Previous Issues Volume 1, Issue 1 - 2017
A Rare Cause of Penile Fracture: Changing the Electrical Lamp
Selcuk Sarikaya
Corresponding Author: Selcuk Sarikaya, Gulhane Research and Training Hospital, Department of Urology, Ankara Turkey, Tel: +(90) 531 6274819; E-Mail:[email protected]
Received Date: 21 Aug 2017 Accepted Date: 22 Aug 2017 Published Date: 25 Aug 2017
Copyright © 2017 Sarikaya S
Citation:Sarikaya S. (2017). A Rare Cause of Penile Fracture: Changing the Electrical Lamp. Mathews J Urol Nephrol 1(1): 003.
INTRODUCTION
Penile fracture is a urologic emegergency [1]. There are several causes of penile fracture as well as rare causes that can occur according to the habits of different populations and nations.1 Self fracture called taghaandan would be seen in east culture and number of cases were reported in the literature [2]. Also other causes are mainly traumas and most of them due to sex positions during the intercourse. ‘Woman on top’ is the most seen cause as sex position [3, 4]. There would be rare causes as it was seen in our case. Conservative and surgical approaches would be considered for the treatment. Conservative approach is mainly for mild or moderate fractures but for severe fractures and hemodynamic instabilities surgical approaches must be considered. In this study, we aimed to present a case of self-blunt trauma, which is a rare cause of penile fracture in our clinic.
CASE REPORT
A 41-year-old male patient admitted to the emergency department due to painful swelling and color change in the penis. Subsequently, the patient was consulted to our clinic. especially the fracture line extending from the left side of the penis to the dorsum of penis there were advanced ecchymosis and edema. Hemoglobin level of the patient was monitored at normal limits and vital findings were observed as stable. When the story of the patient was questioned, he stated that he fell down from the stepladder while controlling and changing the lamp of the room that was not working and it was reasonable when considering the condition of the region that he was living. Exploration and open surgical repair were planned considering the current condition of the patient. Under spinal anesthesia, the penis was removed from the circumcision line. And folds were opened to the left corpus cavernosum tissue. On the tunica albugine, there was 3 cm-long laseration line active bleeding area was observed. In addition, it was observed that the laceration line was very close to the urethra but did not cause any urethral injury (Figure 1). Following this, thelaseration line was repaired and the layers were closed and the procedure was terminated without any complication after bleeding control.
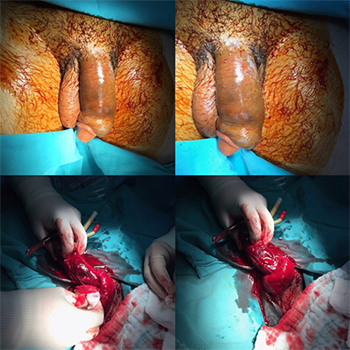
Figure 1: Penile fracture and open surgical view.
The patient was hospitalized two days postoperatively in urology clinic, and then the patient was discharged. Postoperative early and late period controls did not show any erection loss or deformity (Figure 2). The patient was included in the routine follow-up program.
DISCUSSION
The penile fracture has several causes but mainly caused by ‘taghaandan’ (self fracture) in middle-aged men, especially in the middle eastern countries, and with different sex positions, especially ‘woman on top’ position. Fracture line would be minimal and would cover a wide area as observed in our case. Conservative approach would be preferred in the treatment of penile fracture.

Figure 2: Postoperative view of penis.
Surgical intervention is also another option that would be considered according to the severity of fracture. Various postoperative complications such as erectile dysfunction and deformity can be observed in patients. Fortunately no postoperative complications were observed after surgical repair in our case and erectile functions were similar comparing to preoperative state.
REFERENCES