Previous Issues Volume 1, Issue 2 - 2016
Providing In-Between Meals During Dialysis Treatment Contributes to an Adequate Protein And Energy Intake in Hemodialysis Patients: A Non-Randomized Intervention Study
Geertrude I Struijk-Wielinga1, Marieke Romijn2, Floor Neelemaat1, Piet M ter Wee2, Peter JM Weijs1,3
1Department of Nutrition and Dietetics, Internal Medicine, VU University Medical Center, Amsterdam, Netherlands.
2Department of Nephrology, VU University Medical Center, Amsterdam, Netherlands.
3School of Sports and Nutrition, Amsterdam University of Applied Sciences, Amsterdam, Netherlands.
Corresponding Author:Geertrude I. Struijk-Wielinga, RD, Department of Dietetic and Nutrition, Internal Medicine, VU University Medical Center, De Boelelaan 1117, 1081HV Amsterdam, Netherlands,Tel: 0031 20 4441997; E-Mail:[email protected]
Received Date: 08 Jun 2016 Accepted Date: 27 Jun 2016 Published Date: 08 Jul 2016
Copyright © 2016 Struijk-Wielinga GI
Citation:Struijk-Wielinga GI, Romijn M, Neelemaat F, ter Wee PM, et al. (2016). Providing In-Between Meals During Dialysis Treatment Contributes to an Adequate Protein And Energy Intake in Hemodialysis Patients: A Non-Randomized Intervention Study. Mathews J Nutr Diet. 1(2): 006.
ABSTRACT
Reduced protein intake, imbalance between protein synthesis and degradation during hemodialysis treatment are causes of protein-energy wasting. The latter predicts morbidity and mortality in these patients. This study aimed to achieve adequate protein and energy intake on dialysis days. During a six week intervention period all consenting adult chronic hemodialysis patients in an outpatient dialysis clinic an in-between meal were offered. At start protein and energy requirements were calculated, nutritional status determined. 24-hour dietary recall was completed for two dialysis days pre and post-intervention. In 23 patients protein intake increased from 1.0 ± 0.5 g/kg to 1.2 ± 0.5 g/kg (p = 0.002) and energy intake increased from 25 ± 10 kcal/kg (85 % of the energy requirement) to 29 ± 10 kcal/kg (95%) (p = 0.051). At least 90% of their protein requirement was achieved in 35% of the patients before versus 61% after intervention. At least 90% of their energy requirements was achieved in 44% of the patients versus 57% after intervention. Protein and energy intake on days of dialysis treatment is adequate in only one out of three patients. In-between meals improved adequate protein and energy intake to two out of three patients.
KEYWORDS
Hemodialysis; Protein Energy Wasting; Malnutrition, In-Between Meal; Protein, Energy.
INTRODUCTION
Worldwide approximately two million people suffer from chronic kidney disease (CKD). Protein energy wasting (PEW) is common in CKD patients and is associated with high morbidity and mortality, especially in patients receiving maintenance dialysis therapy. PEW is present in 18-75% of the patients and characterized by reduced protein- and energy stores in the body [1, 2]. The negative consequences are numerous, such as an increase in frequency and severity of complications caused by reduced immunological defense, impaired wound healing, a reduced recovery from illnesses, impaired quality of life and reduced muscle mass with a decrease of the overall condition resulting in a fourfold increased risk on mortality [3]. The cause of PEW is multifactorial. Acidosis, the dialysis procedure itself and loss of amino acids during dialysis are factors contributing to the development of PEW with persistent inflammation. The latter contributes to anorexia as in most studies spontaneous intake of protein has been reduced to less than 1.0 g/kg/day [4-6]. Nutritional therapy for dialysis patients focuses on maintaining or improving the nutritional status by advising small protein meals and nutrition supplements, tube feeding or intradialytic feeding (added parenteral nutrition which is provided during dialysis). Beside providing food or nutrition supplements during hemodialysis treatment seems to be important. It increases skeletal muscle protein synthesis, reduces catabolism and improves protein balance [7]. A pilot study in 2011 at the VU University Medical Center, showed that hemodialysis patients had on average a deficiency of 15 grams of protein and 240 kcal per day over a period of three consecutive days (two days of dialysis and one non dialysis-day) (Table 1) [8]. Our patients were encouraged to eat during dialysis, but most of the food being provided was low in protein. Based on these results we posed the question whether protein and energy intake of hemodialysis patients during dialysis days could be improved by providing high protein and energy in-between meals during the dialysis treatment.
Table 1: Protein- and energy intake on dialysis days and non dialysis days (n = 24).
| Requirements | Intake on dialysis days | Percentage of requirements | Intake on non-dialysis days | Percentage of requirements | |
|---|---|---|---|---|---|
| Protein/gram | 83 ± 13 | 72±19 | 87 | 65 ± 29 | 78 |
| Energy/kcal | 1878 ± 244 | 1786 ± 486* | 95 | 1570 ± 609* | 84 |
The values are presented as mean ± SD. * Significant difference dialysis days compared with non dialysis days
METHODS
Patients
The intervention study was conducted from September to December 2012 in an outpatient hemodialysis center. All Dutch and English speaking chronic hemodialysis patients older than 18 years who dialyzed at least twice a week with a minimum life expectancy of three months were included. Patients with acute renal failure, dementia and patients who were transplanted during the study period were excluded. Patients gave informed consent according to the Helsinki II declaration.
Procedure
At baseline patient data were recorded from the digital medical file: age, gender, ethnicity, duration of dialysis (months), dialysis time per week, residual diuresis (maximum two months ago), co-morbidity, height, weight after dialysis (weight at the start of the study and six months earlier) and laboratory data (maximum two weeks old). One to two weeks before the start of the study energy requirements were determined, protein requirements calculated, and the nutritional status determined by Subjective Global Assessment (SGA), according to the Dutch standard. Mean systolic and diastolic blood pressure were recorded 4 weeks prior and during the study, as well as the number of hypotensive episodes. A hypotensive episode was defined as blood pressure beneath 90/60 mmHg, with clinical symptoms such as dizziness, cramps or loss of consciousness. At baseline and after six weeks handgrip strength, body weight after dialysis, 24-hour dietary recall, appetite and serum phosphate were measured.
Intervention / High Protein In-Between Meal
Patients were advised by dietitians (trainees) to eat a high protein and energy in-between meal for a period of six weeks during every dialysis treatment with a variation of about 15-18 grams of protein and 86-279 kcal. Patients were eating this extra in-between meal as well as the regular meal and snack that was already provided to all patients. A choice out of seven extra in-between meals was made including cheese (prepared with vegetable oil), chicken nuggets, unsalted peanuts, candy bar, Greek low fat yoghurt or two oral supplements and were provided by the nutrition assistant. Every patient's preference was checked in order to determine which in-between meal was appreciated best. After the intervention the increase or decrease in protein and energy intake per dialysis day per patient was calculated.
Intervention / Education on Protein, Energy and Phosphate
In the first week, patients were informed about adequate protein and energy intake in order to reduce the risk of developing PEW, during the dialysis treatment. This information was supported by three posters. Poster one provided information on what protein is, why protein requirements increase in hemodialysis patients, how much protein is adequate for a body weight and what happens when patients consume adequate or inadequate amounts of protein. Information about phosphate was also provided. A higher protein intake will result in a higher intake of phosphate, which will lead to a higher serum phosphate level. This can be reduced by the use of phosphate-binding medication. The second poster gave an overview of the various possibilities of high protein and energy in-between meals, with per in-between meal the amount of phosphate. Poster three focused on the situation at home and contained tips for meals including lunch, dinner and inbetween meals to provide optimal protein intake.
Protein and Energy Intake
The protein and energy intake of hemodialysis patients were estimated using a 24-hour dietary recall method by two previously trained dietitian trainees. During dialysis patients were asked what kind and which amounts of food and drinks they consumed from midnight until the moment of the 24-hour recall was taken. Patients were contacted by telephone the day after (on a non-dialysis day) for completing the intake of the dialysis day. Household sizes were calculated into grams, the nutrients were coded using the NEVO codes version 2011/3.0 [9]. Patients mean protein and energy intake were calculated using Microsoft Access 2010.
Protein and Energy Requirements
The protein requirement of all hemodialysis patients was established at 1.2 grams of protein per kilogram of current body weight [10, 11]. To prevent overestimation protein requirements in obese patients (BMI > 27 kg/m2), a BMI of 27 kg/m2 was used [11]. A patient achieved his/her protein and energy intake when a minimum of 90% of the requirements was consumed. Total energy requirement of the patient was determined by measuring resting energy expenditure (REE) plus the physical activity level (PAL). The REE per patient was measured using indirect calorimetry (Vmax Encore 29, Viasys Healthcare, CA, USA) two weeks before the start of the intervention. Measurement conditions were semi-standardized conditions that comply with indirect calorimetry measurements in clinical practice. Patients had no feeding or smoking at least three hours before the measurement, and had not been physically active. Measurements were performed in standard neutral dialysis ward room temperature, the patient was in supine position and awake. During dialysis a canopy was placed over the head of the patient. Oxygen consumption (VO2) and carbon dioxide (VCO2) was measured and energy expenditure was calculated by the formula of Weir [12]. Acceptable coefficient of variation was 10%. The measurements took place for at least 30 minutes. The REE of every patient was also estimated using the Harris and Benedict formula 1984 [13]. Measured REE was obtained in 21 patients. On a group level, the mean estimated REE showed no bias compared to measured REE. Since some patients were without measured REE, we have used the estimated REE levels for both consistency (all patients) and practical (used in clinical practice) reasons." Patients were asked which activities (per hour) they performed on a dialysis day in order to estimate the PAL.
Body Weight
Body weight after the dialysis treatment was assessed with indoor clothes and shoes on an electronic scale (Soehnle S20 2763, Weegtechniek Holland BV, Zeewolde, the Netherlands).
Appetite
The appetite of the patients was asked by the dietitian during the 24 hour recall at baseline and after 6 weeks. A score between zero and ten was given on a Visual Analogue Scale (VAS). A score of zero represented a very bad appetite and score of ten a very good appetite [14].
Nutritional Status
The Subjective Global Assessment was used to estimate the nutritional status. This SGA included a questionnaire on weight progress, nutritional intake, gastrointestinal symptoms such as anorexia, vomiting and diarrhea, and a physical examination for a subjective evaluation of muscle atrophy and a decrease in subcutaneous adipose tissue. Patients could score between 1 to 7 points, and were categorized into severely malnourished (score 1 and 2), mild to moderately malnourished (score 3, 4, and 5), and well nourished (score 6 and 7) [15]. Because of the small number, the patients were classified malnourished (SGA score 1 to 5) or well nourished (SGA score 6 and 7).
Handgrip Strength
During dialysis maximum handgrip strength (kg) was measured twice with a hydraulic hand grip strength meter (Baseline, Fabrication Enterprises Inc., Irvington, USA, NY) at the shunt-free (usually dominant) arm. This method was chosen to prevent complications to the shunt. Patients were measured on the same arm at both time moments. The test was performed in a sitting position under standardized conditions [16]. Patients were instructed to perform a maximum isometric grip strength with an interval of 30 seconds between the measurements. The maximum grip strength was determined with an accuracy of 0.5 kg. The highest value was used.
Phosphate
To analyze the effect of the intervention on the serum phosphate level of the patients, serum phosphate was measured. Serum phosphate levels were compared to the reference values from the "Guideline diet for hemodialysis 2011" [11].
Statistics
Statistical analyzes were performed only in patients with measurements available at baseline and at the end of the study. Descriptive statistics were used to determine means, standard deviations, percentages, minimum and maximum and changes in variables. A confidence interval of 95% was used to calculate the differences in percentages and means. A paired T-test with a significance of 0.05 was performed in order to show differences between the baseline measurement and the measurement at the end of the study. All collected data were analyzed using SPSS 20.0 (SPSS, Chicago, IL, USA).
RESULTS
At the time of this study 43 hemodialysis patients underwent dialysis treatment in the VU University Medical Center. Fifteen patients were excluded due to refusal to participate (n = 8), suffering from dementia (n = 4), not speaking Dutch/English language (n = 1), dialysis treatment < 2 times a week (n = 1) and life expectancy < 3 months (n = 1). So in total 28 were included. Data of 23 patient were analyzed since 5 patients were lost to follow-up during the intervention; one patient died, one patient had to stop because of a severely decreased physical condition, one patient was transplanted and two patients refused to cooperate with the final measurement of the 24-hour recall. Classification in nutritional status showed that 5 of the 23 remaining patients were malnourished (SGA score 4 and 5) and 18 patients were well-nourished. In the malnourished group the score was given mainly based on muscle atrophy and inadequate protein and energy intake and not based on loss of body weight. Table 2 shows the patient characteristics. At baseline there were no differences between the malnourished and the well-nourished group.
Table 2: Patient characteristics
| Demographic and clinical characteristics | Total n = 23 | Malnourished n = 5 | Well-nourished n = 18 |
|---|---|---|---|
| Age in years | 55.4 ± 12.7 | 65.9 ± 5.5 | 52.5 ± 12.6 |
| Gender (men/women) | 11 / 12 | 3 / 2 | 8 / 10 |
| Caucasian Negroid Asian North-African | 13 3 4 3 | 3 1 1 0 | 10 2 3 3 |
| Dialysis duration in months (median and range) | 35 (15-142) | 26 (15-109) | 35 (16-142) |
| Dialysis hours p/w | 12.0 ±1.6 | 13.2 ±1.8 | 11.6 ±1.5 |
| Residual diuresis yes/no | 13 / 10 | 3 / 2 | 10 / 8 |
| Comorbidity Diabetes mellitus Cardio vascular diseases Left ventricle dysfunction Peripheral vascular disease Oncological diseases Other pathological like gastro intestinal, system diseases, hepatitis C, tetra parese | 6 6 3 5 3 8 | 2 2 1 2 2 2 | 4 4 2 3 1 6 |
| Height (m) Body weight (kg) BMI(kg/m) Appetite (Vas scale 1-10) Handgrip strength (kg) Serumphosphate (mmol/l) | 1.70 ±0.11 70.8 ±14.2 24.5 ±4.4 7 ±1 28.7 ±10.4 1.93 ±0.80 | 1.72 ±0.12 72.8 ±14.7 24.7 ±3.6 7 ±1 30.0 ±13.3 1.35 ±0.41 | 1.69 ±0.10 70.2 ±14.4 24.4 ±4.6 7 ±1 28.2 ±10.0 2.09 ±0.82 |
In-Between Meals
The use of a high protein and energy in-between meal on days of dialysis treatment resulted in an average increase of 12 (0- 39) grams of protein and 175 (0-370) kcal per patient per dialysis day. On average, two in-between meals were consumed per week. Cheese (prepared with vegetable oil), chicken nuggets and peanuts were the favorite choice. One out of 10 patients did not consume an extra in-between meal.
Protein Intake
Protein intake increased significantly during the intervention from 1.0 ± 0.5 g/kg to 1.2 ±0.5 g/kg (p = 0.002). At baseline, 35% of the patients reached the minimal target of 90% of their protein requirement and after the intervention 61% of the patients. In the malnourished group protein intake increased from 0.8 ±0.4 g/kg to 1.3 ±0.5 g/kg (p = 0.033) and in the well-nourished group from 1.0 ±0.5 g/kg to 1.2 ±0.5 g/kg (p=0.041). Protein intake increased with an average of 18 ±25 grams of protein per day. After six weeks the protein intake in the malnourished group increased with 38 ±32 g/d (p=0.057, Table 3) versus 12 ±20 g/d in the well-nourished group (p= 0.019). The malnourished group reached an average of 68 ±27 % of the protein requirement (p = 0.05) versus 86 ±39% (p=0.03) in the well- nourished group.
Energy Requirements and Energy Intake on Days of Dialysis
During the intervention, the mean energy intake increased from 25 ±10 kcal/kg to 29 ±11 kcal/kg (p = 0.051). At least 90% of their energy requirements was achieved in 44% of the patients before and in 57% after the intervention. Energy intake increased with an average of 264 ±555 kcal. During the intervention, the average energy intake of the malnourished group increased from 20 ±9 kcal/kg to 30 ±11 kcal/ kg (p = 0.053). During the intervention, the average energy intake of the well-nourished group increased from 26 ±10 kcal/kg to 29 ±11 kcal/kg (p = 0.315 Figure 1). In the malnourished group the average energy intake on dialysis days increased with 716 (-26-1981) kcal (p = 0.06) versus 139(-565-1450) kcal (p = 0.2, Table 3) in the well-nourished group. Figure 2 shows the relative improvement in energy intake during dialysis days.
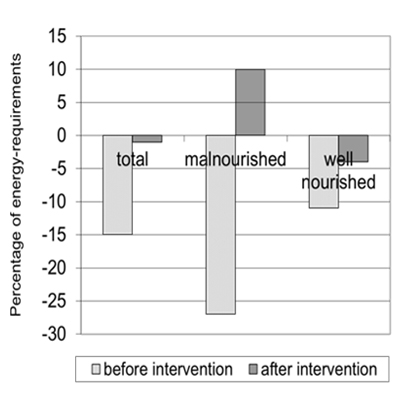
Figure 1: Energy intake as percentage (%) of energy requirements, before and after intervention of the total group (n = 23), the malnourished group (n = 5), the well nourished group (n = 18).
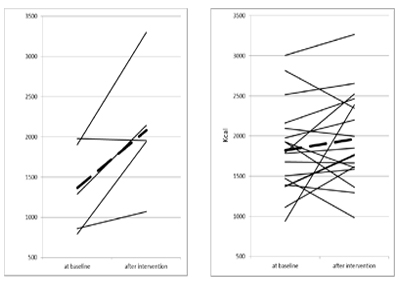
Figure 2: Energy intake (kcal) per patient at baseline and after the intervention in the malnourished group (left figure, n = 5) and the well nourished group (right figure, n = 18). The straight line indicates the mean.
Blood Pressure an Hypotensive Episodes
Mean systolic and diastolic blood pressure before start of the study were 149 ±17 and 82 ±12 mmHg. During the study this was 152 ±18 and 81 ±12 mmHg. Hypotensive episodes occurred 11 times in 7 patients before start of the study, and 12 times in 7 patients during the study. Body weight, appetite, handgrip strength, serum phosphate: those values did not differ statistically significant between baseline and final measurements.
DISCUSSION
This study shows that both malnourished and well-nourished hemodialysis patients consume insufficient protein and energy on days of dialysis. Mean protein and energy intake increases with 18 grams of protein and 264 kcal per dialysis day after intervention with a protein and energy-enriched in-between meal and education about protein intake. On average, 12 grams of protein and 175 kcal is provided by the in-between meals. Several randomized trials, based on different nutritional interventions, showed similar results, but without the use of normal food [5, 6, 17, 18]. Inadequate protein intake is mainly due to the increased protein requirement, while appetite is not increased. An explanation could be that metabolic changes of the kidney disease and the dialysis procedure itself results in an average increase in protein requirement of 0.4 g/kg compared to healthy people [19]. On average 6-8 grams of protein per dialysis treatment is lost in the dialysate during each dialysis treatment [19]. Also inflammation, due to contact of blood with the dialysis membrane, results in a negative nitrogen balance. Studies about nitrogen balance in stable hemodialysis patients show that patients become catabolic when the protein intake is less than 0.8 g/kg [20, 21]. Additional protein and energy enriched in-between meals have the potential to restore protein and energy balances when muscles are broken down in order to maintain amino acid plasma values and to promote the synthesis of acute phase proteins. A study by Veeneman et al. showed that by consuming a high protein and energyenriched meal, the protein balance changed from a negative protein balance during fasting to a positive protein balance after the energy-enriched meals [22]. Pupim et al. showed that additional administration of oral feeding during dialysis or providing nutrients directly into the blood circulation (intradialytic parenteral nutrition, IDPN) causes a positive nitrogen balance and an improvement in muscle protein homeostasis [22, 23]. The benefit of oral nutrition instead of IDPN was that the anabolic effects of IDPN in the blood circulation disappeared in the period after the dialysis while the effect of oral feeding remained [23, 24]. In our intervention study no effect is found on post-dialysis weight and handgrip strength. Since inflammation can influence serum albumin, this parameter has not been determined as a marker of nutritional status. However, an improvement in nutritional status or other clinical parameters in malnourished hemodialysis patients was found using oral supplements during dialysis.2 Improvement is found in subjective global assessment protein intake, quality of life, reduced inflammation and improved physical function, mortality [25-30]. A positive effect on survival in hemodialysis patients has been demonstrated with a higher protein intake, in patients with more fat mass and more muscle mass [17]. Energy deficiency during dialysis can have a large effect on body weight progress since hemodialysis patients dialyze for years. Patients lose on average 3 kg of body weight in the first 3 years of dialysis treatment if no nutritional support is provided [31, 32]. Our study, showed that protein and energy requirements can be achieved with additional protein and energy-enriched in-between meals. As expected no effect on body weight was found, possibly due to the limited duration of the study. An extra 264 kcal per dialysis day was consumed, which theoretically means an increase in fat mass of 2.6 kg after one year. No effect on handgrip strength was found in our study. Literature showed that a higher protein and energy intake may lead to an improvement of handgrip strength and functional status [19]. Handgrip strength is an indicator of the muscle function and is related to the total body muscle mass. A loss of 10% muscle protein will lead to reduced muscle strength. Indirectly it provides an impression of malnutrition. Qureshi et al. and Stenvinkel et al. found significantly lower handgrip strength in patients who were assessed as malnourished by the SGA [33]. In several studies a significant positive relationship between handgrip strength and lean body mass (protein mass) measured by DXA was found [33]. A possible explanation could be that the duration of 6 weeks is too short to demonstrate a difference, and that an increase of 18 grams of protein intake per day of dialysis treatment might not be enough. Our study included a limited number of patients in comparison with other studies. Postprandial hypotension is one of the reasons for some, why meals during dialysis are not prescribed [34]. In our study, hypotensive episodes where measured before and during the study. No difference was found in hypotensive episodes, thus postprandial hypotension was not provoked during intervention with in-between meals [35]. Serum phosphate did not increase significantly after the intervention period of 6 weeks with the protein (phosphate rich) and energy-enriched in-between meals. An explanation could be the attention for the intake of phosphate binders. Phosphate binders were also provided when patients forgot them. This is also found in the FrEDI study where no extreme rise of serum phosphate was shown after eating a protein-enriched meal during dialysis together with a phosphate binder. Hyperphosphatemia contributes to the development of vascular calcifications, which increases the risk of cardiovascular morbidity. Prevention is also possible by reducing foods high in phosphate. However, these foods also contain a lot of protein. Research shows that hemodialysis patients with lower serum phosphate level can reach a better prognosis by correctly taking their medicines and a higher protein intake compared to a low serum phosphate- and low protein intake [2, 5, 36]. Appetite of the patients was good at baseline and after six weeks. Patients ate more by providing additional in-between meals and education on protein. The attention to nutrition, inbetween meals and the "luxury" of being offered something extra during dialysis might stimulate to eat more and better. During our study, patients were offered 7 different in-between meals. The "ordinary" foods and drinks were consumed most, instead of the oral supplements. However this study has some limitations. The study groups were small and possibly not representative of the entire dialysis population. It is not certain that results are due to the intervention because there was no control group. Also the 24- hour recall method could cause biased results, however differences between pre- and post-assessment would be expected to be less biased. Because the normalized Protein Nitrogen Appearance (nPNA) has not been determined in all patients, this could not be compared with the data of the 24 hour recall.
CONCLUSION
Most of the hemodialysis patients consume inadequate amount of protein and energy on dialysis days. This study shows that the protein and energy intake can be improved by providing a protein and energy-enriched in-between meal (15 grams of protein and 240 kcal) during dialysis treatment and education. Rich in protein and energy in-between meals should be part of the assortment of food in dialysis wards.
ACKNOWLEDGEMENTS
The authors thank Tessa Slieker, Mariska Koolen, Najoua Zanaki, and Maryam Hdoudoe for their help with this study.
DISCLOSURE AND FUNDING
There are no potential financial conflicts of interest for each author. The Dutch Kidney Foundation has provided financial support in writing the report.
REFERENCES
- Fouque D, Kalantar-Zadeh K, Kopple J, Cano N, et al. (2008).A proposed nomenclature and diagnostic criteria for proteinenergy wasting in acute and chronic kidney disease. Kidney Int. 73(4), 391- 398.
- Kalantar-Zadeh K and Ikizler TA. (2013). Let them eat during dialysis: An overlooked opportunity to improve outcomes in maintenance hemodialysis patients. J Ren Nutr. 23(3), 157-163.
- Mak RH, Ikizler AT, Kovesdy CP, Raj DS, et al. (2011). Wasting in chronic kidney disease. Journal of Cachexia, Sarcopenia and Muscle. 2(1), 9-25.
- Avesani CM, Draibe SA, Kamimura MA, Colgnati FAB, et al. (2004). Resting energy expenditure of chronic kidney disease patients: influence of renal function and subclinical function. Am J Kidney Dis. 44(6), 1008-1016.
- Shinaberger C, Greenland S, Kopple J, Wyck van D, et al. (2008). Is controlling phosphate by decreasing dietary protein intake beneficial or harmful in persons with chronic kidney disease? Am J Clinical Nutrition. 88(6), 1511-1518.
- Sharma M, Rao M, Jacob S and Jacob CK. (2002). A controlled trial intermittent enteral nutrient supplementation in maintenance hemodialysis patients. J Ren Nutr. 12(4), 229-237.
- Kistler BM, Fitschen PJ, Ikizler A and Wilund KR. (2015). Rethinking the ristriction of nutrition during hemodialysis treatment. J Ren Nutr. 25(2), 81-87.
- Struijk-Wielinga GI, Zanaki N, Hdoudoe M and Weijs PM. (2012). Is protein-energy intake adequate during dialysis treatment in hemodialysis patients? Kidney Res Clin Pract 31, A76, 235.
- Nevo-online.rivm.nl version 2011/3.0.
- Fouque D, Vennegoor M, Ter Wee P, Wanner C, et al. (2007). EBPG Guideline on Nutrition. Nephrol Dial Transplant. 22(suppl 2), ii45-ii87.
- Dietitians Nephrology in the Netherlands. (2011). Guideline diet for hemodialysis.
- Weir JB. (1949). New methods for calculating metabolic rate with special reference to protein metabolism. J Physiol. 109(1-2), 1-9.
- Roza AM and Shizgal HM. (1984). The Harris and Benedict equation reevaluated: Resting energy requirements and the body cell mass. Am J Clin Nutr. 40(1), 168-182.
- Flint A, Raben A, Blundell JE and Astrup A. (2000). Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int Journ of Obesity. 24(1), 38-48.
- Steiber AL, Kalantar-Zadeh K, Secker D, Mc Carthy M, et al. (2004). Subjective global assessment in chronic kidney disease: a review. JRenNutr. 14(4), 191-200.
- Mathiowetz V, Kashman N, Volland G, Weber K, et al. (1985). Grip and pinch strenght: normative data for adults. Arch Phys Med Rehabil. 66(2), 69-74.
- Rocco MV, Paranandi L, Burrowes JD, Cockram DB, et al. (2002). Nutritional Status in the HEMO Study Cohort at Baseline. Am J of Kidney Diseases. 39(2), 245- 256.
- Burrowes JD, Larive B, Cockram DB, Dwyer J, et al. (2003). Effects of dietary intake, appetite and eating habits on non-dialysis treatment days in hemodialysis patients: cross sectional results from the HEMO Study. J Ren Nutri. 13(3), 191-198v
- Kalantar-Zadeh K, Cano N, Budde K, Chazot C, et al. (2011). Diets and enteral supplements for improving outcomes in chronic kidney disease. Nat. Rev Nephrol. 7(7), 369-384.
- Rao M, Sharma M, Juneja R, Jacob S, et al. (2000). Calculated nitrogen balance in hemodialysis patients: influence of protein intake. Kidney Int. 58(1), 336-345.
- Ikizler TA, Pupim LB, Brouilette JR, Levenhagen DK, et al. (2002). Hemodialysis stimulates muscle and whole body protein loss and alters substrate oxidation. Am J Physiol Endocrinol Metab. 282(1), E107-E116.
- Veeneman JM, Kingma HA, Boer TS, Stellaard F, et al. (2003). Protein intake during hemodialysis maintains a positive whole body protein balance in chronic hemodialysis patients. Am J Fysio Endocrinol Metab. 284(5), E954-E965.
- Pupim LB, Majchrzak KM, Flakoll PJ and Ikizler TA. (2006). Intradialytic oral nutrition improves protein homeostasis in chronic hemodialysis patients with deranged nutritional status. J Am Soc Nephrol. 17(11), 3149-3157.
- Pupim LB, Flakoll PJ, Brouilette JR, Levenhagen DK, et al. (2002). Intradialytic parenteral nutrition improves protein and energy homeostasis in chronic hemodialysis patients. J Clin Invest. 110(4), 483-492.
- Caglar K, Fedje L, Dimmitt R, Hakim RM, et al. (2002). Therapeutic effects of oral nutritional supplementation during hemodialysis. Kidney Int. 62(3), 1054-1059.
- Cano NJ, Fouque D, Roth H, Aparicio M, et al. (2007). Intradialytic parenteral nutrition does not improve survival in malnourished hemodialysis patients: a 2-year multicenter, prospective, randomized study. J Am Soc Nephrol. 18(9), 2583-2591.
- Moretti HD, Johnson AM and Keeling-Hathaway TJ. (2009). Effects of protein supplements in chronic Hemodialysis and Peritoneal Dialysis patients. J Ren Nutr. 19(4), 298-303.
- Scott MK, Shah NA, Vilay AM, Thomas J 3rd, et al. (2009). Effects of peridialytic oral supplements on nutritional status and quality of life in chronic hemodialysis patients. J Ren Nutr. 19(2), 145-152.
- Tomayko EJ, Brandon MK, Fitschen PJ and Wilund KR. (2015). Intradialytic protein supplementation reduces inflammation and improves Physical Function in maintenance hemodialysis patients. J Ren Nutr. 25(3), 276-283.
- Lacson E Jr, Ikizler A, Lazarus JM, Teng M, et al. (2007). Potential impact of nutritional intervention on end-stage renal disease hospitalization, death, and treatment costs. J Ren Nutr. 17(6), 363-371.
- Weiner DE, Tighiouart H, Ladik V, Meyer KB, et al. (2014). Oral intradialytic nutritional supplement use and mortality in hemodialysis patients. Am J Kidney Dis. 63(2), 276-285.
- Rocco MV, Dwyer JT, Larive B, Green T, et al. (2004). The effect of dialysis dose and membrane flux on nutritional parameters in hemodialysis patients. Results of the HEMO Study. Kid Int. 65(6), 2321-2134.
- Leal VO, Mafra D, Foque D and Anjos LA. (2010). Use of handgrip strength in assessment of the muscle function of chronic kidney disease patients on dialysis: a systematic review. Nephrol Dial Transplant.1-6.
- Kistler B, Benner D, Burgess M, Stasios M, et al. (2014). To eat or not to eat - International experiences with eating during hemodialysis treatment. J Ren Nutr. 24(6), 349-352.
- Shibagaki Y and Takaichi K. (1998). Significant reduction of the large-vessel blood volume by food intake during hemodialysis. Clin Nephrol. 49(1), 49-54.v
- Fouque D, Horne R, Cozzolino M and Kalantar-Zadeh K. (2014).Balancing Nutrition and Serum Phosphate in Maintenance Dialysis. Am J Kidney Dis. 64(1), 143-150.