain, increase in grip strength and improvement in function |
|
Giray, 2019 [36] |
Kinesiotaping plus exercises (n = 10), sham taping plus exercises (n = 10), and control (exercises only) (n = 10). |
All recipients were provided a home exercise program including strengthening and stretching exercises. In kinesiotaping and sham taping groups, tapings were performed and changed every 3–4 d for 2 weeks. |
The patient-rated tennis elbow evaluation (PRTEE), Pain visual analogue scale (VAS), Grip strength, Disabilities of the arm, Shoulder and hand (QuickDASH). |
Kinesiotaping in addition to exercises is more effective than sham taping and exercises. |
|
|
Kachanathu, 2019 [37] |
Intervention group n = 20 Control group n = 20. |
Intervention group – Treatment as outlined in control group + Standard wrist splint (Futuro® reversible splint wrist brace), which was to be worn 6-8 hours during the day time. 9 physical therapy sessions, three per week for three weeks. |
Control group: Conservative physical therapy exercise program Ultrasonic therapy was applied on the lateral elbow, around the area of pain for a total duration of 3 minutes, with an intensity of 1.5 W/cm2 in a continuous form. Deep friction massage for approximately 5 minutes at the area of the proximal attachment of the common extensors of the wrist. 9 physical therapy sessions, three per week for three weeks. |
Pain intensity measured with the Visual Analogue Scale (VAS), Wrist ROM assessed using a universal goniometer, Grip strength measured using Sphygmomanometer. |
Short-term use of a wrist splint in addition to a physical therapy program is more effective than physical therapy alone in reducing pain. |
|
Babaei-Ghazani et al., 2020 [33] |
Experimental group n = 22
Control Group n = 21. |
Experimental Group Exercises + continuous shortwave 27.12 MHz diathermy capacitive application, 40–70 W intensity for 15 min over the elbow for 10 sessions, every other day. |
Control Group Exercises + Sham diathermy15 min over the elbow for 10 sessions, every other day. |
100 mm Visual Analogue Scale, Quick DASH, Pneumatic Grip Strength Dynamometer. |
Significant improvements in patients receiving shortwave alongside exercise, in comparison to the sham group. |
|
Deshak, 2020 [53] |
Experimental group n = 30
Control Group n = 30. |
Experimental group: Functional task exercises, 45 minutes session 10 repetitions for 4 weeks. |
Control group: Conventional therapy, 45 minutes session 10 repetitions for 4 weeks. |
Grip assessment using sphygmomanometer, Michigan hand outcome questionnaire. |
Significant improvement in hand function and grip strength with the functional task exercises in comparison with the control group. |
|
Ramteke, 2020 [41] |
Control Group n = 15 Intervention Group n = 15. |
Intervention Group: Rotator cuff strengthening along with good scapular control and conventional treatment). |
Control Group: Conventional treatment mainly electrotherapeutic modalities, elbow exercises taping). |
Pain & Functional Activity using Visual Analog Scale (VAS). |
Rotator Cuff strengthening protocol is significantly effective in Reducing pain, improving functional activity. |
|
Vuvan, 2020 [44] |
Control Group n = 19 Intervention Group n = 21. |
Control Group: Wait-and-see.
|
Intervention Group: Single supervised instruction session by a physiotherapist, followed by an 8-wk unsupervised daily program of progressive isometric exercise. |
Patient-Rated Tennis Elbow Evaluation, Global rating of change on a six-point scale, Pain-free grip strength at 8 wk. Resting and worst pain on an 11-point numerical rating scale, Thermal and pressure pain thresholds as a measure of pain sensitivity. |
Unsupervised isometric exercise was effective in improving pain and disability. |
|
Muralidharagopalan, 2021 [49] |
Injection alone group n = 24 Injection + exercises group n = 26. |
Injection Alone: 1 ml of Triamcinolone acetonide (ABBOTT) (40mg/ml) mixed with 2 cc of 2% Lignocaine and injected into the lateral epicondyle and the most tender areas surrounding it |
Injection + Exercise: 1 ml of Triamcinolone acetonide (ABBOTT) (40mg/ml) mixed with 2 cc of 2% Lignocaine and injected into the lateral epicondyle and the most tender areas surrounding it + eccentric elbow strengthening exercises monitored remotely for the next two weeks. |
Pain was measured using the visual analogue scale,
Shoulder and hand (QuickDASH) Checked for tenderness on resisted dorsiflexion of wrist and middle finger (on a 3-point scale: no tenderness, some tenderness, definitive tenderness).
|
Addition of eccentric strengthening exercises of the elbow to local corticosteroid injection produces significant improvement compared to local corticosteroid injections alone. |
According to the NICE guidelines [16], failure to respond to a course of conservative management (6-12-month) including exercise-based interventions requires referring TE patients for orthopedic consultation and the consideration of surgical intervention. It is therefore vital that conservative management follows a targeted exercise prescription approach supported by best evidence with an aim to achieve optimal results. This should then reduce the likelihood of patient referral for potentially invasive procedures and the risks that come with this, and to minimize unnecessary burdens on NHS resources. The current systematic review identified gaps in the exercise prescription practice in TE patients, highlighting the need for more robust randomised clinical trials using appropriate scientific justification to support the development and implementation of evidence-based rehabilitation programmes.
Quality of Trials
Following PEDro evaluation [34,54] of the 21 trials were classed as ‘excellent’, although the majority of studies [35-45] were classed as ‘good’. Cashin [32] cites that trials involving complex treatment interventions such as exercise, should ideally score a minimum of 8/10 on the PEDro scale. Of the trials evaluated, only 3 [33,34,44] scored 8/10 or above. Further high-quality studies are required to enhance the existing evidence base in support of use of exercise regimens in patients with TE.
Justification for Overall Exercise Prescription
‘Exercise is medicine’ is the mantra we have been hearing and preaching as healthcare professionals all our practicing life. However, Swisher (2010) [55] brings home a very important point that much needs to done when it comes to exercise prescription and as one would not simply advise patient to take medicine ‘willy nilly’, the same analogy between ‘Exercise’ & ‘Medicine’ is that exercise needs to be prescribed to the patient as a specific dosage, designed as per individual patient needs, the frequency, intensity and other parameters maters when providing a patient with an exercise program. Only 16 of the 21 articles provided a rationale for the base-line exercise prescription and only two studies tailored the exercise programme in relation to individual participants, basing decision-making upon repetitions to fatigue [36] and participants’ own judgment [42]. Wegener et al. [45] considered individual patient tolerance in their exercise intervention, however, it was unclear if any adjustments were made to personalise the programme. Vuvan [44] set the intensity of exercise intervention based upon the strength of each participant’s unaffected limb without apparent consideration of the response to exercise in the affected limb. A surprisingly low number of studies tailored their programme to the individual participants and even fewer reported monitoring methods and exercise progression dose in relation to exercise training principles such as FITT (Frequency, Intensity, Timing, and Types) [54]. Without clear evidence on how best to monitor, adapt, and progress exercise intervention for TE patients, clinicians, and physiotherapists would potentially extrapolate literature from other conditions which may not yield the same benefits as approaches specifically targeting the TE population. Future high-quality studies are required to be more explicit in outlining exercise prescription and related justification in order to guide clinicians in formatting exercise intervention plans for individual patients.
Justification for Exercise Type
Stretching Exercise
Murtezani et al. [50] utilized stretches as the sole exercise component in their control group, delivered alongside therapeutic ultrasound. Furthermore, stretches were reported to produce favorable results by Hassan et al. [48] in a comparison study. While both authors provided justification for the use of stretches in terms of pain relief, the quoted evidence was based on a study combining stretches with strengthening, not stretches in isolation [56]. Kachanathu et al. [37] incorporated stretching exercises as part of standard care in combination with ultrasound and cross-friction massage with limited rationalization for their approach as to why this was considered standard cares. Stretching exercises were combined with eccentric loading with minimal justification [40] and a strengthening programme by Giray et al. [36] who provided more substantive justification. Stretching in the absence of strength-based exercises is not supported by national guidance (NICE, 2020) [57] or by current clinical practice [11]. This may reflect why authors were not able to provide adequate explanation in support of their stretch-based interventions which in turn raises questions about their choice of intervention in the first place.
Eccentric Exercise
The benefits of eccentric exercise have been investigated and reported by a number of authors and the rationale for this form of intervention is generally well justified. Sevier et al. [42] justified their intervention based on them being considered the gold standard intervention. Lee et al. [38] and Wegener et al. [45] each provided substantive support for the use of eccentric exercises, describing collagen changes and improvements in tensile strength; enabling tendons to gain more power during activities. Despite clear evidence and rationale to support the use of eccentric exercises, some studies lacked sufficient reasoning for utilising eccentric exercises [49]. The majority of studies opting to investigate eccentric training did not make it clear if their applied protocol was based on clinical experience or scientific rationale as it is difficult to gauge an optimal eccentric loading protocol from the current available research pool [58].
Strengthening and Functional Exercise
Early evidence is available to support the application of exercises targeting global upper limb musculature to manage patients with TE [59,60]. Some articles included in the present systematic review provided further support to this approach. Ramteke et al. [41] investigated the application of global upper limb strengthening and isometric exercises in a small RCT. Despite favorable results, they failed to provide a clear rationale for the chosen approach or acknowledge pre-existing literature. Furthermore, despite acknowledging the paucity of literature to support the use of functional upper limb exercises to manage TE, Deshak et al. [53] also failed to provide any robust rationale for the applied approach. Lee et al. [38] used shoulder stabilization exercises to optimise function in their comparison study. Whilst the study rightly recognised a paucity of evidence to justify examining the intervention, it failed to highlight the existing literature in relation to the use of shoulder exercise in the management of TE.
Variability was observed with how specific exercise approaches were justified. On some occasions, authors provided a rationale based on pathology of TE, and on others it was based on cited existing research. Across several of the studies included the justification provided was either very poor or absent altogether. In several instances where approaches or aims of intervention were not justified, it impacted upon the choice of outcome measures leading to the unclarity around the optimal targets of the intervention. The findings of this study may explain the variability in both type and dose of exercise-based interventions commonly used in clinical practice for the management of TE, which is in line with results of a multi-centre service evaluation [11]. Innovative approaches to improve exercise prescription would help to support health professionals in their clinical practice. Health APPs are available to support patients and clinicians in tailoring rehabilitation, however further work is required with validation against specific protocols [61].
CONCLUSIONS
There is clearly a paucity of high-quality evidence available to guide physiotherapists and other health care providers in first designing and then suitably monitoring and progressing exercise programmes in TE patients. Based on the present systematic review, authors made the strongest and most consistent justification in relation to eccentric exercises, which could reflect the strength of the evidence base surrounding this particular approach. We recommend authors to ensure that exercise interventions are fully justified while also considering how the most appropriate outcome measures are utilised to measure and demonstrate the effects of their chosen intervention. Further research in the field of exercise prescription in terms of repetitions, load, dosage, and related progression is required in order to provide more robust evidence in prescribing exercise for the management of TE in clinical practice.
REFERENCES
- Alizadehkhaiyat O, Fisher AC, Kemp GJ, Frostick SP. (2007). Pain, functional disability, and psychologic status in tennis elbow. Clin J Pain. 23(6):482-489.
- Nirschl RP. Elbow tendinosis/tennis elbow. Clin Sports Med. 11(4):851-870.
- Stegink‐Jansen CW, Jung B, Somerson JS. (2022). Translation of Runge's 1873 publication “On the etiology and treatment of writer's cramp”: The first description of “tennis elbow”. Clin Anat. 35(3):316-322.
- Thurston AJ. (1998). Conservative and surgical treatment of tennis elbow: a study of outcome. Aust N Z J Surg. 68(8):568-572.
- Descatha A, Despréaux T, Calfee RP, Evanoff B, Saint-Lary O. (2016). Progressive elbow pain. BMJ. 353:i1391.
- Steinmann S, Pfeifer CG, Brochhausen C, Docheva D. (2020). Spectrum of tendon pathologies: Triggers, trails and end-state. Int J Mol Sci. 21(3):844.
- Alsayed A, Eid A, Fahmy FS. (2020). Arthroscopic Management of Tennis elbow. ZUMJ. 26(2):248-254.
- Korthals-de Bos IB, Smidt N, van Tulder MW. (2004). Cost effectiveness of interventions for lateral epicondylitis. Pharmacoeconomics. 22(3):185-195.
- Sayegh ET, Strauch RJ. (2015). Does nonsurgical treatment improve longitudinal outcomes of lateral epicondylitis over no treatment? A meta-analysis. Clin Orthop Rel Res. 473(3):1093-1107.
- Amar E, Chechik O, Khashan M, Lador R, Rath E. (2014). Lateral epicondylitis treatment: International survey of surgeons' preferences and literature review. Int J Clin Practice. 68(11):1383-1387.
- Bateman M, Littlewood C, Rawson B, Tambe AA. (2019). Surgery for tennis elbow: a systematic review. Shoulder Elbow. 11(1):35-44.
- Bisset L, Paungmali A, Vicenzino B, Beller E. (2005). A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. Br J Sports Med. 39(7):411-422.
- Lucado AM, Dale RB, Vincent J, Day JM. (2019). Do joint mobilizations assist in the recovery of lateral elbow tendinopathy? A systematic review and meta-analysis. J Hand Ther. 32(2):262-276. e261.
- Razi Kazemi H, Ahmadi Bani M, Pazhooman H. (2020). The Effects of Conservative Treatments on Pain, Function and Grip Strength among Patients with Tennis Elbow Syndrome: A Systematic Review. J Rafsanjan Uni Med Sci. 18(12):1287-1300.
- Yao G, Chen J, Duan Y, Chen X. (2020). Efficacy of extracorporeal shock wave therapy for lateral epicondylitis: a systematic review and meta-analysis. BioMed Res Int. 2020:2064781.
- (NICE). Tennis Elbow-NICE CKS. 2017. Available from: https://cks.nice.org.uk/tennis-elbow#!backgroundSub:2. Accessed 8 June 2020.
- Chen Z, Baker NA. (2021). Effectiveness of eccentric strengthening in the treatment of lateral elbow tendinopathy: a systematic review with meta-analysis. J Hand Ther. 34(1):18-28.
- Irby A, Gutierrez J, Chamberlin C, Thomas SJ, Rosen AB. (2020). Clinical management of tendinopathy: a systematic review of systematic reviews evaluating the effectiveness of tendinopathy treatments. Scan J Med Sci Sports. 30(10):1810-1826.
- Tyler TF, Thomas GC, Nicholas SJ, McHugh MP. (2010). Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis: a prospective randomized trial. J Shoulder Elbow Surg. 19(6):917-922.
- Woodley BL, Newsham-West RJ, Baxter GD. (2007). Chronic tendinopathy: effectiveness of eccentric exercise. Br J Sports Med. 41(4):188-198.
- Yoon SY, Kim YW, Shin IS, Kang S, Moon HI, Lee SC. (2021). The beneficial effects of eccentric exercise in the management of lateral elbow tendinopathy: A systematic review and meta-analysis. J Clin Med. 10(17):3968.
- Landesa-Piñeiro L, Leirós-Rodríguez R. (2022). Physiotherapy treatment of lateral epicondylitis: A systematic review. J Back Musculoskelet Rehabil. 35(3):463-477.
- Ortega-Castillo M, Cuesta-Vargas A, Luque-Teba A, Trinidad-Fernández M. (2022). The role of progressive, therapeutic exercise in the management of upper limb tendinopathies: Asystematic review and meta-analysis. Musculoskeletal Science and Practice. 62:102645.
- Day JM, Bush H, Nitz AJ, Uhl TL. (2015). Scapular muscle performance in individuals with lateral epicondylalgia. J Orthop Sports Phys Ther. 45(5):414-424.
- Gül S, Yilmaz H, Karaarslan F. (2022). Comparison of the effectiveness of peloid therapy and kinesio taping in tennis elbow patients: a single-blind controlled study. Int J Biometeorol. 66(4):661-668.
- Barton C, King M, Dascombe B. (2021). Many physiotherapists lack preparedness to prescribe physical activity and exercise to people with musculoskeletal pain: a multi-national survey. Phys Ther Sport. 49:98-105.
- Stenner R, Swinkels A, Mitchell T, Palmer S. (2016). Exercise prescription for patients with non-specific chronic low back pain: a qualitative exploration of decision making in physiotherapy practice. Physiother. 102(4):332-338.
- Karanasios S, Tsamasiotis GK, Michopoulos K, Sakellari V, Gioftsos G. (2021). Clinical effectiveness of shockwave therapy in lateral elbow tendinopathy: systematic review and meta-analysis. Clin Rehabil. 35(10):1383-1398.
- Yoon SY, Kim YW, Shin IS, Kang S, Moon HI, Lee SC. (2021). The Beneficial Effects of Eccentric Exercise in the Management of Lateral Elbow Tendinopathy: A Systematic Review and Meta-Analysis. J Clin Med. 10(17):3968.
- Harris JD, Quatman CE, Manring M, Siston RA, Flanigan DC. (2014). How to write a systematic review. Am J Sports Med. 42(11):2761-2768.
- Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. (2003). Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 83(8):713-721.
- Cashin AG, McAuley JH. (2019). Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J Phys. 66(1):59-59.
- Babaei-Ghazani A, Shahrami B, Fallah E. (2020). Continuous shortwave diathermy with exercise reduces pain and improves function in Lateral Epicondylitis more than sham diathermy: A randomized controlled trial. J Bodywork Mov Ther. 24(1):69-76.
- Coombes BK, Wiebusch M, Heales L, Stephenson A, Vicenzino B. (2016). Isometric exercise above but not below an individual’s pain threshold influences pain perception in people with lateral epicondylalgia. Clin J Pain. 32(12):1069-1075.
- Babaei-Mobarakeh M, Letafatkar A, Barati AH, Khosrokiani Z. (2018). Effects of eight-week “gyroscopic device” mediated resistance training exercise on participants with impingement syndrome or tennis elbow. J Bodywork Mov Ther. 22(4):1013-1021.
- Giray E, Karali‐Bingul D, Akyuz G. (2019). The effectiveness of Kinesiotaping, sham taping or exercises only in lateral epicondylitis treatment: a randomized controlled study. PM&R. 11(7):681-693.
- Kachanathu SJ, Alenazi AM, Hafez AR, Algarni AD, Alsubiheen AM. (2019). Comparison of the effects of short-duration wrist joint splinting combined with physical therapy and physical therapy alone on the management of patients with lateral epicondylitis. European J Phys Rehabil Med. 55(4):488-493.
- Lee J-h, Kim T-h, Lim K-b. (2018). Effects of eccentric control exercise for wrist extensor and shoulder stabilization exercise on the pain and functions of tennis elbow. J Phys Ther Sci. 30(4):590-594.
- Nishizuka T, Iwatsuki K, Kurimoto S, Yamamoto M, Hirata H. (2017). Efficacy of a forearm band in addition to exercises compared with exercises alone for lateral epicondylitis: a multicenter, randomized, controlled trial. J Orthop Sci. 22(2):289-294.
- Olaussen M, Holmedal Ø, Mdala I, Brage S, Lindbæk M. (2015). Corticosteroid or placebo injection combined with deep transverse friction massage, Mills manipulation, stretching and eccentric exercise for acute lateral epicondylitis: a randomised, controlled trial. BMC Musculoskelet Disord. 16(1):1-13.
- Ramteke S, Samal S. (2020). To Study the Effect of Rotator Cuff Exercises on Tennis Elbow. Indian J Public Health Res Dev. 11(3):610-614.
- Sevier TL, Stegink-Jansen CW. (2015). Astym treatment vs. eccentric exercise for lateral elbow tendinopathy: a randomized controlled clinical trial. Peer J. 3:e967.
- Stasinopoulos D, Stasinopoulos I. (2017). Comparison of effects of eccentric training, eccentric-concentric training, and eccentric-concentric training combined with isometric contraction in the treatment of lateral elbow tendinopathy. J Hand Ther. 30(1):13-19.
- Vuvan V, Vicenzino B, Mellor R, Heales LJ, Coombes BK. (2020). Unsupervised isometric exercise versus Wait-and-See for lateral elbow tendinopathy. Med Sci Sports Exerc. 52(2):287-295.
- Wegener RL, Brown T, O’Brien L. (2016). A randomized controlled trial of comparative effectiveness of elastic therapeutic tape, sham tape or eccentric exercises alone for lateral elbow tendinosis. Hand Ther. 21(4):131-139.
- Basak T, Pal TK, Saha MB, Agarwal S, Das T. (2018). Comparative efficacy of wrist manipulation, progressive exercises and both treatments in patients with tennis elbow. Int J Health Sci Res. 8(4):87-94.
- Fathy AA. (2015). Iontophoresis versus Cyriax-type exercises in chronic tennis elbow among industrial workers. Electron Physician. 7(5):1277.
- Hassan SM, Hafez AR, Seif HE, Kachanathu SJ. (2016). The effect of deep friction massage versus stretching of wrist extensor muscles in the treatment of patients with tennis elbow. Open J Ther Rehabil. 4(1):48-54.
- Muralidharagopalan NR, Gopal R, Natarajan S. (2021). Addition of Eccentric Elbow Exercises to Local Corticosteroid Injection for Tennis Elbow–A Prospective Randomized Study. European Journal of Molecular & Clinical Medicine. 7(8):3528-3537.
- Murtezani A, Ibraimi Z, Vllasolli TO. (2015). Exercise and therapeutic ultrasound compared with corticosteroid injection for chronic lateral epicondylitis: a randomized controlled trial. Ortop Traumatol Rehabil. 17(4):351-357.
- Tiwari M. (2018). Effectiveness of flex bar eccentric exercises versus progressive resistance exercises of wrist on pain, pain free grip strength and functional activities in sub-acute tennis elbow. Indian J Physiother Occup Ther. 12(3):28-32.
- Upadhyay S, Shukla Y, Patel KK. (2017). Effects of progressive strengthening exercises in chronic lateral epicondylitis. Int J Health Sci Res. 7(4):244-257.
- Deshak S, Yeole U, Moralwar S. (2020). Effect of functional task exercises on hand function and grip strength in patients with lateral epicondylitis. Indian J Public Health Res Dev. 11(6):927-932.
- Katsukawa F. (2016). FITT principle of exercise in the management of lifestyle-related diseases. Clin Calcium. 26(3):447-451.
- Swisher AK. (2010). Yes,“exercise is medicine”…. but it is so much more! Cardiopulm Phys Ther J. 21(4):4.
- Pienimäki TT, Tarvainen TK, Siira PT, Vanharanta H. (1996). Progressive strengthening and stretching exercises and ultrasound for chronic lateral epicondylitis. Physiother. 82(9):522-530.
- (NICE). Tennis Elbow, NICE-CKS. 2020. Available from: https://cks.nice.org.uk/topics/tennis-elbow/management/management/. Accessed September 16, 2021.
- Habets B, Van Cingel R. (2015). Eccentric exercise training in chronic mid‐portion A chilles tendinopathy: A systematic review on different protocols. Scan J Med Sci Sports. 25(1):3-15.
- Day JM, Bush H, Nitz AJ, Uhl TL. (2015). Scapular muscle performance in individuals with lateral epicondylalgia. J Orthop Sports Phys Ther. 45(5):414-424.
- Titchener A, Fakis A, Tambe A. (2013). Risk factors in lateral epicondylitis (tennis elbow): a case-control study. J Hand Surg. 38(2):159-164.
- Heales LJ, Randall S, Vicenzino B, Coombes BK, Obst S. (2021). An evidence-based evaluation of mobile health apps for the management of individuals with lateral elbow tendinopathy using a systematic review framework. Phys Ther Rev. 26(4):243-253.