Previous Issues Volume 1, Issue 1 - 2017
A Complex Clinical Case with Retroperitoneal Fibrosis
Selçuk Sarıkaya1 , Rıdvan Özbek2,Cagri Senocak2,Ömer Faruk Bozkurt2
Corresponding Author: Selcuk Sarikaya, Gulhane Research and Training Hospital, Department of Urology, General Tevfik Saglam Caddesi, Etlik – Ankara / Turkey, Tel: +905316274819; Email:[email protected]
Received Date: 21 Aug 2017 Accepted Date: 22 Aug 2017 Published Date: 25 Aug 2017
Copyright © 2017 Sarikaya S
Citation:Sarikaya S, Özbek R,Senocak C and Bozkurt ÖF.(2017). A Complex Clinical Case with Retroperitoneal Fibrosis. Mathews J Urol Nephrol 1(1): 001.
INTRODUCTION
Retroperitoneal fibrosis (RP) is an inflammatory tissue reaction characterized with fibrosis in the the retroperitoneum [1].There are different diagnostic radiologic studies used for the diagnosis of RP [2]. The disease is also called 'Ormond disease [3]. In this study, we aimed to present the patient that was admitted to our clinic with bilateral hidronephrosis and diagnosed as retroperitoneal fibrosis, the surgical treatment of disease and persistent clinical situation.
CASE REPORT
54 year-old male patient admitted to emergency service with bilateral flank pain, nausea and vomiting. According to ultrasonography there was bilateral hydronephrosis. Creatine level increased and the patient was consulted to our clinic. Creatinine level was 6.2mg/dl and there was oliguria. Ultrasonography revealed right pelvicalyceal grade 3 hydronephrosis, and left pelvicalyceal grade 1 hydronephrosis. Computerised tomography was normal. Magnetic resonance revealed hypointense soft tissue formation compatible with retroperitoneal fibrosis that was in midline of abdomen and started form truncus choliacus and extended to iliac bifurcation level and through paraaortic and left pararenal space. Bilateral double J catheterization and steroid treatment was given. (Figure 1)
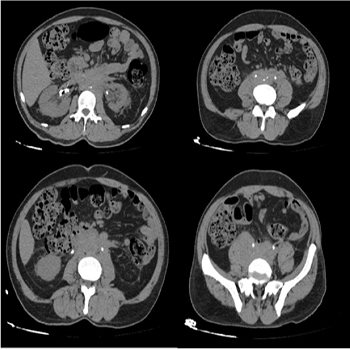
Figure 1:Computerised tomography(CT), fibrotic inflammation.
In early postoperative period, creatinine level decreased to 2.1 mg/dl. In the following period, bilateral uretherolysis operation was performedin another clinic due to the increased creatinin levels and persistent bilateral hydronephrosis according to ultrasonography. On postoperative 6th month, patient admitted to our clinic again with bilateral flank pain and ultrasonography revealed right grade 3 hydronephrosis and left grade 1 hydronephrosis. After that we performed bilateral uretheral double J catheterization. But due to the persistent right hydronephrosis nephrostomy catheter was inserted On postoperative 3rd month Escherichia Coli was detected in urine culture and appropriate antibiotherapy was given. After treatment rightnephrostomy and left DJ catheter was removed and right metalic DJ catheterization was performed. On postoperative 3rd month creatinine level was 1.4 mg/dl. There wasn't any urinary tract infection periodic dj catheter exchange operations planned for the patient
DISCUSSION
Retroperitoneal fibrosis, is a progressive clinical situation caused by inflammatory and fibrotic reaction in retroperitoneum that pushes üreter the and create mass effect to retroperitoneal structures like ureter [4]. Firstly, medical treatment and endoscopic or percutaneous decompression options would be considered as treatment options. For the cases that medical therapy failed, open or laparoscopic surgical treatment would be prefered. Despite to medical and surgical treatments, clinical situation would be unfortunately seen as persistent and resistant.
REFERENCES
- Zhou HJ, Yan Y, Zhou B, Lan TF, et al. (2015). Retroperitoneal fibrosis: a retrospective clinical data analysis of 30 patients in a 10-year period. Clin Med J. 128(6): 804-810.
- Van der Bilt FE, Hendriksz TR, Van der Meijden WA, Brilman LG, et al. (2016). Outcome in patients with idiopathic retroperitoneal fibrosis treated with corticosteroid or tamoxifen monotherapy. Clin Kidney J. 9(2): 184-191.
- Cristian S, Cristian M, Cristian P, Constantin G, et al. (2015). Management of idiopathic retroperitoneal fibrosis from the urologist's perspective. Ther Adv Urol. 7(2):85-99.
- Khalil F, Ouslim H, Mhanna T and Barki A. (2015). Extensive primary retroperitoneal fibrosis (Ormond's disease) with common bile duct and ureteral obstruction: A rare case report. Int J Surg Case Rep. 13: 5-7.