Information Links
Related Conferences
Previous Issues Volume 6, Issue 1 - 2024
Surgical Repair of Penile Fractures: Outcomes of a Prospective Mono-Centric Case Series Study
Mahmoud Alafifi*, Abderrahmane Doumer, Reda Safwate, Hamza Ait Mahanna, Adil Kbiro, Amine Moataz, Mohamed Dakir, Adil Debbagh, Rachid Aboutaieb
Department of Urology, University Hospital Center IbnRochd Casablanca and Faculty of Medicine and Pharmacy of Casablanca, Morocco
*Corresponding author: Dr. Mahmoud Alafifi, Department of Urology, University Hospital Center IbnRochd Casablanca and Faculty of Medicine and Pharmacy of Casablanca, 19 Tarik ibnou quartiers des hôpitaux, Morocco, Phone: +212700148612, E-mail: [email protected].
Received Date: March 18, 2024
Published Date: April 01, 2024
Citation: Al-Affifi M, et al. (2024). Surgical Repair of Penile Fractures: Outcomes of a Prospective Mono-Centric Case Series Study. Mathews J Urol Nephrol. 6(1):16.
Copyrights: Al-Affifi M, et al. © (2024).
ABSTRACT
Background: Penile fracture is a traumatic rupture of the tunica albuginea with subsequent subcutaneous hematoma with or without rupture of the corpus spongiosum and the urethra. Methods: On a duration of 6 years, we carried prospectively a single-center case-series study on fractures of the cavernous bodies of the penis within the urology department. The parameters studied were: age, mechanism of occurrence, clinical and surgical data, and then postoperative follow-up. Checks had been carried out on the 1st and 2nd week and 1st, 3rd, and 6th month. The complications were: aesthetic and functional; erectile dysfunction was assessed according to the International Erectile Function Index (IIEF-5). This work has been reported in line with the PROCESS criteria. Results: 214 patients were enrolled in the study, the average age was 39.74 years, the majority were married (66.8%). The most present clinical signs were crackling and detumescence, hematoma, and tumefaction. Misstep of coitus was the predominant mechanism followed by forced maneuver. Only 29.4% of patients had ultrasounds, and the fracture was seen in 71.42% of cases. The most used incision was coronal (80%), and 21.96% had aesthetic and/or functional complications after surgery. Conclusion: Penile fracture is primarily caused by forced maneuvers during an erect state or sexual activity. Inadequate or delayed treatment can result in functional and aesthetic complications, as observed in 21.96% of cases in our study. There is a correlation between the duration of sexual abstinence and the extent of the fracture line.
Keywords: Penile Fracture, Corpora Cavernosa, Surgery Outcome, Erectile Dysfunction.
INTRODUCTION Fracture of the corpora cavernosa is an uncommon but increasingly incident urological emergency, characterized by the rupture of the albuginea of the cavernous bodies during erections. In most cases, the diagnosis of penile fracture relies on a comprehensive medical history and physical examination. Patients often describe blunt trauma during sexual intercourse, accompanied by an audible "pop," followed by immediate pain and loss of erection. Physical examination typically reveals edema, bruising, and a characteristic penile deformity known as an "eggplant deformity." Various imaging modalities, including ultrasound, cavernosography, or MRI, may be utilized in cases where diagnosis is uncertain. Surgical management involves penile exploration, evacuation of hematoma, and repair of defects in the tunica albuginea and urethra. This can be achieved through a sub-coronal circumferential degloving incision or a longitudinal incision directly over the site of the injury. Therefore, our study aimed to assess the status of the penis after experiencing a fracture of the cavernous body.
PATIENTS AND METHODS
Between January 2017 and December 2022, spanning a duration of 6 years, we carried out a single-center case series study on fracture of the cavernous bodies of the penis within the urology department. The study included all patients aged 15 years or older experiencing a cavernous body fracture, provided they gave consent to participate. Exclusions comprised individuals with albuginea rupture due to self-harm and those with specific medical histories, including a prior cavernous body fracture, pre-existing erectile dysfunction, or penis curvature (12 patients in total). Multiple parameters were examined in our study, including age, marital status, mechanisms of occurrence, consultation time, clinical data (such as cracking sensation, penis pain, hematoma, penis curvature, and urethrorrhagia), ultrasound findings, and surgical outcomes. The study also considered the evolution of treatment, factoring in the duration of abstinence following surgery (measured in months).
The mechanisms of occurrence were categorized as follows: forced maneuver on an erect penis, shock on an erect penis and coitus misstep (including Andromachus, vaginal doggie, missionary positions and others). All patients underwent surgery within 24 hours of admission, conducted under spinal anesthesia. The choice of the surgical approach was either selective or coronal. A braided thread with rapid resorption, ranging from 3/0 or 4/0 polyglactin (Vicryl) was used for suturing on the albuginea, and if there were lesions on the urethra. Additionally, all patients received analgesics, antibiotics and anti-edematous medications. Postoperatively, the patients underwent reviews on the 7th and 15th day (for the removal of the bladder probe in case of associated urethral rupture) and at 1st, 3rd, and 6th months to monitor and address any potential complications.
Complications were categorized into two groups: (A) aesthetic, which included issues like repair scar and the persistence of penis curvature, and (B) functional, encompassing discomfort during sexual intercourse and erectile dysfunction. Erectile dysfunction was evaluated using the International Index Erectile Function-5 (IIEF-5). For patients reporting a deviation or curvature of the penis during an erection, to objectively assess this anomaly, they were asked to bring a photography during erection showing the deviation or an intracavernous injection of prostaglandin (Caverject 20μg) or saline was administered.
As flowmetry was unavailable in our department, we solely relied on the Urinary Symptom Profile (USP) score for assessing lower urinary tract disorders during the follow-up of patients with a repaired urethral lesion. Additionally, retrograde urethrocystography was conducted at six months. Data analysis was performed using SPSS software version 25, and the chi-square test was employed for comparisons, with a significance threshold set at < 5%.
This work has been reported in line with the PROCESS criteria to ensure the reliability and standardization of reporting clinical procedures.
RESULTS
We examined a total of 226 files, and after exclusions, 214 cases were considered for analysis. The average age was 39,74 years, ranging from 15 to 64 years. Of the patients, 143 were married (66.82%), and 71 were single (33.18%). A majority of our patients sought consultation within the first 24 hours (79,9% of cases), while 20.1% sought consultation after 24 hours (see Table 1). Crackling and detumescence was observed in all patients and hematoma in the genital area was the second most common symptom (see Figure 1), and the most frequently encountered mechanism of occurrence was a misstep of coitus (see Figure 2). Among the instances of interrupted coitus, specific positions were identified: the vaginal doggy style position (47 cases), the andromachus position (42 cases), the "missionary" position (31 cases) and twelve patients had their penis fractures in other positions during intercourse. Interestingly, the fractures were more frequently oriented to the right (78.97%) than to the left (21.02%).
Table 1. Demographic Characteristics of Enrolled Patients
|
Characteristic |
Total Patients (N=214) |
Details |
|
Age (years) |
Mean: 39.74 <br> Range: 15-64 |
|
|
Marital Status |
Married: 143 (66.82%) <br> Single: 71 (33.18%) |
|
|
Consultation Time |
< 24 hours: 79.9% <br> > 24 hours: 20.1% |
|
|
Mechanism of Occurrence |
Coitus misstep: Most frequent |
|
|
Orientation of Fracture |
Right: 78.97% <br> Left: 21.02% |
|
|
Hematoma Location |
Entire penis: 75.23% <br> Proximal: 18.69% <br> Distal: 6.08% |
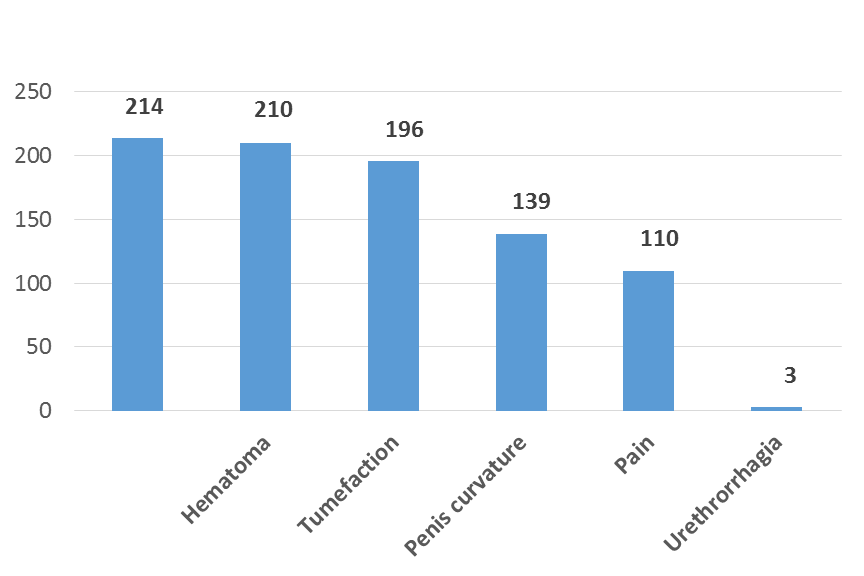
Figure 1. Distribution of patients according to clinical signs.
.png)
Figure 2. Distribution of patients by injury mechanism.
The hematoma extended across the entire penis in 75.23% of cases, sometimes localised in the proximal area (18.69%) or in the distal area (6,08%). Among the 63 patients who underwent a penile ultrasound, the fracture was identified in 45 patients. The fracture pattern was proximal, distal, and mid-axial in respectively 71%, 7%, and 22% of cases. None of the patients had an MRI scan before surgery.
A total of 172 patients underwent coronal incisions, while selective incisions were performed in 42 patients. The prevalent fracture line length ranged between 1 and 2 cm (see Figure 3). Regarding the sutures of the albuginea, all the patients had inverted stitches with long resorbing braided thread 3/0 or 4/0. The average duration of the intervention was 57,72 minutes, with a range of 30 to 150 minutes, and the normal hospitalization duration was 24 hours. No complications were observed intraoperatively or in the immediate post-operative period. However, 47 patients experienced short- and long-term complications, occurring at an average follow-up of approximately 6 months (ranging from 4 to 60 months), representing 21,96% of cases. These complications were distributed as follows: 16 cases of aesthetic complications, 13 cases of functional complications, and 18 cases involving a combination of aesthetic and functional issues. For patients with a combination of both types of complication, the complication that the patient considered to be the most troublesome was taken into account during data collection.
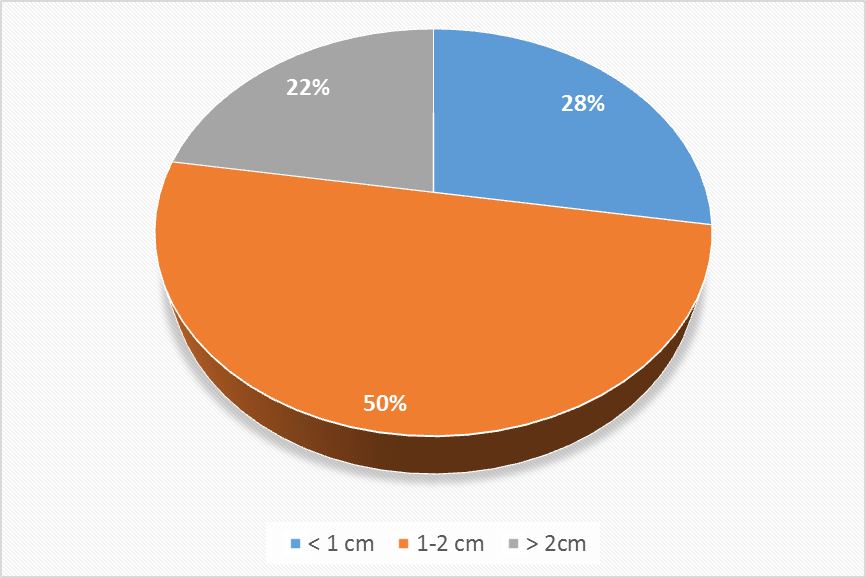
Figure 3. Distribution of patients according to the length of fracture.

Figure 4. Penile fracture cases.
During the follow-up phase, discomfort during sexual intercourse emerged as the predominant functional complication. None of the patients developed a fibrosis plaque on the penis, and 14 experienced a penis curvature with an angle less than 15°, without any impact during sexual intercourse (see Table 2). Penis curvature accounted for 30% of complications, representing 6,5% of the overall study population. The average period of abstinence after surgery was 2.1 months, with the majority of patients (86%) abstaining for one to two months. For less than a month and beyond two months, there were 11% and 3% of cases, respectively.
Table 2. Distribution of patients according to complication type
|
Complication Type |
N |
% |
|
|
Aesthetic (A) |
Penis curvature |
14 |
30 |
|
Scar |
10 |
21 |
|
|
Functional (B) |
Erectile dysfonction |
11 |
23 |
|
Discomfort during intercourse |
12 |
26 |
|
Table 3. Distribution of patients according to sexual abstinence and complications
|
A* |
B* |
A+B* |
Total* |
|
|
< 1 month |
7 |
9 |
13 |
29 |
|
1-2 months |
4 |
3 |
3 |
10 |
|
> 2 months |
5 |
1 |
2 |
8 |
|
Total |
16 |
13 |
18 |
47 |
|
Ki(2)** = 11,32 ; p < 0,05*** |
||||
Here's a breakdown of the data:
For sexual abstinence of less than 1 month, there were 7 patients in group A, 9 in group B, and 13 in group A+B, making a total of 29 patients.
For sexual abstinence of 1-2 months, there were 4 patients in group A, 3 in group B, and 3 in group A+B, totaling 10 patients.
For sexual abstinence of more than 2 months, there were 5 patients in group A, 1 in group B, and 2 in group A+B, making a total of 8 patients.
The overall totals indicate there were 16 patients in group A, 13 in group B, and 18 in group A+B, with a grand total of 47 patients.
**: The Chi-square (Ki(2) or χ²) value of 11.32 with a p-value < 0.05 suggests that there is a statistically significant difference in the distribution of complications across different durations of sexual abstinence. In simpler terms, the variation in the presence of complications (A, B, A+B) among these groups of sexual abstinence duration is unlikely to be due to chance.
***: A p-value < 0.05 typically indicates that the observed differences are statistically significant, meaning there's less than a 5% probability that these differences occurred by chance. Therefore, this result could imply that the duration of sexual abstinence might be associated with the incidence of complications in patients, although the table does not specify the nature of these complications or groups A and B. Further investigation and context would be needed to understand the implications fully and to determine any potential causality or underlying reasons for these associations.
Table 4. Distribution of patients according to the lenght of the fracture and complications
|
A* |
B* |
A+B* |
Total* |
|
|
< 1 cm |
2 |
0 |
2 |
4 |
|
1-2 cm |
3 |
1 |
2 |
6 |
|
> 2 cm |
11 |
12 |
14 |
37 |
|
Total |
16 |
13 |
18 |
47 |
|
Ki(2)** = 12,05 ; p < 0,05*** |
||||
Here's the data breakdown:
For fractures less than 1 cm, there were 2 patients in group A, 0 in group B, and 2 in group A+B, resulting in a total of 4 patients.
For fractures between 1 and 2 cm, there were 3 patients in group A, 1 in group B, and 2 in group A+B, totaling 6 patients.
For fractures greater than 2 cm, there were 11 patients in group A, 12 in group B, and 14 in group A+B, making a total of 37 patients.
Overall, there were 16 patients in group A, 13 in group B, and 18 in group A+B, with a grand total of 47 patients.
**:The Chi-square (Ki(2) or χ²) value of 12.05 with a p-value < 0.05 suggests that there is a statistically significant difference in the distribution of complications across the different fracture lengths. This means the variation in complication rates (across groups A, B, and A+B) among these categories of fracture length is unlikely due to chance.
***: A p-value < 0.05 typically indicates that the observed differences are statistically significant, implying there's less than a 5% probability that these differences occurred by chance. Therefore, this result could suggest that the length of the fracture might be associated with the incidence of complications, with longer fractures potentially leading to more or different types of complications. However, without additional context or information on the nature of the fractures, the groups (A, B, and A+B), and the specific complications, it's difficult to draw more detailed conclusions or understand the implications fully. Further analysis and clinical insight would be necessary to interpret these findings accurately.
Table 5. Distribution of patients according to abstinence period and IIEF5 score
|
IIEF5 : 5-10 |
IIEF5 : 11-15 |
IIEF5 : 16-20 |
Total |
|
|
< 1 month |
5 |
1 |
1 |
6 |
|
1-2 months |
1 |
0 |
2 |
3 |
|
> 2 months |
0 |
0 |
2 |
2 |
|
Total |
6 |
1 |
5 |
11 |
|
Ki(2)* = 10,73 ; p < 0,05 |
||||
The USP score of the patients who had a urethral rupture did not indicate dysuria, and the retrograde urethrogram was normal at the 6th month for the 3 patients, this is explained by the fact that the rupture of the urethra in the 3 patients was minimal, involving no more than a third of the urethra.
DISCUSSION The penis benefits from inherent defenses in its mobility, yet it becomes vulnerable to injury during erection due to substantial increases in intracavernous pressure, surpassing the tensile strength of the tunica albuginea under sudden, acute loading. While the tunica albuginea measures 2 mm in thickness in the flaccid state, it decreases to 0.25–0.5 mm during erection [1]. Penile fracture stands out as a dramatic consequence of blunt trauma when the penis is erect [2].
Several authors have observed a significant incidence of cavernous body fractures associated with forced maneuvers of an erect penis, particularly in Maghreb and Eastern countries [3-5]. However, the occurrence is not uncommon in cases of coitus misstep [6], as seen in our series. This trend can be attributed to the relatively young age of our study population, with an average age of 39,74 years, and the majority being married, indicating active sexual engagement. For patients who reported a forced maneuver to deal with a bothering erection, manipulating the erect penis is a commun and harmless way to resolve the erection, according to them, until the fracture happens. De Rose et al. [7] proposed that repeatedly bending the erect penis to facilitate detumescence in inappropriate circumstances might, over time, induce structural abnormalities that compromise the mechanical integrity of the tunica, rendering it less resistant to expansion.
Among the mechanisms of interrupted coitus, the doggy position was the most predominant, followed by the Andromachus position, aligning with findings reported by some authors [8,9]. This phenomenon can be explained by the dynamics of sexual intercourse. When the man is in a dominant position and highly aroused, the sexual activity can become particularly vigorous. This intensity may lead to a more forceful impact when the penis slides out of the vagina, striking against the perineum or pubic symphysis. Additionally, when the woman is on top, if the erect penis inadvertently slips out of the vagina, the entire weight of the woman may unintentionally land on the penis, contributing to the risk of fractures.
Information obtained from the patients' medical history and physical examination remains crucial for accurate diagnosis, as a sudden cracking sound is often reported, followed by pain, rapid loss of erection, swelling, and penile deformity [7,10]. In our cases, surgical repair was performed, and a tear in the tunica albuginea was consistently found upon evacuation of the hematoma, even when ultrasound results were negative in some instances. The location of the tear correlated with the direction of penile deviation away from the tear site and was confirmed intraoperatively in the majority of cases, consistent with findings from previous studies [11-13].
While clinical history and genital examination are acknowledged as the primary methods for diagnosis, there is no unanimous agreement on the optimal approach to rule out a concurrent urethral lesion, which may be present in nearly a third of cases. The approach to using transurethral catheters varies among researchers. In a retrospective review by Al Ansari involving 114 cases, it was found that in 70 patients with low preoperative suspicion for urethral injury, a 16 Fr catheter was inserted before repair and then removed 6 hours after surgery [14]. Gamal's series of 51 patients, where urethral injury repair was performed, saw catheters remaining in place for 1 week following the procedure [15]. Hatzichristodoulou placed catheters in 18 of 25 patients with confirmed penile fracture if swelling was severe or if the tunical tear was close to the urethra, leaving them in place for 3 days after repair. For seven patients with concomitant urethral injury, catheters were kept in for 14 days [16]. Zargooshi advocates against routine catheterization in penile fracture cases unless the tunical injury is near the urethra or extends ventrally with undefined margins [17]. The duration of catheterization is primarily decided by the surgeon's discretion, as there is no standardized approach. Interestingly, patients undergoing simultaneous urethral injury repair tended to have longer catheter durations compared to those without urethral injury.
In our study, no correlation was observed between sexual position and the severity of penile injury, consistent with findings in a meta-analysis that did not identify a significant impact on relative risk [3]. The diagnosis of penile fracture primarily relies on clinical evaluation, incorporating the stereotypical account of the incident and physical examination. In typical cases, no additional diagnostic tests are deemed necessary [18-20]. Nevertheless, for atypical or delayed presentations, some authors suggest the use of Color Doppler ultrasound, retrograde urethrocystography, cavernography, or MRI [19-21]. Ultrasonography plays a crucial role in identifying hematoma and potential bleeders, which may indicate the need for penile exploration. However, in our study, tunical tears were only visualized by ultrasonography in 45 out of 63 cases (71,4%). This relatively low detection rate could be attributed to its operator-dependent nature and reliance on the examiner's experience, as well as the extent of hematoma. Therefore, while ultrasonography can be helpful, history taking and physical examination remain reliable methods and may even be superior to ultrasonography in diagnosing penile fracture. Retrograde urethrocystography is specifically indicated in cases of associated urethral rupture.
MRI provides a detailed evaluation of the location and extent of the rupture of the albuginea of the cavernous body, along with associated lesions like a rupture of the spongy body or urethra [22]. In our specific case, we did not use MRI due to it’s unavailability in urgent situations and the use of ultrasonography was limited to diagnostic uncertainties.
Experts generally agree that immediate repair yields the quickest recovery of erectile function and the most satisfactory cosmetic outcome. Research by Al Ansari et al. showed that 4.1% of patients who underwent immediate repair developed erectile dysfunction, compared to 18.2% in those who had delayed surgical intervention [23]. Delayed repair, occurring 1 to 7 days post-injury, was associated with a higher incidence of erectile dyscfunction. Kozacioglu et al. categorized penile fracture cases based on the hours elapsed from injury to surgical repair and found no significant differences in outcomes between groups. Their findings suggest that patients with penile fracture do not necessarily require immediate surgery, as long as repair occurs within 24 hours [24].
Two commonly employed incision techniques in the repair of penile fracture are the distal circumcising-degloving and vertical penoscrotal approaches. The sub-coronal, distal degloving incision is the most popular technique reported for repairing penile fracture [25-27], it was predominantly employed in our study. This approach offers advantages such as full inspection of the corporal body, facilitating the detection of contralateral corporal body or urethral injuries, and aiding in easier repair [26]. Additionally, this technique typically results in the most natural cosmetic outcome [15].
Nevertheless, some authors highlight the potential risks associated with the coronal approach for penis fracture, including the possibility of edema, infection, and skin necrosis [28]. It is noteworthy that in our study, there were no reported cases of infection or edema of the penis. This positive outcome may be attributed to the administration of antiedematous measures and antibiotics to all our patients. Certain authors propose that a lateral and longitudinal incision in front of one of the cavernous bodies provides an elective approach to the fracture site without posing a risk to the skin. However, it is acknowledged that this approach may result in an unsightly scar [6].
All tears were repaired using absorbable continuous sutures with an inverted knot, aligning with the preference of most authors and contrasting with others who prefer nonabsorbable interrupted sutures [11,16, 29-32]. The use of absorbable sutures appears to offer advantages in postoperative outcomes. Conversely, nonabsorbable sutures have disadvantages such as stitch sinus, foreign body granuloma at the suture site, and discomfort during sexual activity [33]. In our study, we observed a short- and long-term complication rate of 21,96%, with a prevalence of discomfort during sexual intercourse and erectile dysfunction, similar to findings reported by many authors [3]. Complications subsequent to penile fracture repair encompass pain during erection and intercourse, wound infection, wound edema, skin necrosis, and wound dehiscence. In a meta-analysis by Amer et al., involving 22 studies with 584 surgical patients and 81 nonsurgical patients, an overall complication rate of 20.6% and 46.4%, respectively, was reported. Among surgically treated patients, prevalent complications included penile plaques/nodules (13.7%), curvature (2.7%), and erectile dysfunction (1.9%). Conversely, nonsurgically managed patients commonly experienced erectile dysfunction (22%), plaques/nodules (19%), and curvature (13%) [34]. Additionally, Penbegul et al. assessed the long-term psychological status of surgically treated penile fracture patients, revealing that immediate repair did not elevate the incidence of depression, anxiety, or psychogenic sexual dysfunction [35].
The frequency of complications in our series could be attributed to non-compliance with the recommended post-operative abstinence period in some cases, as we identified a correlation between the duration of abstinence and the occurrence of complications (p < 0.05). The observed erectile dysfunction following penile fracture seems to be more associated with a venous cause (leakage of venous blood into the spongy body) rather than an arterial cause related to cavernous artery failure. However, the origin of this dysfunction in our series remains unknown, as we did not resort to echo-Doppler to investigate its etiology.
In our series, we identified a correlation between the length of the fracture line and the occurrence of short- and long-term complications (p < 0.05). We hypothesize that the size of the fracture line may lead to significant fibrosis of the albuginea, causing curvature, and substantial leakage of cavernous venous blood into the spongy tissue, contributing to erectile dysfunction. It's important to acknowledge the subjectivity of questionnaire responses as a potential bias in the assessment of sexual function in our patients.
CONCLUSION
In conclusion, our study highlights the critical nature of penile fractures, often resulting from forced maneuvers during an erect state or sexual activity. Delayed or inadequate management can lead to functional and aesthetic complications, as observed in 21.96% of cases in our study. There is a notable correlation between the duration of sexual abstinence and the extent of the fracture line, emphasizing potential risk factors that clinicians should consider. Immediate exploration and repair of the tunica albuginea have traditionally been the standard approach, yielding favorable cosmetic and functional outcomes when promptly addressed. However, inconsistent terminology surrounding surgical intervention has led to diverse practices across surgeons and medical facilities, suggesting a need for standardized terminology and improved multidisciplinary collaboration in managing these urological emergencies.
HIGHLIGHTS
- Penile fracture represents a critical urological emergency, often resulting from forced maneuvers during an erect state or sexual activity.
- The diagnosis of penile fracture primarily relies on clinical evaluation, incorporating the stereotypical account of the incident and physical examination. No additional diagnostic tests are necessary.
- There is a correlation between the occurrence of complications and the duration of sexual abstinence.
- No causal link was found between the type of thread used for suture, the type of coitus misstep, and the incidence of complications.
REFERENCES
- Miller S, McAninch JW. (1996). Penile fracture and soft tissue injury. In: McAninch JW, ed. Traumatic and reconstructive urology, ch. 59. Philadelphia, PA: WB Saunders. pp. 693-698.
- Penson DF, Seftel AD, Krane RJ, Frohrib D, Goldstein I. (1992). The hemodynamic pathophysiology of impotence following blunt trauma to the erect penis. J Urol. 148:1171-1180.
- Amer T, Wilson R, Chlosta P, AlBuheissi S, Qazi H, Fraser M, Aboumarzouk OM. (2016). Penile Fracture: A Meta-Analysis. Urol Int. 96(3):315-329.
- el-Sherif AE, Dauleh M, Allowneh N, Vijayan P. (1991). Management of fracture of the penis in Qatar. Br J Urol. 68(6):622-625.
- Zargooshi J. (2000). Penile fracture in Kermanshah, Iran: report of 172 cases. J Urol. 164(2):364-366.
- Padja E, Bahri A, Tayiri A, Chafi ki J, Janane A. (2016). Surgical treatment of rod fractures: Surgical treatment of yard fractures: Surgical treatment of 24 cases. Uro’Andro. 1:251-255.
- Nicolaisen GS, Melamud A, Williams RD, McAninch JW. (1983). Rupture of the corpus cavernosum: Surgical management. J Urol. 130(5):917-919.
- Barros R, Schulze L, Ornellas AA, Koifman L, Favorito LA. (2017). Relationship between sexual position and severity of penile fracture. Int J Impot Res. 29(5):207-209.
- Gayito Adagba RA. (2020). Outpatient treatment of yard fractures at the University Hospital of Lomé. Prog Urol. 30(10):507-513.
- Hinev A. (2000). Fracture of the penis: Treatment and complications. Acta Med Okayama. 54(5):211-216.
- Zargooshi J. (2000). Penile fracture in Kermanshah, Iran: Report of 172 cases. J Urol. 164(2):364-366.
- Fergany AF, Angermeier KW, Montague DK. (1999). Review of Cleveland Clinic experience with penile fracture. Urology. 54(2):352-355.
- Mydlo TH, Gershbein AB, Macchia RJ. (2001). Nonoperative treatment of patients with presumed penile fracture. J Urol. 165:424-425.
- Al Ansari A, Talib RA, Shamsodini A, Hayati A, Canguven O, Al Naimi A. (2013). Which is guilty in self-induced penile fractures: marital status, culture or geographic region? A case series and literature review. Int J Impot Res. 25(6):221-223.
- Agarwal MM, Singh SK, Sharma DK, Ranjan P, Kumar S, Chandramohan V, et al. (2009). Fracture of the penis: a radiological or clinical diagnosis? A case series and literature review. Can J Urol. 16:4568-4575.
- Hatzichristodoulou G, Dorstewitz A, Gschwend JE, Herkommer K, Zantl N. (2013). Surgical management of penile fracture and long-term outcome on erectile function and voiding. J Sex Med. 10(5):1424-1430.
- Zargooshi J. (2009). Sexual function and tunica albuginea wound healing following penile fracture: An 18-year follow-up study of 352 patients from Kermanshah, Iran. J Sex Med. 6(4):1141-1150.
- Mensah JE, Morton B, Kyei M. (2010). Early surgical repair of penile fractures. Ghana Med J. 44(3):119-122.
- Sylla C, Diallo AB, Fall PA, Gueye SM, Ndoye A, Thiam OB, Ba M, Diagne BA. (2000). Penis fracture: About 12 cases. Andrology. 10(4):407-411.
- Yamaçake KG, Tavares A, Padovani GP, Guglielmetti GB, Cury J, Srougi M. (2013). Long-term Treatment Outcomes Between Surgical Correction and Conservative Management for Penile Fracture: Retrospective Analysis. Korean J Urol. 54(7):472-476.
- Palliyagiru KH, Suvendran S, Abeygunasekera AM. (2014). A case of penile fracture caused by self manipulation to achieve detumescence. The Sri Lanka Journal of Surgery. 32(1):36-38.
- Swain FR, Udeschi M, Armm MF, Gagliardi JA. (2015). Fracture of the Penis: Demonstration by MRI with Surgical Correlation. Radiol Case Rep. 2(3):75.
- Yapanoglu T, Aksoy Y, Adanur S, Kabadayi B, Ozturk G, Ozbey I. (2009). Seventeen years' experience of penile fracture: conservative vs. surgical treatment. J Sex Med. 6(7):2058-2063.
- Kozacıoğlu Z, Ceylan Y, Aydoğdu Ö, Bolat D, Günlüsoy B, Minareci S. (2017). An update of Penile Fractures: Long-term significance of the number of hours elapsed till surgical repair on long-term outcomes. Turk J Urol. 43(1):25-29.
- El-Assmy A, El-Tholoth HS, Abou-El-Ghar ME, Mohsen T, Ibrahiem EH. (2012). Risk factors of erectile dysfunction and penile vascular changes after surgical repair of penile fracture. Int J Impot Res. 24(1):20-25.
- Gedik A, Kayan D, Yamiş S, Yılmaz Y, Bircan K. (2011). The diagnosis and treatment of penile fracture: our 19-year experience. Ulus Travma Acil Cerrahi Derg. 17(1):57-60.
- Hatzichristodoulou G, Dorstewitz A, Gschwend JE, Herkommer K, Zantl N. (2013). Surgical management of penile fracture and long-term outcome on erectile function and voiding. J Sex Med. 10:1424-1430.
- Eke N, Elenwo SN. (1990). Penile fracture from attempted rape. Orient Journal of Medicine. 11:37-38.
- Pandyan GV, Zaharani AB, Al Rashid M. (2006). Fracture penis: An analysis of 26 cases. Scientific World Journal. 6:2327-2333.
- Uygur MC, Gulerkaya B, Altug U, Germiyanoglu C, Erol D. (1997). 13 years’ experience of penile fracture. Scand J Urol Nephrol. 31(3):265-266.
- Wessells H, Long L. (2006). Penile and genital injuries. Urol Clin North Am. 33(1):117-126.
- El-Bahnasawy MS, Gomha MA. (2000). Penile fractures: the successful outcome of immediate surgical intervention. Int J Impot Res. 12(5):273-277.
- Kattan S, Youssef A, Onuora V, Patil M. (1993). Recurrent ipsilateral fracture of the penis. Injury. 24(10):685-686.
- Bolat MS, Özen M, Önem K, Açıkgöz A, Asci R. (2017). Effects of penile fracture and its surgical treatment on psychosocial and sexual function. Int J Impot Res. 29(6):244-249.
- Penbegul N, Bez Y, Atar M, Bozkurt Y, Sancaktutar AA, Soylemez H, et al. (2012). No evidence of depression, anxiety, and sexual dysfunction following penile fracture. Int J Impot Res. 24(1):26-30.
- Alafifi M, Mostapha AE, Dibingue C, Moataz A, Dakir M, Debbagh A, et al. (2022). Penile Tri-Tubular Fracture: A Case of Partial Urethral Ruptur with Bilateral Corpora Cavernosa Fractures. J Urol Nephrol. 7(1):000200.
- Mathew G, Sohrabi C, Franchi T, Nicola M, Kerwan A, Agha R, et al. (2023). Preferred Reporting Of Case Series in Surgery (PROCESS) 2023 guidelines. Int J Surg. 109(12):3760-3769.