Previous Issues Volume 1, Issue 2 - 2016
A Very Rare Case Report of Pleomorphic Adenoma of the Base of the Tongue With 15 Years Follow-Up: A Review Of Literature
Paolo Roberto Ordesi1, Luca Pisoni1, Paolo Siervo2, Pierluigi Nannei1 Roberto Giardini3, Andrea Edoardo Bianchi4, Sandro Siervo1
1Maxillofacial Surgery Unit, Istituto Stomatologico Italiano, via Pace 21, Milan.
2Private Practice, Milan
3Anatomical Pathology Unit, Policlinico di Monza, via Amati 111, Monza.
4Department of Periodontology, Istituto Stomatologico Italiano, via Pace 21, Milan.
Corresponding Author: Paolo Roberto Ordesi, Maxillofacial Surgery Unit, Istituto Stomatologico Italiano, via Pace 21, Milan. Tel: +39 02.5513071; Email: [email protected]
Received Date: 03 Mar 2016 Accepted Date: 18 Apr 2016 Published Date: 25 Apr 2016 Copyright © 2016 Ordesi PR.
Citation: Ordesi PR, Pisoni L, Siervo P, Nannei P, et al. (2016). A Very Rare Case Report of Pleomorphic Adenoma of the Base of the Tongue With 15 Years Follow-Up: A Review Of Literature. Mathews J Dentistry. 1(1): 007.
ABSTRACT
The mixed benign tumour, or pleomorphic adenoma, is the most common tumour affecting salivary glands. In the oral cavity, the predominant localization of this kind of tumours is the palate, followed by the upper lip and the cheek mucosa. The localization at the base of the tongue is extremely rare. Clinically they appear as compact asymptomatic formations. The diagnosis of these tumours is placed on the basis of histopathological features. The first-line treatment of benign this kind of tumour is surgical excision. In 1999 a woman aged 38, came to our attention reporting the presence since a few months of a roundish mass at the level of the body of the tongue. A surgical enucleation of the mass was performed, and an histological diagnosis of pleomorphic adenoma was made. The patient has been inserted in a program of follow-up. During the observation period (15 years) recurrence of the lesion was not observed.
KEYWORDS
Dental Health; Oral Health; Schizophrenia; Periodontal; Dental Hygiene; Dental education.
INTRODUCTION
The mixed benign tumour, or pleomorphic adenoma, is the most common tumour affecting salivary glands. Chaudhary et al pointed out that the pleomorphic adenoma represents almost 56% of intraoral minor salivary glands tumours [1]. In 85% of cases, it affects the parotid gland, while the submandibular gland and other minor salivary glands respectively in 8% and 7% of the cases [2-5].
The pleomorphic adenoma of the base of the tongue is a rare tumour, which has a multiform origin from epithelial and connective tissues: the originating cells are the myoepithelial cells interposed with the ductal cells [6].
As shown in table 1, the international literature has reported a very low number of cases of pleomorphic adenoma involving the tongue. Patients ranged from 19 months to 87 years of age. Male:female ratio was 4:15, including this case. In all cases the treatment adopted was the surgical excision. In only 1 case, in addition to surgery, radiotherapy was included [7]. The follow-up period, when specified, ranged from 3 months to 25 years (Table1).
Table 1: Literature cases of pleomorphic adenoma of the tongue reported by literature.
| Author/year | n° Cases | Location | Size | Sex | Age (years) | Surgical Approach | Follow-up |
|---|---|---|---|---|---|---|---|
| Goepfert 1976 | 1 | NA | NA | W | 39 | intraoral + RT | NA |
| Grewal 1984 | 1 | NA | 4 | W | 35 | intraoral | NA |
| Deitmer 1985 | 1 | NA | 2 x 3 | M | 29 | intraoral | NA |
| Banerjee 1987 | 1 | NA | 2 x 3 | M | 32 | intraoral | NA |
| Magliulo 1996 | 1 | NA | 2 x 3 | W | 32 | intraoral | NA |
| Gupta 1997 | 1 | NA | 1,75 x 2,53 | W | 50 | intraoral | NA |
| Bayles 1999 | 1 | right side | NA | W | 19 months | intraoral | 16 months |
| Yoshihara 2000 | 1 | base | 2 x 3 | W | 87 | intraoral | NA |
| Jorge 2002 | 1 | base | NA | W | 18 | intraoral | 25 years |
| Berry 2004 | 1 | base | 2 x 2 | W | 66 | intraoral | NA |
| Tanigaki 2004 | 1 | lateral side | NA | W | 54 | intraoral | NA |
| Vaamonde 2004 | 1 | base | NA | M | 42 | intraoral | 7 years |
| Virk 2005 | 1 | right side and left side | NA | M | 38 | intraoral | 3 MONTHS |
| El Kohen 2007 | 1 | base | NA | W | 70 | intraoral | NA |
| Gupta 2007 | 1 | base | NA | W | 52 | intraoral (mandibulotomy) | 1 Year |
| Ghosh 2011 | 1 | base | 2 x 2,5 | W | 40 | intraoral | 6 months |
| Bansal 2012 | 1 | base | 3 x 3 | W | 24 | intraoral | NA |
| Nascimento 2014 | 1 | NA | 8 x 8 | W | 55 | extraoral | NA |
| Ordesi 2015 | 1 | base | 1,5 x 1 | W | 38 | intraoral | 15 years |
The histogenesis of this tumour is related to the proliferation of cells which resemble the ductal and/or myoepithelial ones. The presence of a differentiated myoepithelial cell is important in order to define the composition and the aspect of mixed tumors [8]. Most of the studies show the presence of different cell types in mixed tumours; the epithelial tumours occupy one end of the spectrum, and the myoepithelial ones the other [9]. Between these two ends, more undifferentiated types are present, with both myoepithelial and ductal features [10]. It was hypothesized that this tumour origins from a single cell which can differentiate both in epithelial and myoepithelial sense, rather than from the simultaneous growth of epithelial and myoepithelial cells.
Mixed tumours can develop at every age, while they affect mainly female patients, with an incidence 3-4 times higher in female than male patients, and occur mainly between the fourth and the sixth decade of life [11]. Generally, these tumours are mobile, with the exception of the localizations on the palate [12]. Clinically they appear as compact asymptomatic formations, and in most cases the overlying mucosa is not ulcerated.
From a histopathological point of view, mixed tumours show a typical proteiform histopathological context, which explathe synonymous of pleomorphic adenoma, which these tumours are also called by, as composed by tissues of both epithelial and mesenchymal origin, intermingled in a variable proportion in each case (in 1/3 of cases the components are equal). Considering the predominant component, some authors subdivide these neoplasms in: cellular type (predominance of epithelial component) and myxoid type (composed mainly of myxoid or myxochondroid substance), the latter more frequent than the previous [13].
The epithelial component, also in the minor salivary glands tumours, includes different types of cells: spindle-shaped, clear, squamous, basaloid, cuboidal, plasmacytoid, oncocytoid, mucous and sebaceous. These cells are organized in a variety of architectural configurations: trabecular, ductal, tubular, cystic [14-17].
The mesenchymal component, often interposed to the epithelial one up to isolate single elements, is composed of myxoid, ialine, chondroid (consisting of heparan-e chondroitinsulphate and by protease inhibitors, which confer antiinvasive properties), osseous, and more rarely of lipomatous areas [18]. In a percentage varying from 1,5% to 1,5% a 21% the literature reports the presence of crystalloid structures, radial- or petal-arranged, probably due to the precipitation of the collagen of the epithelial stromal component.
The interface between the tumor and the surrounding salivary parenchyma is usually well defined, and is often highlighted by a fibrous pseudocapsule, rarely present, however, in tumours of minor salivary glands. Islands of neoplastic glandular tissue, or satellite nodules are usually detectable especially in sections of the serial sampling of the tumour, and must not be considered as neoplastic invasion [1]. Focal necrosis, hypercellularity, hyperchromasia and nuclear polimorphism, mitotic index increased and an extended hyalinization can be considered as malignant transformation of the tumor, but the predictive value for that evolution has been proven only for an extended hyalinization, which is accompanied by a focal hypocellularity [19-21].
By its nature, the pleomorphic adenoma arises in differential diagnosis with numerous benign entities (myoepithelioma, canalicular adenoma) and malignant (low grade pleomorphic adenocarcinoma, myoepithelial carcinoma, epithelial-myoepithelial carcinoma, mucous adenocarcinoma, adenoid cystic carcinoma, carcinoma in pleomorphic adenoma), from which it can be differentiated by some morphological features, while immunophenotypic methods are of little help. In minor salivary glands the most difficult differential diagnosis is the one with the low-grade pleomorphic carcinoma, often restricted and characterized by myxoid areas with bland cytological appearance: the evaluation of perineural growth and the formation of tubular structures which is absent in the mixed tumour is mandatory for differential diagnosis.
The diagnosis of these tumours is placed on the basis of histopathological features. The incisional biopsy gives the pathologist a better chance of diagnosis compared with fine needle aspiration, without increased morbidity [22]. Radiographic and CT instrumental particularly magnetic resonance imaging (MRI) provide information on the nature of the injury, the extent and possible involvement of the surrounding structures. The MRI is preferable because of its better resolution of soft tissue [5].
The first-line treatment of benign mixed tumour of the major and minor salivary glands is surgical excision. The enucleation as a primary mode increases the chances of recurrence4. Inadequate removal of the tumour hampers results in the appearance of a relapse, often characterized by multiple tumour foci. Recurrences usually are localized at the site of a previous intervention and can be associated with a surgical scar [23]. To avoid the appearance of recurrences must first follow a proper surgical treatment at an early stage. In many cases, relapses have the same histological characteristics of the primary tumour but are often associated with a high risk of malignant transformation [24]. About 25% of benign mixed tumours, if left untreated, undergo malignant transformation. The probability of a malignant transformation also increases if the area has been previously treated surgically or with radiotherapy.
CASE REPORT
In April 1999 a woman aged 38, is referred to our ward with negative history for important familiar diseases, non-smoker, with a good oral hygiene. The physical examination showed, at the lower dental arch, the presence of an amalgam reconstruction at 3.6, a ceramic inlay reconstruction at 3.7, a metal ceramic crown at 4.6, and a single implant supported crown in position 3.1. There weren't any pathological probings and BoP was negative. At the level of the body of the tongue, in a ventral left position a roundish mass was present of hard-elastic texture, not aching, neither spontaneously nor at palpation. Patient refers the appearance of the lesion since a few months and a limitation to the common tongue movements due to the increasing bulk of the mass (Figure 1).

Figure 1:Clinical presentation of the case. A round mass was present on the ventral left side of the tongue.
The common radiological and instrumental investigations didn't show the presence of abscess lesions or calculi. We decided for the surgical enucleation of the mass with histological examination for a certainty diagnosis.
After infiltration of local anaesthetic (UBISTESIN, 3M/ESPE, Seefeld, Germany) at the level of the ventral side of the body and the tip of the tongue, a median incision of the mucosa is performed. A submucosal layer dissection by blunt scissors is performed, until the neoformation, which appears well encapsulated, is completely isolated (Figure 2). After having it separated from the deep layers, the tumour is removed (Figure 3), and the wound sutured at different layers with resorbable filament 4-0 and 5-0 (Vicryl, Ethicon Inc., Somerville NJ, USA).
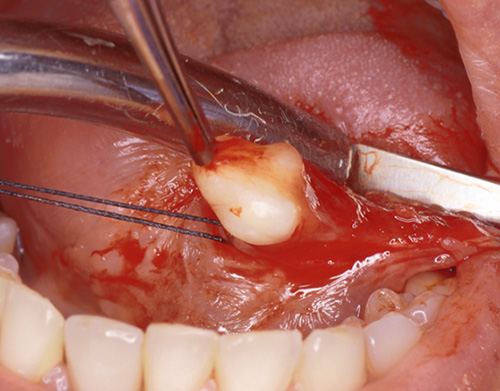
Figure 2: Surgical enucleation of the tumour.
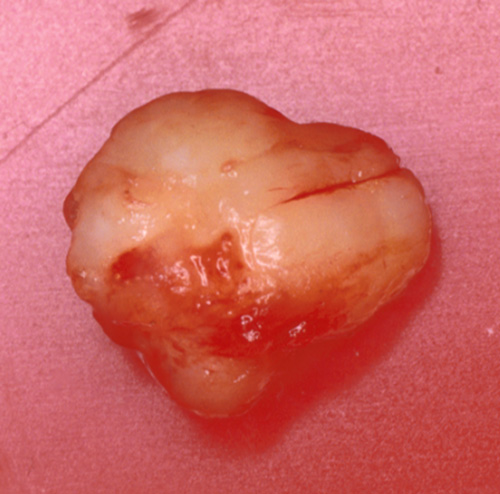
Figure 3: The resected tumour.
The tumour is immediately fixed in buffered formalin and sent for histological examination, which puts diagnosis of pleomorphic adenoma (Figure 4).
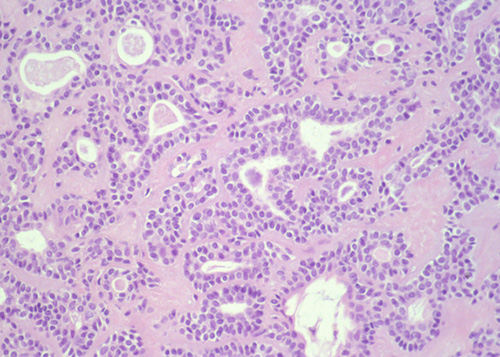
Figure 4: Histological sample of the tumour. The diagnosis of pleomorphic adenoma was confirmed.
The patient, made aware of the nature of the lesion, is inserted in a program of follow-up controls every 6 months. Clinically, during the observation period (15 years) recurrence of the lesion was not observed, although the tissutal "blending" in the operated area has never returned to normal if compared to the healthy zone (Figure 5).

Figure 5: Intraoral situation 15 years post-surgery. No signs of recurrence have occurred.
REVIEW OF LITERATURE
As shown in table 1, the international literature has reported a very low number of cases of pleomorphic adenoma involving the tongue.
Patients ranged from 19 months to 87 years of age. Male:female ratio was 4:15, including this case. In all cases the treatment adopted was the surgical excision. In only one case, in addition to surgery, radiotherapy was included [8]. The follow-up period, when specified, ranged from 3 months to 25 years (Table 1).
Mixed tumours can develop at every age, while they affect mainly female patients, with an incidence 3-4 times higher in female than male patients, and occur mainly between the fourth and the sixth decade of life [13]. Generally, these tumours are mobile, with the exception of the localizations on the palate [12]. Clinically they appear as compact asymptomatic formations, and in most cases the overlying mucosa is not ulcerated
As reported by the literature, surgical excision is the treatment of choice for the pleomorphic adenoma enucleation. The complete enucleation diminishes the recurrence rates [5]. According to tumour dimensions, the surgical approach can be: intraoral, median transhyoid and lateral with pharyngotomy [8].
If possible, the treatment of choice is the intraoral, for a minor morbidity and the absence of scars. The tumour resection with a transhyoid approach and pharyngotomy allows a relevant higher possibility of radicalization, with a statistically lower recurrence rate. It is clear that this approach is more invasive. The choice for an intraoral approach (just like recommended by the literature) in patients who can undergo a strict follow-up control program, can be a suitable option. Our patient was subjected to 6 months scheduled controls, and the clinical success 15 years later has been warranted.
Thanks to the early surgical treatment, there wasn't neither malignant transformation, nor recurrence of the tumour.
REFERENCES
- Chaudhary AP, Viekers RA and Gorlin RJ. (1961). Intraoral minor salivary gland tumours. An analysis of 1,414. Oral Surgery 14, 1194-1226.
- Eveson JW and Cawson RA. (1985). Salivary gland tumors. A review of 2,140 cases with particular reference to histologic types, site, age, and sex distribution. J Pathol. 146, 51-58.
- Crippa R, Angiero F and Passoni E. (2005). Pleomorphic adenoma of the hard palate. The Modern Dentist. 119-123.
- Berry S, Tay H and Puentes CP. (2004). Pleomorphic adenoma of the base of the tongue. Ear Nose Throat J, 83(9), 646-648.
- Virk RS and Hundal H. (2005). Bilateral pleomorphic adenoma of the anterior tongue: a case report. Ear, Nose & Throat J. 84(12), 789-790.
- Tangaki Y, Mikami Y, Ono M, Tsukuda M, et al. (2004). Pleomorphic adenoma of the lateral side of the tongue. Case Report. Acta Otolaryngol. 124, 649-651.
- Goepfert H, Giraldo AA, Byers RM, Luna MA, et al. (1976). Salivary gland tumors of the base of the tongue. Arch Otolaryngol. 102(7), 391-395.
- Yoshihara T and Suzuki S. (2000). Pleomorphic adenoma of tongue base causing dysphagia and dysphasia. J Laryngol Otol. 114(10), 793-795.
- Handa U, Dhingra N, Chopra R, Mohan H, et al. (2008). Pleomorphic adenoma: Cytologic variations and potential diagnostic pitfalls. Diagn Cytopathol. 37(1), 11-15.
- Cheuk W and Chan JKC. (2007). Advances in salivary gland pathology. Histopathology. 51(1), 1-20.
- Banerjee S. (1987). Benign pleomorphic adenoma of the base of the tongue. J R Coll Surg Edinb. 32, 164-165.
- Enorth CM, Hjertman K and Moberger G. (1972). Salivary gland adenomas of the palate. Acta Otolaryngologica. 73, 305-315.
- Seifert G, Langrock I and Donath K. (1976). Pathomorphologische Subklassifikation der pleomorphen Spreicheldruesenadenome. Analyse von 310 Parotisadenomen. 24, 415-426.
- Geopfert H, Giraldo AA, Byers R, Luna M, et al. (1976). Salivary gland tumours of the base of the tongue. Arch Otolaryngol 1076(102), 391-395.
- Feinmesser M, Feinmesser R, Okon E, Freeman JL, et al. (1993). A monomorphic adenoma of the minor salivary glands presenting at the base of the tongue: a case report and review of the literature. Journal of Otology. 22(2), 110-112.
- Clark SK and Yarington CT. (1980). Lingual malignant disease of minor salivary gland origin. American Journal of Otolaryngology. 1, 181-185.
- Goldblatt LI and Ellis GL. (1987). Salivary gland tumours of the tongue: analysis of 55 new cases and review of literature. Cancer. 60(1), 74-81.
- Sternlicht MD, Safrians S, Rivera SP, Barsky SH, et al. (1996). Characterizations of the extracellular matrix and proteinaseinhibitor content of human myoepithelial tumors. Lab Invest. 74, 781-796.
- Main JH, Orr JA, McGurk FM, McComb RJ, et al. (1976). Salivary gland tumours: review of 643 cases. Journal of Oral Pathology 5(2), 88-102.
- Burbank PM, Dockerty MB and Devine KD. (1959). A clinicopathology study of 43 cases of glandular tumours of the tongue. Surgery Gynecology Obstetrics. 109, 573-582.
- Lewis JE, Olsen KD and Sebo JJ. (2001). Carcinoma ex pleomorphic adenoma: pathologic analysis of 73 cases. Hum Pathol. 32, 596-604.
- Grewal DS, Pusalkar AG and Phatak AM. (1984). Pedunculated pleomorphic adenoma of the tongue base manifesting with dyspnea: A case report. J Laryngol Otol. 98(4), 425-427.
- Hong KW and Yang YS. (2008). Intraoral approach for the treatment of submandibular salivary gland mixed tumors. Oral Oncol. 44, 491-495.
- Spiro RH. (1986). Salivary neoplasm: Overview of a 35-year experience with 2,807 patients. Head Neck Surg. 8(3), 177-184.